
Abstract
This is a cross-sectional study investigating the prevalence and nature of trauma-informed care (TIC) training in obstetrics and gynecology residency programs. In our sample, 20% of programs had annual TIC training, 53% had less than annual training, and 27% had no training at all. Only 25.3% of respondents were satisfied with their current training in interpersonal trauma and TIC. A lack of facilitators to conduct such training was the primary barrier to implementing TIC. Significant opportunity exists to improve TIC education for Ob/Gyn trainees.
Introduction
Interpersonal trauma affects the lives of millions, and may occur at the level of the individual (domestic violence, sexual or physical assault), the community or society at large (collective trauma, such as racism, sexism, xenophobia, homophobia, and historic or structural trauma; Huang et al., 2014). Nearly 61% of Americans experience childhood trauma, either through personal abuse, neglect, or household dysfunction, such as domestic violence, mental illness, or imprisonment of a family member (Lanius et al., 2010). One in three women and one in six men experience sexual violence at some point in their lives (Breiding, 2015). Trauma significantly affects marginalized populations: in a large systematic review, individuals who identify as transgender were on average 2.5 times more likely to report having experienced sexual violence compared to cis-gender respondents in the same study (Peitzmeier et al., 2020). Trauma experienced in childhood results in a higher risk of severe obesity, 20% increased risk of hypertension, an 80% increase in heavy drinking, a 430% increase in risky sexual behavior, a 500% increase in depression, a 320% increase in disability, and is associated with a higher prevalence of chronic pelvic pain (Campbell et al., 2016; Dugan et al., 2023; Felitti, 2009; Garza-Leal et al., 2021; Riley et al., 2010).
Trauma-informed care (TIC) refers to a paradigm of clinical practice in which the clinician approaches each patient encounter with an understanding of the social and health effects of trauma, developing a safe environment built on trust and transparency to minimize retraumatization and improve healthcare outcomes (Infield & Boswell, 2020). TIC is intended to be applied universally and is not predicated on knowledge or documentation of an individual's personal experiences of trauma. TIC principles have been taught to healthcare providers within the fields of Pediatrics, Family Medicine, and Internal Medicine, and only recently in Obstetrics and Gynecology (Ob/Gyn) (Dichter et al., 2018; Marsac et al., 2016; Schiff et al., 2017; Shamaskin-Garroway et al., 2017; Stevens et al., 2020). Obstetrician-gynecologists in particular should be prepared to care for survivors of sexual assault and interpersonal trauma given that these Ob/Gyn visits are often a patient's only entrance into or interaction with the medical system for much of their reproductive lives. Furthermore, a successful Ob/Gyn physician–patient interaction requires the transfer of very sensitive medical information as well as very personal breast and pelvic exams. Without a trauma-informed approach, Ob/Gyn visits may trigger or retraumatize the patient, and may also cause trauma. Indeed, prior studies of patient testimonies report that this retraumatization is experienced specifically during Ob/Gyn clinical encounters (Ackerson, 2012; Coles & Jones, 2009; Hilden et al., 2003; Hobbins, 2004; Kohler et al., 2021; Leeners et al., 2007; Sobel et al., 2018; Weitlauf et al., 2008, 2010; White et al., 2016).
Despite the magnitude of this problem, TIC is not a required aspect of Ob/Gyn training and was not acknowledged until the summer of 2020, upon the release of the latest edition of the educational objectives put forth by the Council on Resident Education in Obstetrics & Gynecology (CREOG; Council on Resident Education in Obstetrics and Gynecology, 2020). This document is meant to inform residency programs of their curriculum requirements and adds TIC as a recommended objective for the first time. In 2016, The American College of Obstetricians and Gynecologists (ACOG) published a Committee Opinion that encouraged providers to screen for a history of sexual assault, and in 2019 this document was updated to suggest that clinicians incorporate a TIC framework when caring for sexual assault survivors (Sexual Assault: ACOG Committee Opinion No. 777, 2019). In 2021, ACOG released a separate Committee Opinion specifically about caring for patients who have experienced trauma (Caring for Patients Who Have Experienced Trauma: ACOG Committee Opinion, Number 825, 2021). It is a resource for general Ob/Gyns to familiarize themselves with what trauma and TIC are, however, there still is no standardized curriculum on how to train Ob/Gyn residents to care for patients who disclose a sexual assault or trauma history.
In order to understand the gap in knowledge around TIC training in Ob/Gyn, we conducted a survey of Ob/Gyn residency programs to describe the availability, frequency, and content of current TIC curricula, and to determine the need for and components of further curriculum development.
Materials and Methods
This cross-sectional study identified eligible participants using the electronic database of residency program directors (PDs) maintained on the Association of Professors of Gynecology and Obstetrics (APGO) website to identify all Ob/Gyn residency programs in the United States and Canada (APGO, 2019). We sent an initial email in September 2019 to all PDs describing study objectives and methods. A link to the Qualtrics Survey Software survey was embedded within the email, and consent was affirmed by clicking this hyperlink. The survey was anonymous, though respondents were given the opportunity to provide their email addresses if they wanted to receive the results of the survey. Three reminder emails were sent a week apart for a total recruitment invitation period of 1 month. No compensation was offered. This study #2019P001373 was approved by the Partners Healthcare Institutional Review Board on 7/9/2019.
Since we could find no prior literature to evaluate training curricula in TIC, we developed our own survey instrument. To do this, we created a multidisciplinary team of TIC experts including academic Ob/Gyn physicians who regularly teach TIC principles (DB, CR, and CD), a trauma and posttraumatic stress disorder (PTSD) expert social worker who serves as the Chair of the Mass General Brigham (MGB) TIC Education and Training Committee (SG) and the founder of the MGB Coordinated Approach to Resilience and Empowerment clinic for trauma victims and survivors (ALO). Thirty-six survey elements captured program characteristics (location by ACOG district, number of residents, number of clinical sites, affiliation with a medical school, affiliation with a religious organization), characteristics of any current training on caring for patients with histories of assault, resident evaluation of such training, and any barriers to providing this training. Lastly, respondents were queried about specific components of a hypothetical “yet-to-be-developed” TIC curriculum that the PD would consider for their specific residency program. The survey was designed to be completed within 10 min.
Qualtrics Survey Software data were exported to Stata 15.0 for analysis. As an exploratory assessment, descriptive statistics (mean, median, range, and frequencies) and 95% confidence intervals were computed for each outcome.
Results
Of the 275 programs solicited, 92 responded with a response rate of 33.5%. Table 1 summarizes the responding program characteristics, with the majority being affiliated with a medical school and having more than one clinical site, and the minority being affiliated with a religious organization. Residency programs from all regions of the United States and Canada were represented. There was also a wide range of program sizes represented in this sample but the median number of residents reported was 20 (IQR: 16–25).
Characteristics of Programs Represented by Survey Respondents.
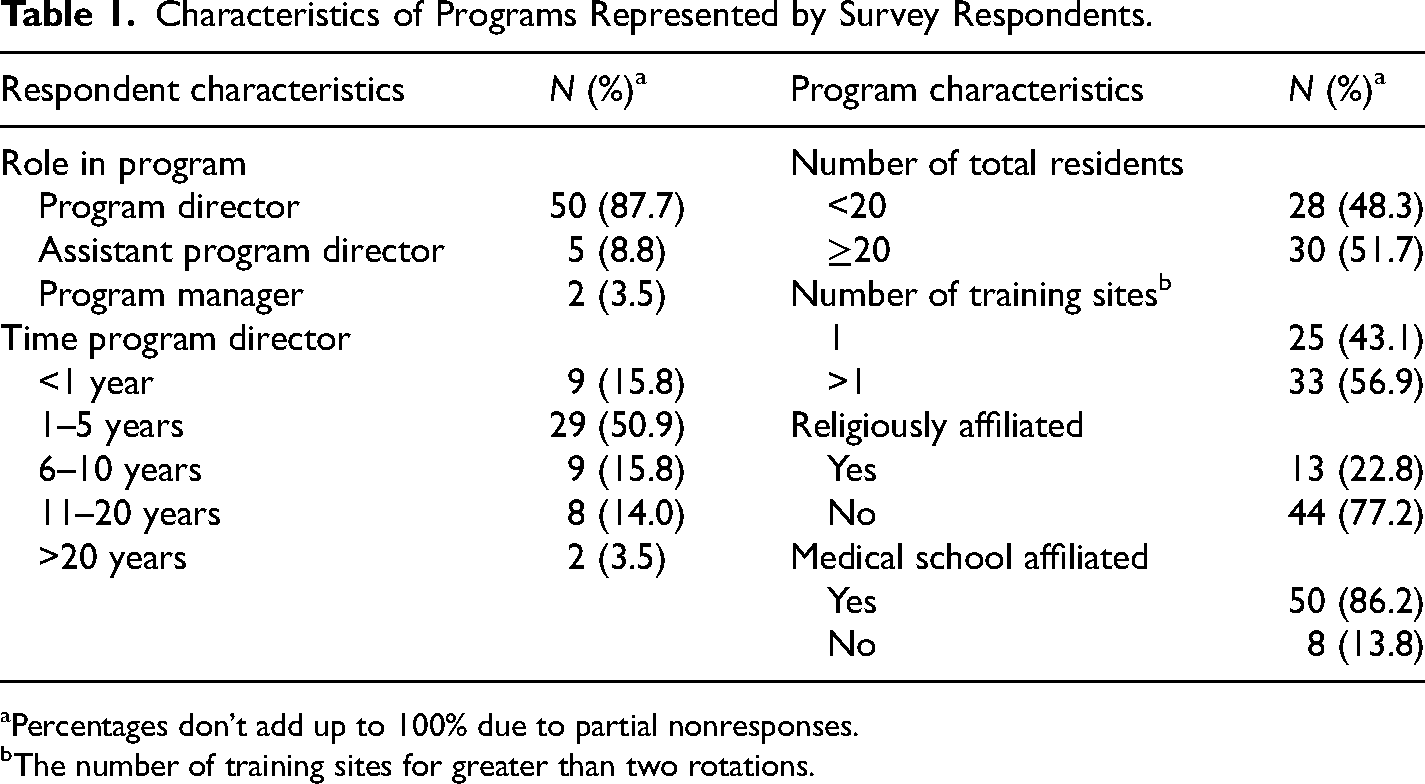
Percentages don’t add up to 100% due to partial nonresponses. bThe number of training sites for greater than two rotations.
In resident continuity clinics, 85.9% of programs reported routine patient screening for a history of sexual assault, 87.0% screened for a history of interpersonal violence (IPV), and 56.2% screened for a history of trauma and/or PTSD. Respondents reported that cases of acute sexual assault were most commonly evaluated by sexual assault nurse examiners (SANE; 63.6% of programs) or Emergency Department residents and faculty (22.0%), while only 6.8% reported Ob/Gyn residents and faculty participating in initial sexual assault evaluations.
Yearly training in caring for patients with trauma histories was reported by 19.6% of programs, while 53.3% reported less than annual training, and 27.1% reported no training. Figure 1a summarizes the characteristics of existing training programs by frequency and modality type, with lectures being the most common modality by far. Existing TIC programs are attended by Ob/Gyn residents, faculty, fellows, and medical students most commonly, and only rarely attended by other clinicians (Figure 1b).
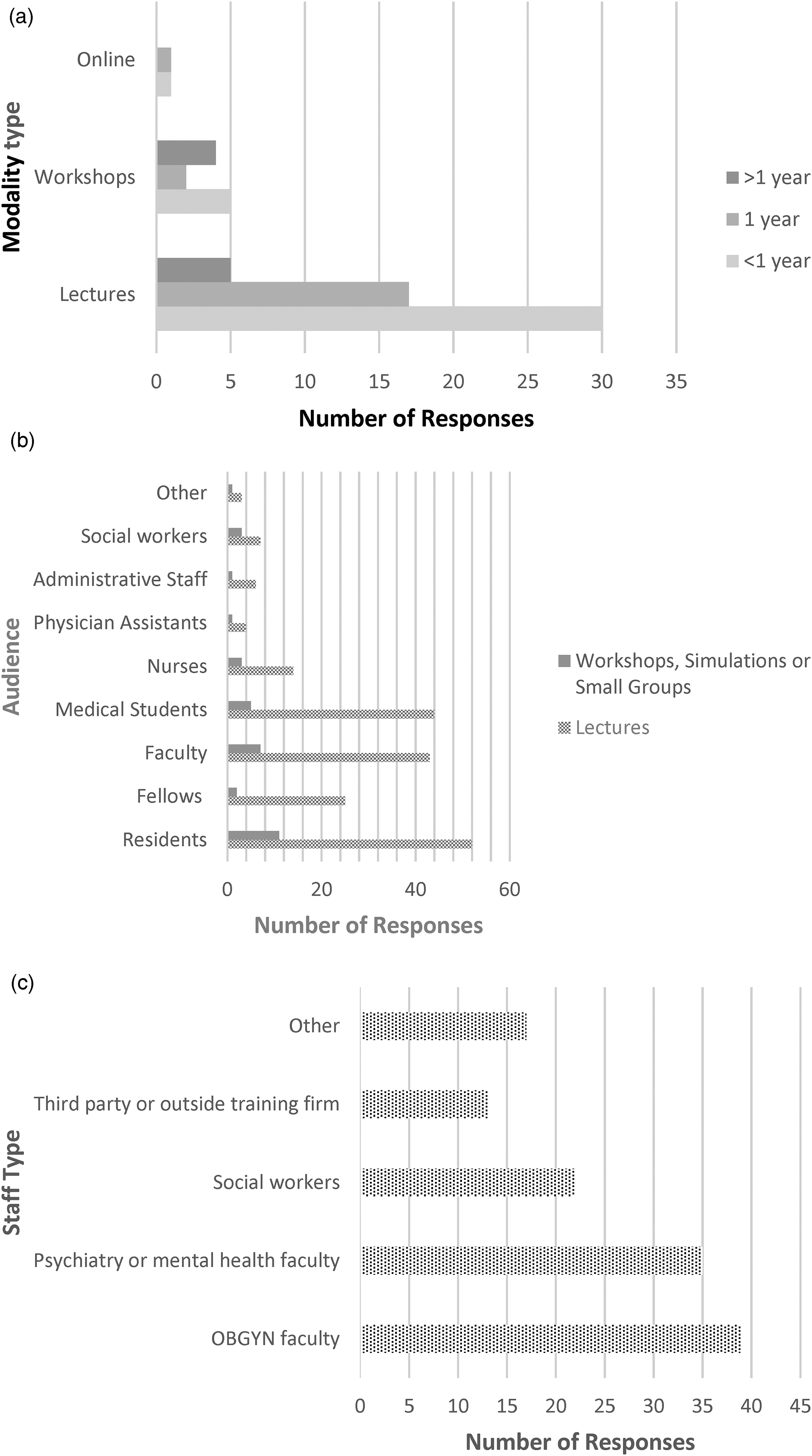
(a) Frequency of program by modality type. (b) Who attends the programs by modality. (c) Facilitators of TIC education.
TIC training was most often facilitated by Ob/Gyn, psychiatry or mental health faculty (58.7%; Figure 1c). Approximately half (52%) of these faculty members were considered experts on the topic of sexual assault or IPV. The remaining 48% were not experts but interested in the topic. Social workers, third-party organizers, and other professionals comprised the remaining 41.3% of facilitators as depicted in Figure 1c. “Other” facilitators included SANE or Planned Parenthood faculty, or those working in other nonprofits with expertise in sexual trauma. Among the programs providing formal education on caring for patients with histories of sexual assault or IPV, 74.2% elicited positive feedback, 3.0% elicited neutral feedback, and 0.0% elicited negative feedback from residents. The remaining 22.7% either had no evaluation done or the response was unknown to the survey respondent.
Of the programs that reported any formal training in sexual assault or IPV, only 25.3% were satisfied with their current programming. In our sample, 93.1% of respondents agreed that Ob/Gyn residents should be trained in TIC. Of the 3.5% of respondents who did not agree with the statement that Ob/Gyn residents should be trained in TIC, one respondent suggested it should be taught in medical school, and another respondent believed such training should be institution-wide, “since all staff members would benefit.” If a TIC curriculum were created specifically for Ob/Gyn residents, 80 programs (92%) would be “extremely likely” or “somewhat likely” to implement it and only one program would be extremely unlikely to implement it. When asked whether TIC should be added to the list of CREOG educational objectives for Ob/Gyn residency programs, 57 (65.5%) agreed, 7 (8.1%) disagreed, and the remaining 23 (26.4%) were unsure.
When asked about barriers to providing training in TIC, a lack of qualified facilitators (26.4%), limited didactic time (18.4%), and lack of national resources or guidelines (14.9%) were most commonly cited. Figure 2 depicts desirable aspects of a hypothetical TIC Ob/Gyn resident curriculum.
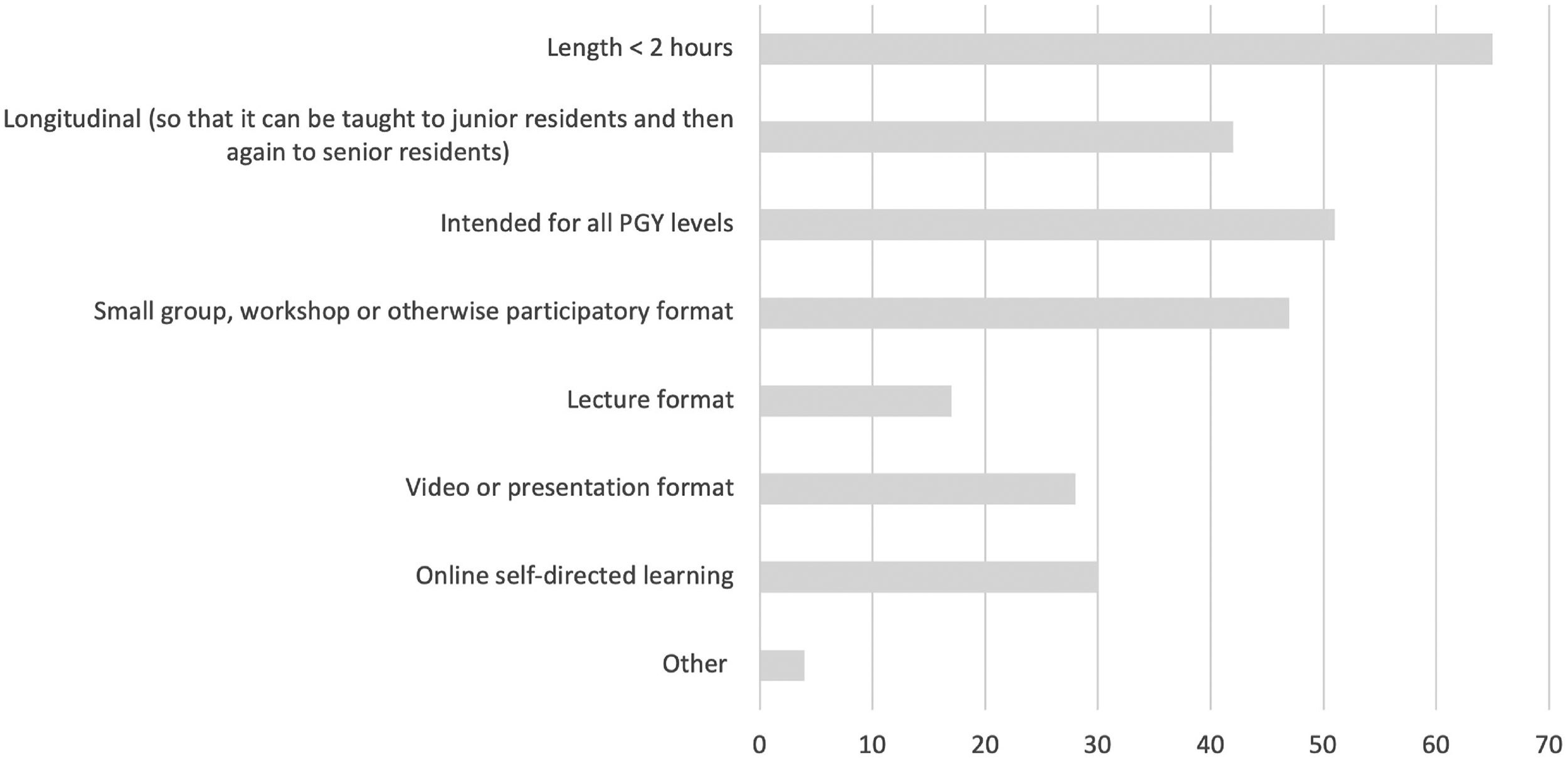
Desired qualities of a TIC education program specifically for Ob/Gyn residents.
Discussion
This study is the first that we are aware of to assess and characterize formal training on TIC provided in Ob/Gyn residency programs. We found that despite a lack of national guidelines on this particular topic, many programs have some formal education on caring for patients with interpersonal trauma histories, but only one in five of these programs has regularly occurring training and the great majority would like to improve this aspect of resident education within their institution.
Given that respondents largely agreed TIC training is important, the lack of regular programming is likely to be a result of the barriers identified in this survey: programs struggle to find facilitators to teach this topic, have little time within their existing curriculum, and are hindered by an absence of national guidelines or resources for providing education in TIC. Dichter et al. (2018) reported similar findings in family medicine programs, where major barriers to implementing TIC training included lack of a faculty champion, followed by lack of time. It is likely other specialties also struggle with finding a recognized expert on this topic, emphasizing the need for collaboration across departments and across institutions. The COVID-19 pandemic has garnered the creation of a national remote didactic curriculum within Ob/Gyn residencies which may provide a venue for such collaboration (Education For All, 2020). National organizations, such as APGO, CREOG, or the Accreditation Council for Graduate Medical Education, may serve a role in facilitating access to TIC experts and training.
Since the adverse childhood events study was published, documenting the high prevalence of childhood traumatic experiences in the general U.S. adult population, many studies have reiterated the pervasiveness of trauma and its tremendous impact on health (Campbell et al., 2016; Lanius et al., 2010). Healthcare providers serve an important role in how patients with a history of trauma interact with our healthcare system. Physicians should have an awareness of trauma-informed practice and apply trauma-informed principles to patient care (Raja et al., 2015). This is especially true for Ob/Gyn practitioners, who regularly broach sensitive topics and perform invasive exams. Fortunately, there are well-established practices that can improve healthcare delivery for trauma survivors as well as reduce the psychologic symptom burden of trauma (Covington, 2008; Elliott et al., 2005; Hopper et al., 2010; Morrissey et al., 2005; Raja et al., 2015). TIC training may also result in increased access to resources for trauma survivors: a year-long study in a managed care setting demonstrated that healthcare providers who were trained to detect IPV made twice as many referrals for IPV resources as providers who were not trained (Kottenstette et al., 2020). Ob/Gyn practitioners who can recognize trauma and respond appropriately are positioned to care for and empower patients in ways that may have far-reaching impacts.
This novel study elicited responses from Ob/Gyn residency programs covering a wide geographic range in North America, program size and diversity in religious and academic affiliation, however, the results may overrepresent PDs who have an interest in this topic or are already providing training on sexual assault and TIC. Nonrespondents may represent programs with even less TIC training, as PDs who are not as familiar with TIC may be less likely to complete the survey. In addition, the response rate indicates limited generalizability or ability to calculate the true prevalence of formal training programs on interpersonal trauma and TIC. In order to calculate the true prevalence of TIC training, programs may need to be surveyed during national meetings or other opportunities when most or all can be reached simultaneously. Another limitation is that this survey queried programs with TIC training on whether facilitators were “experts” in the field or otherwise but did not specify criteria for expertise, therefore the response to this question is very subjective. Furthermore, this study is limited to Ob/Gyn training in the United States and Canada; additional information is needed on how Ob/Gyn providers are trained to care for this patient population in other parts of the world.
Future efforts to create or innovate TIC curriculums should incorporate the responses gleaned from this survey. According to our respondents, such curricula should be interactive, small group-based, intended for all PGY levels, longitudinal and take less than 2 hours to complete for ease of integrating it into existing didactic curricula, all of which are concordant with formats best utilized for adult learning. We propose that such a program should train residents in the principles of TIC, the prevalence of interpersonal trauma and manifestations of trauma from such experiences and also teach residents how to conduct a trauma-informed pelvic exam. In keeping with TIC principles, this programming should also be devised with multidisciplinary input (Huang et al., 2014). It is also important to evaluate the effectiveness of this training, whether residents feel equipped to care for patients with trauma histories and to capture the patient experience to inform curricular development.
Conclusions
This study suggests that though many Ob/Gyn programs are providing some formal training on caring for patients with IPV or trauma histories, few are satisfied with how this training occurs and identify similar barriers to improvement previously demonstrated in other specialties. Moreover, there is strong interest in providing TIC training for Ob/Gyn residents, suggesting that if a resident TIC curriculum were to be developed, uptake would be high. Given how ubiquitous trauma is, and the degree to which the physician–patient relationship is dependent on trauma-informed principles such as safety, trust, transparency, and patient empowerment, significant opportunity exists to improve medical education through the implementation of trauma-informed curricula.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Expanding the Boundaries Grant (Brigham & Women’s Hospital).