
Abstract
Photo-experiencing and Reflective Listening (PEARL) is a trauma-informed intervention developed to promote recovery engagement in survivors of gender-based violence (GBV). This study aimed to understand the feasibility and acceptability of PEARL and identify potential healing elements. GBV survivors were recruited in Philadelphia through an online survey (n = 20). Participants completed the PEARL intervention, a postintervention survey, and a follow-up interview. Results revealed PEARL to be both feasible and acceptable, with thematic analysis revealing its ability to facilitate purposeful reflection, connection to the present, and progress toward healing goals. PEARL shows promise as an engaging strategy to promote healing for survivors of GBV.
Introduction
Gender-based violence (GBV) is violence against an individual based on literal or recognized sex, gender, gender identity, or sexual orientation (Council of Europe, 2021). GBV can take many forms, including physical, emotional, economic, and sexual abuse. A common type of GBV is intimate partner violence, which is violence perpetrated in a romantic relationship against current or past partners.
While any gender can experience GBV, women are disproportionately affected. Globally, one in three women have experienced some form of GBV in their lifetime (WHO, 2021). Relatedly, 43.6% of women in the United States have experienced sexual violence in their lifetime (Smith et al., 2017). Nonbinary and trans individuals also experience a disproportionate GBV burden, with approximately 47% of these populations experiencing some form of physical or sexual violence in their lifetime (James et al., 2016).
Societal norms toward gender and violence have fostered an environment that makes GBV feel tolerated or accepted (Sinko et al., 2021a). People who have experienced GBV often face stigma, disbelief, and safety concerns when seeking support, leading to the underreporting of GBV to law enforcement, healthcare, and social services (Mannell et al., 2018). Societal norms may also influence help-seeking after GBV because survivors may not recognize their experience as violent or worthy of seeking help (Sinko et al., 2021a). Because GBV can have many lasting health impacts on survivors, these unaddressed needs can cause significant challenges to their well-being.
Women survivors of GBV are twice as likely to experience a mental health concern compared to their peers, manifesting as anxiety, depression, posttraumatic stress, mood, and/or substance use disorders (Rees et al., 2011). Survivors also have an increased prevalence of suicidal ideation and attempts compared to their peers, revealing the significant mental, emotional, and spiritual impacts of GBV on survivors (American Psychiatric Association, 2021). Beyond mental health symptom burden, GBV survivors often struggle emotionally to process their trauma. Survivors may feel shame, self-blame, and confusion after a violent incident, with many saying that GBV experiences reshape their sense of self and security (Sinko & Saint Arnault, 2020; Sinko et al., 2022). Regaining power, self-efficacy, and confidence during healing can also be a hurdle for survivors due to the intentional and interpersonal nature of GBV, creating barriers to recovery engagement (Sinko et al., 2021a). For many, healing involves reframing their worldview to regain a sense of purpose and safety (Sinko et al., 2019). Hence, rebuilding one's relationship with oneself, others, and the world is vital (Sinko & Saint Arnault, 2020), which is not often holistically addressed in clinical and social care settings due to fragmentation in survivor support infrastructure.
Trauma Treatment for GBV Survivors
Clinically, GBV-related trauma has been traditionally treated using therapeutic approaches similar to those used for posttraumatic stress disorder (PTSD). The American Psychological Association recommends three interventions to treat PTSD: cognitive behavioral therapy (CBT), cognitive processing therapy (CPT), and prolonged exposure (PE) therapy. CBT focuses on the relationship between thoughts, feelings, and behaviors. This treatment focuses on current stressors and addresses patterns of behaviors, thoughts, and feelings that contribute to adverse health outcomes. CPT is a branch of CBT that focuses solely on challenging and changing disruptive beliefs related to traumatic experiences and stopping troublesome thoughts and behaviors that interfere with individuals’ daily lives. PE, as the name suggests, is a type of CBT where individuals are gradually exposed to traumatic memories, feelings, or situations to alter an individual's thought process to decrease alarm reactions and avoidance (APA, 2021). While many survivors do desire PTSD-oriented mental health treatments, not all survivors of GBV have PTSD. For example, studies estimate that only about one in four women survivors of intimate partner violence experience moderate to severe PTSD symptoms (Coker et al., 2002). In addition, some survivors may be ready to begin exploring their healing but may not be interested in formal mental health therapy or have challenges accessing it. Thus, there is a need for additional, more accessible interventions offered outside of clinical settings to help survivors work toward healing in their daily lives.
Healing After GBV
A recent review synthesized GBV survivor perspectives of healing. Through this review, healing was found to be conceptualized by survivors as a multidimensional, iterative, nonlinear journey requiring courage, patience, and active recovery engagement (Sinko et al., 2022). Survivor-identified healing goals included processing and reexamining trauma, managing negative states, rebuilding the self, connecting with others, and regaining hope and power (Sinko et al., 2022). These diverse goals suggest that while symptom burden is an important consideration, selfhood, social, and future-oriented aspects may be missing when only symptom reduction is emphasized (Sinko et al., 2022). Thus, to improve care and support for individuals who have experienced GBV, it is critical to develop interventions that approach GBV recovery in a multidimensional and holistic manner.
While some survivors understand their healing needs, many encounter barriers when seeking support for their healing. These barriers can include logistical factors (money, time, and insurance), abusive partner interference (preventing survivors from disclosing violence or seeking help), a lack of awareness of available resources and how to access those resources, feeling “frozen,” and lack of social support (Fugate et al., 2005; Saint Arnault & Zonp, 2022; Taylor, 2020). Survivors may also struggle with maintaining self-efficacy and may minimize their trauma, causing a lack of authentic and active engagement in their healing and a decreased likelihood that the survivor will participate in help-seeking behaviors (Johnson & Johnson, 2013; Sinko et al., 2019). Because of these complexities, developing a recovery-oriented action plan with the help of a trained interviewer may help decrease survivors’ cognitive burden and organize their needs to guide future decision-making. With this in mind, the purpose of this study is to pilot test an intervention (Photo-experiencing and Reflective Listening [PEARL]) that leverages photo-elicitation to develop a healing action plan to promote active recovery engagement for woman-identifying survivors of GBV.
The Promise of Photo-elicitation to Explore Healing After GBV
Though traditional clinical approaches effectively address clinical symptoms of trauma, these approaches may not address GBV-specific healing needs and may not be accessible to all survivors (Fugate et al., 2005; Johnson & Johnson, 2013; Taylor, 2020). Many of these approaches can be costly and inaccessible to underserved and underinsured communities. In addition, many traditional methods put the provider in control of the treatment plan and pathologize trauma responses, reinforcing a power dynamic in which survivors may feel a lack of voice or control (Fugate et al., 2005; Sinko & Saint Arnault, 2021). Photo-elicitation approaches may therefore fill a critical gap in the current survivor support infrastructure.
Photo-elicitation is the use of photographs as a stimulus within an interview setting to facilitate a verbal discussion about a particular phenomenon (Burles & Thomas, 2014; Harper, 2002). Photo-elicitation, particularly when it is participant-driven (e.g., Van Auken et al., 2010), has been described as a methodology that enhances empowerment by making meaningful experiences visible while leveling power dynamics in treatment and research spaces (Copes et al., 2018; Lapenta, 2011; Oliffe & Bottorff, 2007). A common photographic approach under this domain is PhotoVoice, which leverages the power of photographic documentation and group dynamics to provide a process by which people can identify, represent, and enhance community (Wang et al., 2000). PhotoVoice has been used in a variety of research contexts, but elements of this method have been perceived to be therapeutic. For example, a recent systematic review of qualitative studies that have used this research technique with survivors of GBV revealed its potential to transgress violence through promoting care for the self and others, illustrating the problem of GBV, and harnessing internal resources (Christensen, 2019). In contrast to this, while many agree that PhotoVoice has been historically successful in promoting awareness of social justice-related issues, a recent systematic review and meta-analysis revealed a minimal impact of PhotoVoice on both physical and mental health outcomes (Halvorsrud et al., 2022). This may be because PhotoVoice was not originally designed to be an intervention or because PhotoVoice may not be appropriate in all situations, particularly for topics more personal in nature where participants may wish to keep their identities hidden from others. Despite this, participants who have experienced trauma or harm frequently share the perceived benefits of engaging in PhotoVoice and other photo-elicitation methodologies. Because of this, additional photographic methods intentionally developed as interventions are needed to extend and test this impact in survivor care settings.
We developed PEARL to promote healing exploration in community settings and the context of survivors’ environments (Sinko & Saint Arnault, 2021). PEARL involves an at-home photography-focusing prompt and a follow-up interview where survivors use their photographs to assess their needs and create an action plan, which may or may not include a connection to formal services. Depending on survivors healing needs, they may want to form goals using the resources they already have access to or may want to be connected to other evidence-based interventions for GBV survivors to support a specific aspect of their healing (e.g., support groups, biodynamic psychotherapy, and trauma-sensitive yoga; Hou et al., 2016; Ong et al., 2019; Saint Arnault & O’Halloran, 2015). PEARL aims to accommodate all these possibilities by offering survivors an opportunity to reflect on where they are in their healing journey, helping them understand and leverage resources within themselves and their environment while aiding in the prioritization of additional resources needed to support their healing.
The Present Study
This study aimed to understand the feasibility and acceptability of PEARL to promote healing and recovery engagement in survivors of GBV. This study also sought to identify the potential healing elements of PEARL. PEARL aims to create a trauma-informed space to promote participant empowerment by making meaningful experiences visible while altering typical treatment power dynamics. PEARL also attempts to be a tool to amplify survivor self-awareness on how their environment and interactions impact their recovery, providing natural ways for survivors to connect what they learn to their real life (Sinko & Saint Arnault, 2021). Understanding whether this approach functions as intended and is feasible and acceptable to engage survivors during their healing process can support or refute the merit of further evaluation in a large-scale clinical trial.
Methods
Pilot Intervention
PEARL is a photo-elicitation method with theoretical underpinnings of mindful self-awareness, experiential sampling, and trauma-informed interviewing (see Sinko & Saint Arnault, 2021). PEARL starts by asking participants to engage with a photography-focusing prompt over a 1–2-week period to document healing and darker moments as they arise in their lives, using photography with their cell phones or cameras. The prompt states: Within the next week, observe your environment and take photographs with your cellphone or camera of moments that feel healing to you (for example, moments you feel connected, whole, or well), as well as darker moments that you experience (for example, moments you feel overwhelmed, ashamed, or fearful) throughout the upcoming week. There is no right or wrong way to do this. The goal is to understand your day-to-day experience navigating recovery as a survivor of GBV.
Procedure
Our procedure consisted of building community partnerships, training research assistants (RAs), and pilot testing the PEARL intervention with GBV survivors with the help of recruitment liaisons at each community site. After the PEARL intervention, survivors were asked to give feedback via a postintervention survey and a follow-up phone interview one month later. Photographs gathered were then shared, with permission, through an online photography exhibit in which participants and community organization members gave feedback before it went live. This paper focuses on the feasibility and acceptability of the PEARL method, but to see the exhibit showcasing the photographs gathered through this process, go to: https://discover.ourwave.org/exhibit/capturing-my-healing. This study was approved by the University of Pennsylvania Institutional Review Board.
Recruitment Site Engagement
Three Philadelphia GBV organizations partnered with the research team for this project. The principal investigator (PI) gave each organization a presentation about the PEARL method to gather their thoughts and feedback. Based on these conversations, the PI made minor procedural changes to increase the potential feasibility and acceptability of the intervention prototype before the study began. Once all organizational entities approved the approach, one recruitment liaison from each site distributed recruitment materials through flyers, email invitations, and referrals to their survivor networks to gather participants to participate in the PEARL intervention.
RA Training
RAs received trauma-informed qualitative interview training over three 2-h sessions to provide foundational knowledge to support their implementation of the PEARL intervention. These RAs were Social Work Master's degree students in their final year of study. The training involved three phases: (1) education on GBV and the manifestations of trauma, (2) trauma-informed interviewing and disclosure response skills, and (3) an overview of PEARL and how to implement it with GBV survivors appropriately.
Education
For the general education portion, GBV was clearly defined to ensure the group had a joint conceptualization of this concept. RAs were also educated on the three Es of trauma (i.e., events, experience, and effect) as outlined by the Substance Abuse and Mental Health Services Association to inform them of the different ways trauma can manifest. The training also emphasized the causes of and common responses to GBV. RAs were then taught general trauma-informed interviewing skills including active listening, matching the terms survivors used to describe their trauma, ways to resist retraumatization, and appropriate ways to open and close the interview space in a trauma-informed way. RAs were also trained in safety and de-escalation procedures. RAs were initially taught how to conduct interviews for PEARL in person. However, due to the COVID-19 pandemic, this training eventually needed to be modified to conduct PEARL virtually. After training completion, RAs took a written test to evaluate their understanding of training content to determine if they were ready for the skills-based training.
Skills-based training
PEARL skills-based training involved an iterative process of familiarizing each RA with the interview guide, procedure, and protocol. The skills-based training involved: (1) watching a PEARL interview conducted by the PI and debriefing about the process, (2) experiencing a PEARL interview as a participant so that they knew what participants would be experiencing, (3) completing at least two practice interviews with volunteers while filling out a postinterview evaluation form and discuss strengths, concerns, and questions, and (4) giving an interview to a volunteer live in front of the PI, who evaluated them using a rubric. Both RAs passed the training and voiced comfort in proceeding to the pilot study.
Pilot Study
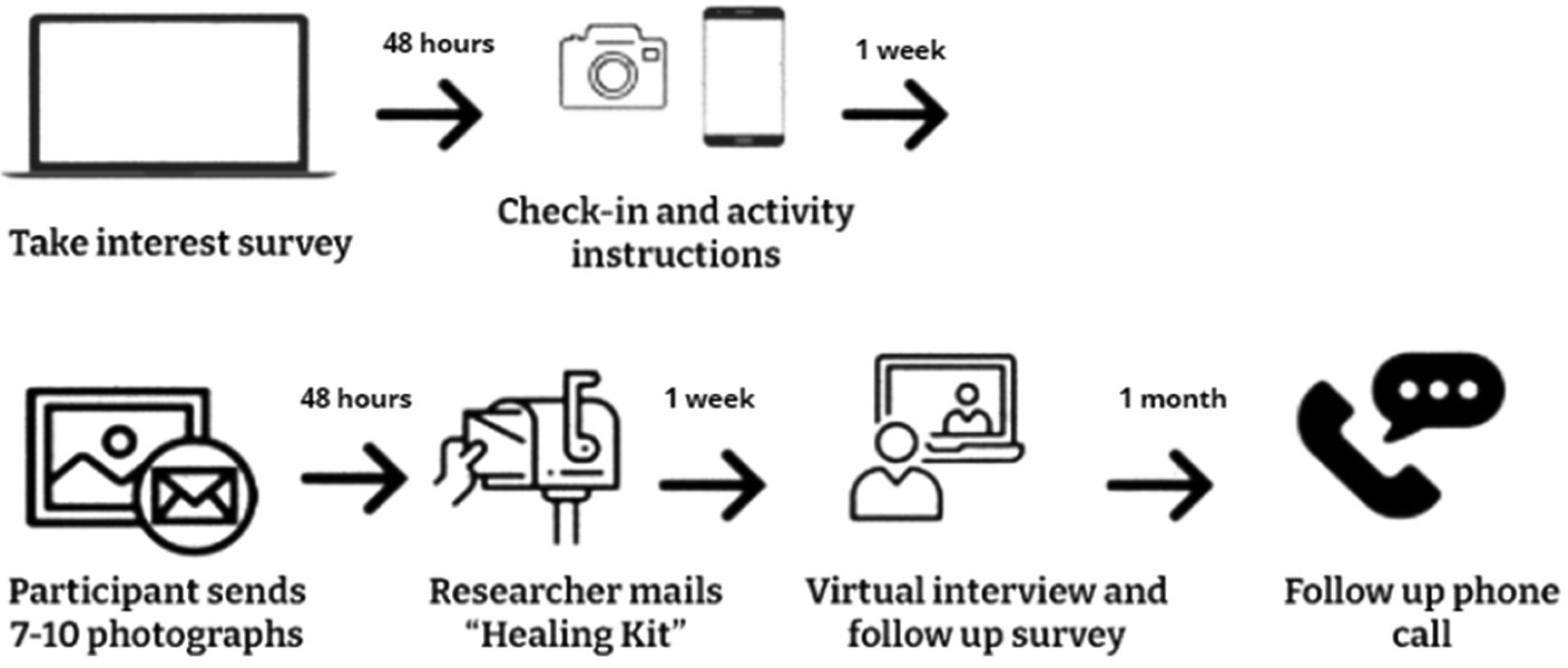
The general study procedure can be seen in Figure 1, but it will be described in more detail below. Participants were directed to a study interest survey, where they completed a background questionnaire containing demographic and trauma history questions along with a baseline healing assessment (The Healing After GBV Scale [GBV-HEAL]; Sinko et al., 2021b). The GBV-HEAL is an instrument aimed at understanding recovery progress after GBV, used in this case to understand the healing potential of PEARL (Sinko et al., 2021c). The instrument consists of 18 statements about one's views of themselves, others, and the world using a 5-point Likert scale (with 0 being “Not at all” and 4 being “To a great extent”). Subscales include relating to others, regaining hope and power, self-connection, and trauma processing/self-advocacy. Good internal consistency, test–retest reliability, construct validity, and convergent/discriminant validity have been demonstrated (Sinko et al., 2021b).
Study procedure.
After completing the online interest survey, study staff contacted participants within 48 h to send them the photography-focusing prompt and schedule their PEARL interview. After the PI received the participant's photographs, photos were printed and mailed to participants in a “healing kit” with an instructional letter, consent forms, stickers, and a fidget toy to use during the interview.
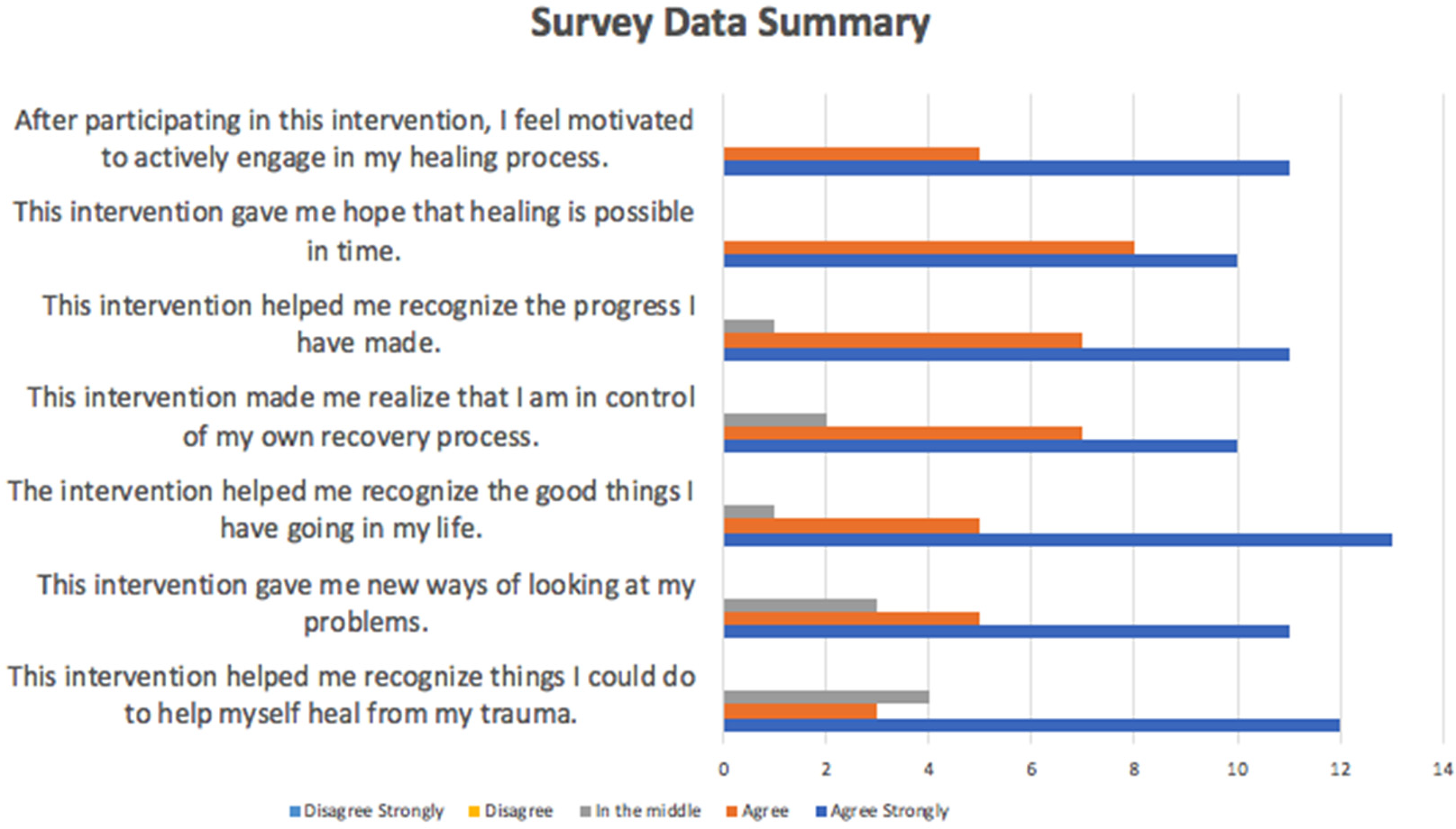
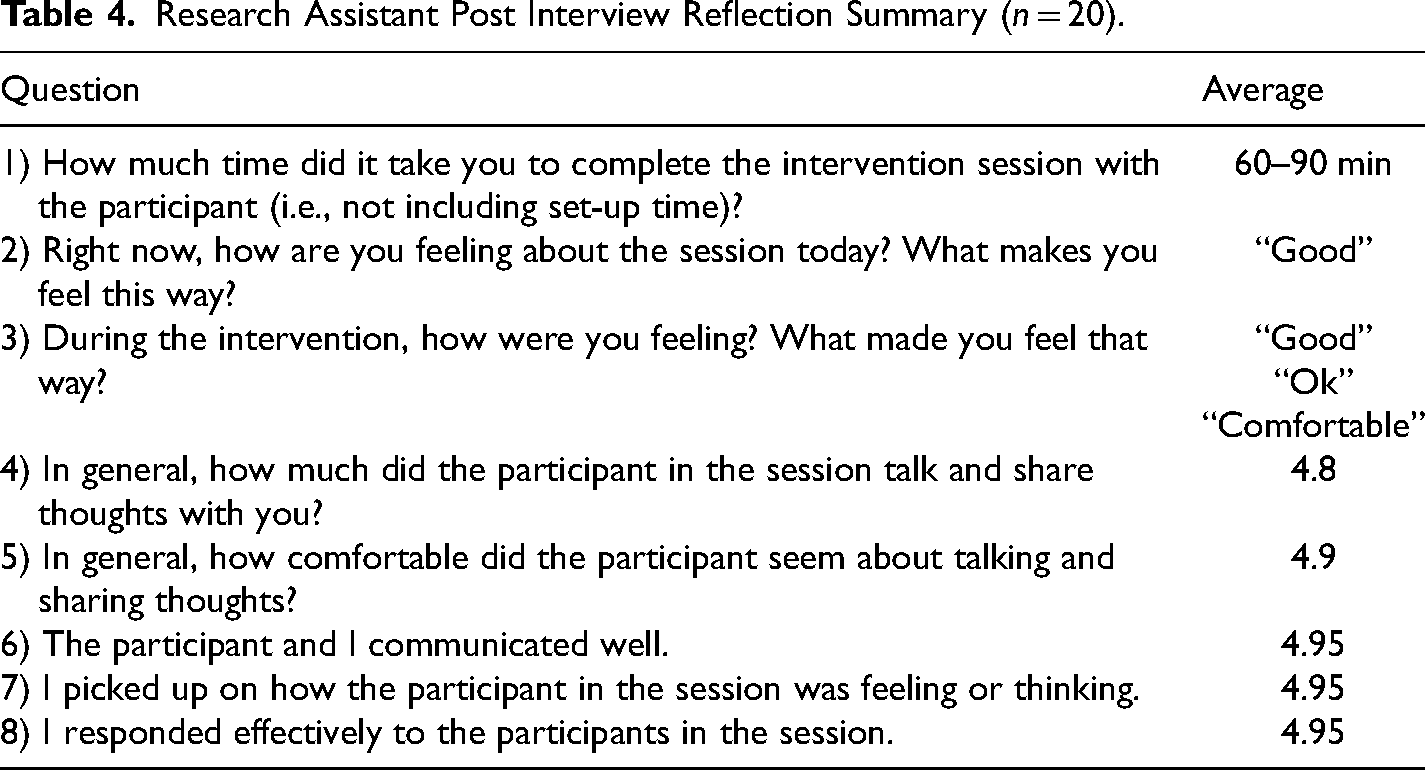
Participants completed all one-on-one PEARL interviews via Zoom. The interviews were audio-recorded. Upon completion of the interview, participants were given a copy of their recovery action plan via email, along with the link to a postintervention evaluation form which had them evaluate the PEARL process and schedule a time for a follow-up interview one month later. Interviewers also conducted a personal postinterview reflection with semistructured free responses and Likert-scale prompts to evaluate their perceptions on how each interview went, how they felt delivering the interview, and how they believed the participant received the interview. This reflection was designed for RAs to reflect on their experiences, process any emotions, and document any visible emotional activation the participant may have experienced that was not caught on the audio recording. See Figure 2 for postinterview check-in evaluation questions and response summaries.
Participant satisfaction.
One month later, participants completed a semistructured, audio-recorded follow-up qualitative phone interview evaluating their experience since engaging with the PEARL method. See Table 1 for a summary of the follow-up interview questions asked.
Key Variables and One Month Follow-up Interview Questions to Operationalize Them.
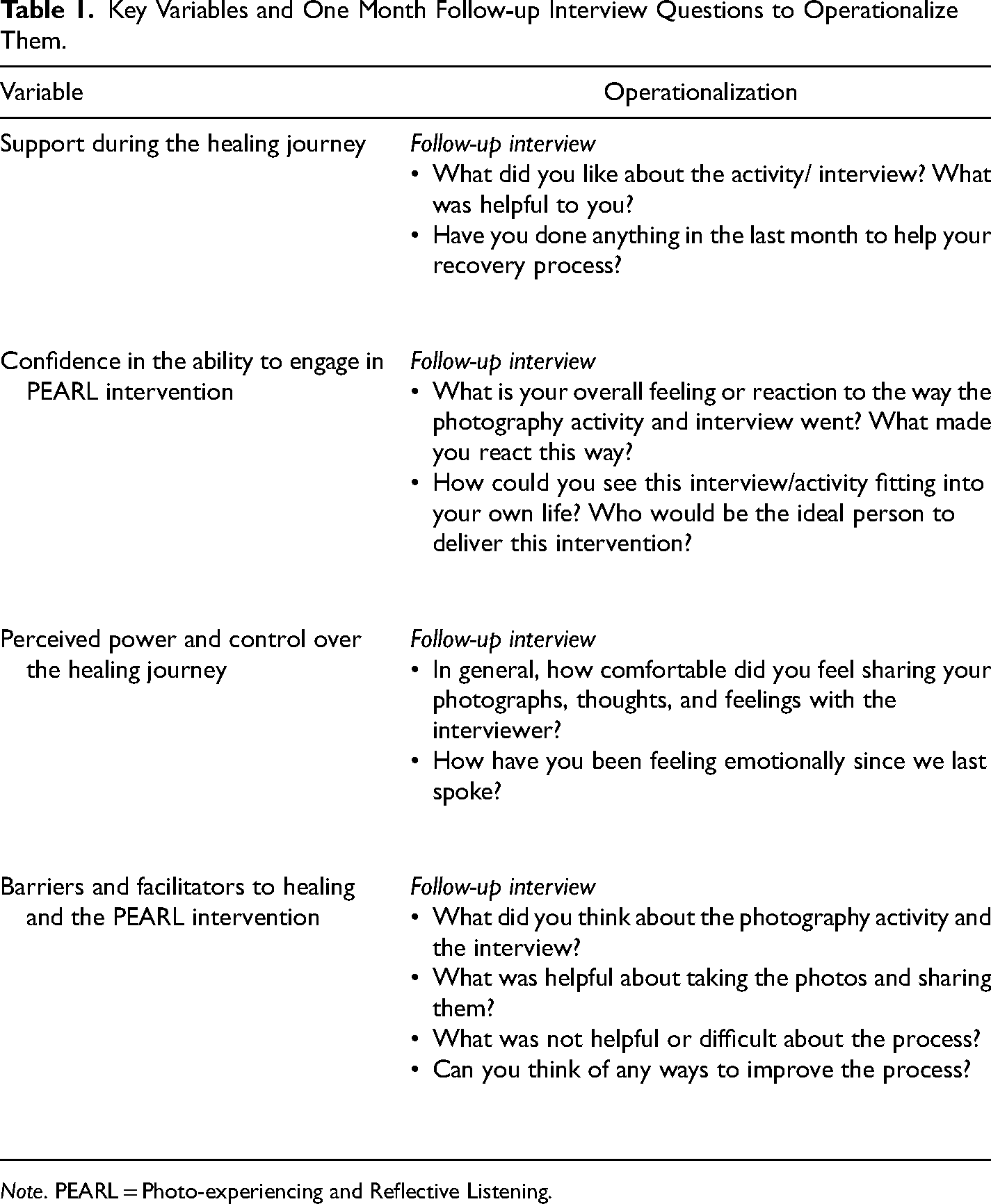
Note. PEARL = Photo-experiencing and Reflective Listening.
Analysis
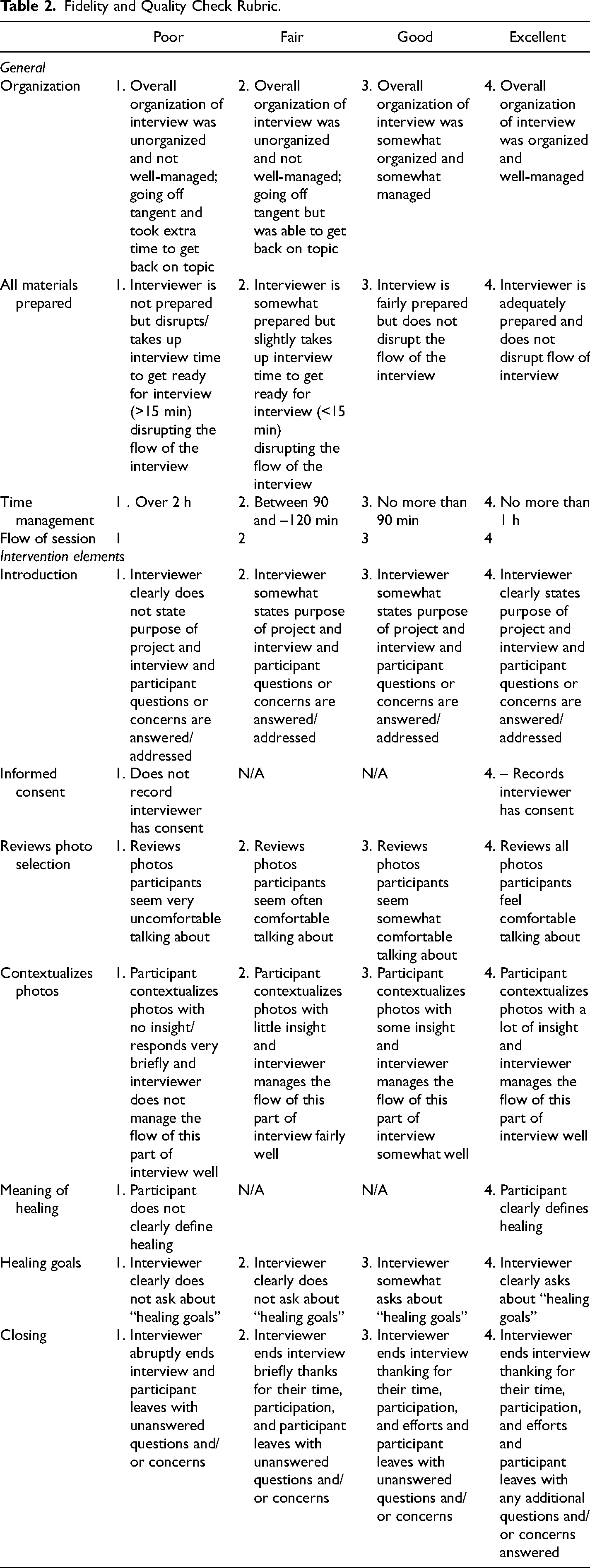
After completing the PEARL interviews, RAs administered intervention fidelity and quality checks. These checks involved an RA who did not conduct the original interview, listening and evaluating each interview using a rubric that asked questions regarding the (1) intervention components and structure and (2) communication and emotional flexibility. Fidelity and quality checks were accessed by listening to each audio-recorded interview twice. The first time was without the rubric to gain familiarity with the interview, and the second time was to conduct a full assessment with the designated rubric. Intervention fidelity and quality evaluation were measured on a 4-point Likert scale (1 = poor, 2 = fair, 3 = good, 4 = excellent) in three categories: general, intervention elements, and communication and emotional flexibility (see Table 2). Averages of item scores were taken to measure overall fidelity and quality.
Fidelity and Quality Check Rubric.
Descriptive statistics and paired sample t tests were conducted to analyze quantitative data using Stata (StataCorp, 2021). This analysis included the quantitative acceptability questions on the postintervention survey and the prehealing and posthealing scores.
Thematic analysis was used to analyze the qualitative portion of this study (Strauss & Corbin, 1998), including the open-ended postintervention survey questions and the audio-recorded one-month follow-up interview transcripts. Close readings of the transcripts contributed to a preliminary sense of the interviews. An initial code list was developed separately by an RA who did not serve as a PEARL interviewer, related to participant comments about PEARL's helpfulness, help-seeking actions attributed to PEARL, and potential challenges that arose related to PEARL participation. Central themes were identified by abstracting codes upwards to main categories, allowing “systematic comparison” and “conceptualizing” (Strauss & Corbin, 1998). ATLAS.ti qualitative software was used for data management and analysis (Muhr, 2006). An audit trail using personal, theoretical, and analytic memos was maintained, with coding concepts being discussed at length in research team meetings to verify accuracy.
Results
Study Sample
Twenty women-identifying survivors of GBV participated in the PEARL pilot study, all recruited through GBV services in Philadelphia, PA (see Table 3). The ages of the women ranged from 22 to 50. Most participants were African American (60%). The highest educational attainment ranged from no high school diploma to a master's degree, with most participants having a bachelor's degree (40%). Fifteen participants reported experiencing more than one type of GBV. Most survivors said that they experienced intimate partner violence, sexual assault, or both. All survivors (n = 20) completed the PEARL intervention and postintervention survey. Fifteen completed the one-month follow-up interview.
Participant Characteristics.
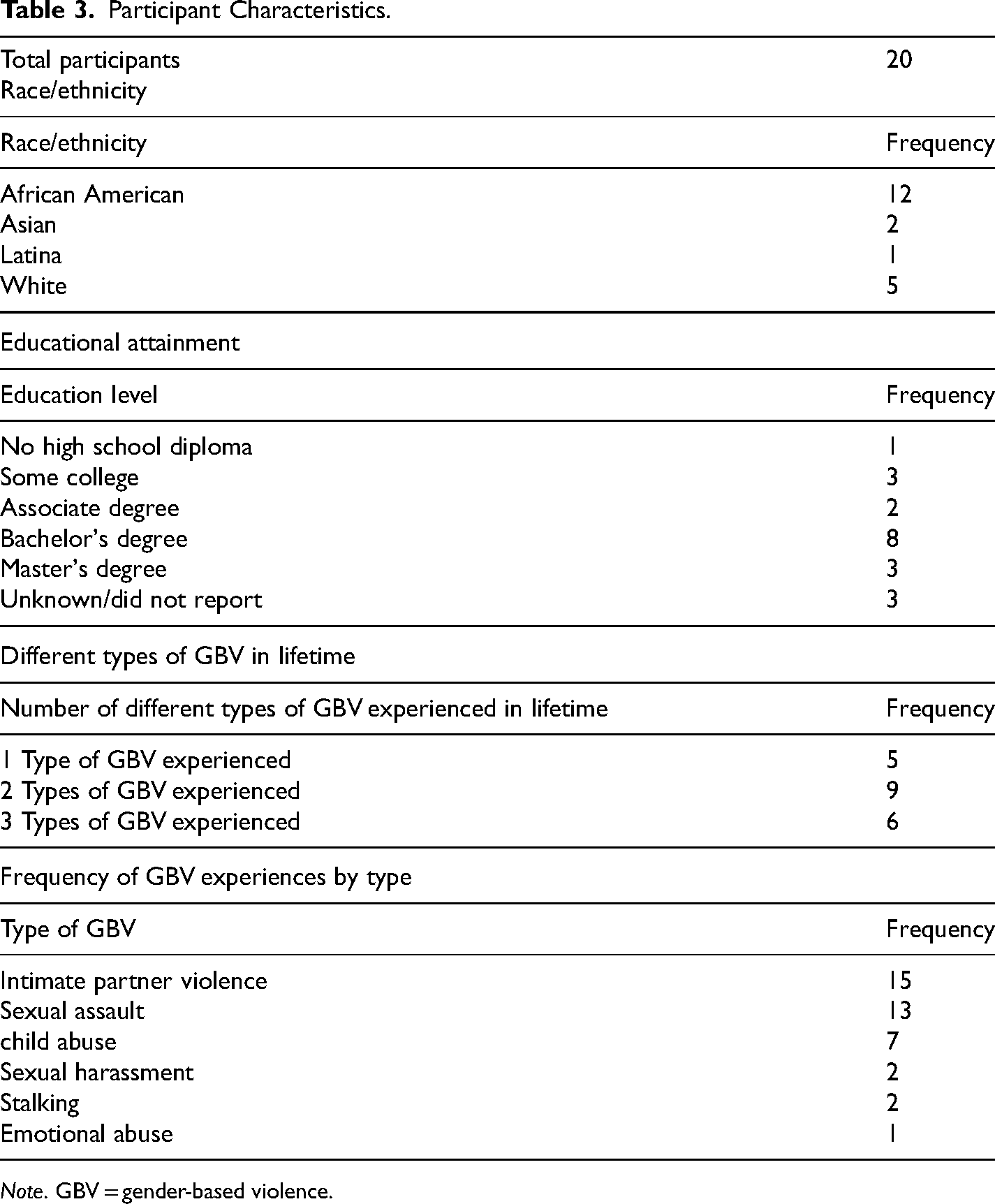
Note. GBV = gender-based violence.
Aim 1: Feasibility of the Intervention
GBV service providers and organizational directors provided vital initial input to increase the feasibility of this intervention before its implementation. This feedback included but was not limited to (1) having the sessions be 1–1.5 h, (2) providing both in-person and virtual meeting options, (3) having a study camera if participants did not have a cellphone with a camera on it, and (4) and ensuring photography prompt language was no higher than an eighth-grade reading level.
RA training
RAs were trained in intervention delivery in three 2-h sessions. RAs passed the written test the first time (95% and 100%) before moving to the skills-based assessment. Both RAs completed their practice interview within 1.5 h.
Intervention fidelity and quality
Likert scale averages revealed that intervention fidelity and quality were good overall (m = 3.74). Likert scale averages also showed excellent communication and emotional flexibility (m = 3.9). The lowest average was found under “Time Management” (m = 2.85), as two interviews went beyond the hour-and-a-half-suggested period (but did not exceed 2 h).
Aim 2: Acceptability of the Intervention
Overall, satisfaction was high in the postintervention survey and the one-month follow-up interview. When asked how much they liked the experience on a scale from 0 “disliked very much” to 5 “liked very much,” 16 people indicated they “liked it very much,” and three indicated that they “liked” it. One person shared that they “neither liked nor disliked it.” Comments shared by participants included: (1) “I really liked the connection of the series of photos to my healing journey; it was therapeutic to discuss it in this way and also helped me get clear on my goals,” (2) “It allowed me to reflect on some things of my past. I was able to look at all the things that helped me to be able to continue my journey,” and (3) “It was helpful to put pictures besides bruises to my pain.”
When asked if the intervention made them feel overwhelmed by the emotions it brought up, 15 people said “no,” four people said “a little,” and one person said “yes.” However, the person who said yes upon follow-up indicated that the overwhelming feeling did not last beyond the interview period. When asked what they disliked about PEARL, 17 people said “nothing.” Others had some comments, including: “I felt some anxiety about being recorded initially, but that went away quickly. Other than that, it was great!” and “I felt like it didn’t capture everything and was a little harder during quarantine when a lot of my days felt similar. I wish it captured other moments like texts I sent between friends.”
RA observations and reflections
Postinterview reflections revealed that RAs felt “good,” “okay,” and overall “comfortable” executing the interview. RAs noted that “rapport building” supported the environment for the participant to “share a great deal” and increase willingness to participate during the photo selection process, meaning of healing, and healing goals. Additionally, RAs repeatedly reported participants being “open,” “engaged,” and “enjoying” or “gaining” a positive experience from PEARL. Overall, the RAs’ critical self-reflections (as interviewers) and observed observations (for participants) reveal a mutually productive interaction. The RA's average Likert score ranged from 4.6 to 5 on their postinterview evaluation forms, with the three highest-rated areas being: (1) The participant and I communicated well, (2) I responded effectively to the participant in the session, and (3) I responded effectively to the participant in the session. See Table 4 for more details.
Research Assistant Post Interview Reflection Summary (n = 20).
Aim 3: Understanding the Potential Healing Properties of PEARL
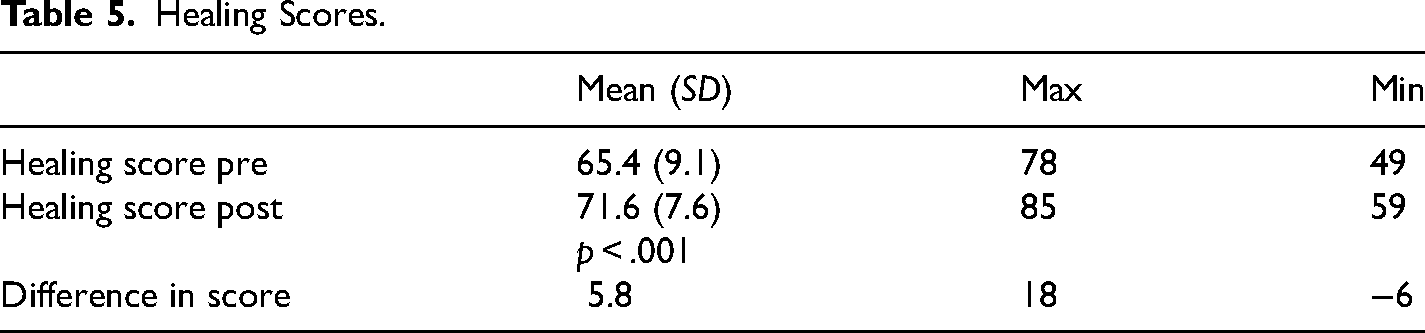
Qualitative analysis of the postintervention surveys and one-month follow-up interviews of PEARL participants aimed to describe the potential healing elements of PEARL. Results revealed three general themes of how PEARL may facilitate healing: purposeful reflection, connection to the present, and promoting progress toward healing goals. This section describes each theme and subtheme (Figure 3). We also share how many survivors contributed to our understanding of each theme by providing frequencies of responses corresponding to each theme and subtheme. GBV healing scores significantly improved postintervention (p < .001; see Table 5).
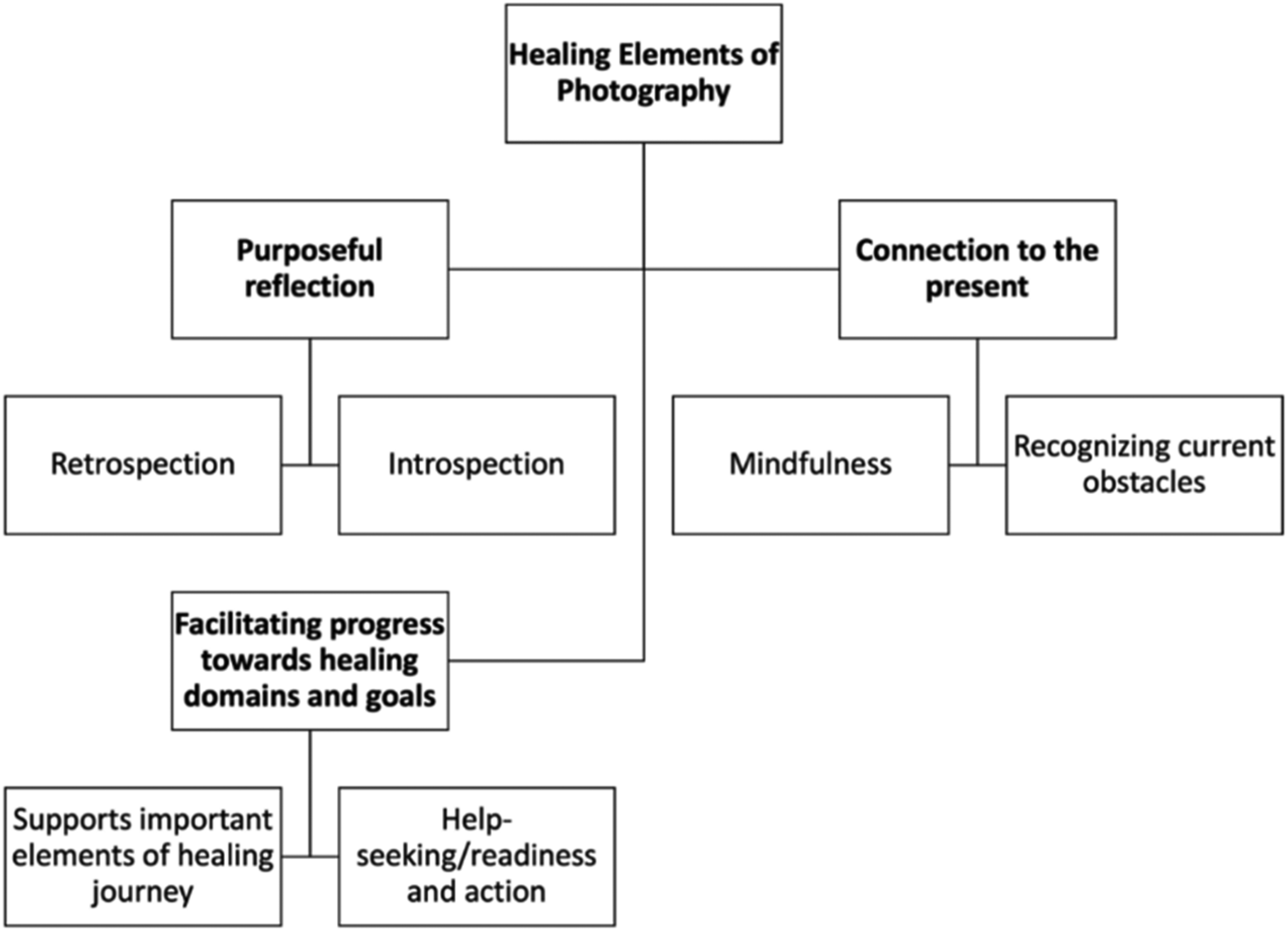
Potential healing elements of Photo-experiencing and Reflective Listening (PEARL).
Healing Scores.
Purposeful Reflection
Survivors found that PEARL aided in purposeful reflection of their healing journey. We defined purposeful reflection as a survivor's intentional participation in thinking and reflecting on their history of trauma and how it impacts their daily life. To illustrate this, 13 survivors (∼86.67%) mentioned PEARL as a catalyst to explore their healing or examine the self “intentionally.” One survivor described PEARL as “help[ing] people to step back and actually like take the time to pay attention” (Participant NY1731). Another survivor stated that PEARL helped them “reflect,” have “gratitude,” and develop “deeper meanings” about their journey (Participant HO1207).
PEARL seemed to facilitate two types of purposeful reflection: retrospective and introspective. For example, Participant PH0966 described the PEARL process as helpful in her healing journey because “[photography] helps [her] appreciate [her] path so far … like as a retrospective and an introspective process.”
We defined retrospection as participants looking back on healing that has been done thus far and developing an appreciation for their progress. Eleven survivors (77.3%) reported that PEARL aided in retrospection. Participants used phrases such as “looking back” and “seeing what [they have] been through” to describe the retrospective process. For example, Participant GR0708 remarked, “The images will always drive [the] conversation … [and are] a reflection of where that person is.” Another survivor said: It was helpful to kind of see my journey laid out … when you’re in the middle of survival, it's very easy to kind of be focused on the things that are directly in front … be[ing] able to just kind of step back and be present and see the big picture was really helpful (Participant KC1313).
Introspection describes the ability of PEARL to help survivors look inward to understand themselves, their emotions, and their healing needs for the future. Eight survivors (∼53.33%) characterized PEARL as an introspective approach to trauma processing. One survivor commented, “I was very surprised about the kind of like stimulation that I got emotionally … from sharing why I took these pictures and what they meant to me” (Participant WE2603). Another survivor mentioned that when they viewed the pictures taken for the intervention, they reflected on “who [they were], where [they are] going, and what things [they are] not going to put up with” (Participant CA2303). In this way, by looking inward, survivors recognized the personal impact of their GBV experience and what they may want to work on going forward to live the life they knew they deserved.
Connection to the Present
Connection to the present described PEARL's ability to allow survivors to be present with their surroundings, thoughts, and the impact of their trauma histories on their current life experiences. Nine survivors (60%) referred to photography's ability to allow them to be present. For example, one survivor noted, “[the photographs] made me think a lot more about what I value and allowed me to be more present” (Participant ME0751). Several survivors (n = 5) described the connection to the present as “mindfulness” and the ability to recognize current obstacles to their healing journey.
Mindfulness describes the capability of survivors to be fully present and aware of their surroundings, actions, and thoughts. Five survivors (33.3%) identified PEARL as a facilitator of mindfulness. For example, one survivor explained that photographs taken during PEARL influenced them to be “more mindful” and “reflect more on [their] experiences” (Participant ME0751). Another participant, Participant PH1405, attributed mindfulness to “self-care,” stating: I think PEARL is helpful in a way of making people think about … self-care … [also] learning how to process different things that are going on because a lot of times … I’m moving so fast … It's hard to be present (Participant PH1405).
Facilitating Progress Toward Healing Goals
Nearly all participants (87%) discussed PEARL's ability to support help-seeking and healing. A survivor noted, “[taking photographs] helped me deal with a lot of stress … [and] things that I need to remember to keep me moving forward. So, it was very inspiring and uplifting for me” (Participant PH2701). Survivors further explained that PEARL supported essential elements of their healing journey and encouraged readiness for seeking help for their trauma and trying to engage with their healing in a more intentional and formal way.
Survivors described the photographs taken through PEARL as reminders of self-worth and that they encouraged them to create and maintain healthy boundaries. Nine survivors (60%) mentioned that PEARL encouraged movement toward their healing goals, such as regaining power and hope, recognizing strength, rebuilding the self, processing trauma, and connecting with others. One person shared: I’ve been doing a lot of thinking … where does this stuff come from? Why is … it okay to [let] people be disrespectful? A lot of processing. Those pictures really put it … you know, they’re there when the stuff is happening, but when you have to talk about those pictures, especially that one about the amplified sound [photo], I felt like nobody ever listened to me, and that began into beginning to think about well how long has that been going on and what situations is this relevant? And I’ve been starting to pay attention … I’ve become aware, consciously aware of it (Participant PA2817).
Discussion
The present study sought to understand the feasibility, acceptability, and healing potential of a photo-elicitation intervention, PEARL, in woman-identifying survivors of GBV. Overall, this intervention was found to be both feasible and acceptable. We identified that PEARL allowed survivors to process their healing and identify their needs in the future. PEARL also seemed to mitigate power imbalances between the provider and patient. Mitigating power imbalances may promote more survivor choice, control, and engagement, making it a trauma-informed way to create a personalized plan tailored to meet their unique needs based on where they currently reside in their healing.
Feasibility and Acceptability of the Intervention
It was feasible for social work master students to learn how to deliver this intervention within three brief sessions. A baseline understanding of therapeutic listening, trauma-informed practices, and de-escalation strategies, however, was foundational for this short training. Because of this, nurses, psychologists, and other providers may also be appropriate to deliver this intervention in the future. In addition, community social workers and psychologists whom we partnered with to develop this intervention agreed that PEARL would be feasible in one to two sessions, with the photography-focusing prompt being “homework” for their clients. Because of this, future research should test the efficacy of this intervention on a larger scale with a randomized control group, harnessing the skillset of GBV providers already working with survivors in social and health service settings.
The Power of Narrative
Through the interview, PEARL harnesses the power of narrative, which is not new for trauma treatment
Photo-elicitation approaches have been used in the past to provide a foundation for shared knowledge-building (Padgett et al., 2013; Wang et al., 2000). Previous studies have documented the deeper understanding visual data can bring compared to narrative alone (True et al., 2015). It is important to note that perhaps beyond the use of images, the process of positive interactions and reflections facilitated by the PEARL structure may also enhance its therapeutic properties. Furthermore, experience sampling is especially important for assessing moods, thoughts, symptoms, or behaviors that can change over time (Ebner-Priemer et al., 2009). PEARL combines all of these principles and ideas to create a survivor-centered package to facilitate purposeful reflection, connection to the present, and the articulation of healing goals.
Photography Revealing Healing on a Continuum
Photography allows survivors to apply healing techniques outside of a clinical setting and assess how they impact their mood, thoughts, and behavior (Sinko & Saint Arnault, 2021). Photography can also give survivors tangible items to aid in describing a complex construct such as trauma healing (Glover-Graf Noreen & Miller, 2006). The survivor-driven aspect of photography gives survivors control over their stories and their journeys as they share them with professionals, underscoring the healing dynamic of regaining control (Prag & Vogel, 2013). Survivors can also be met where they are at and make goals at their own pace, which may enhance treatment readiness (Johnson & Johnson, 2013). Survivors in this study identified PEARL's ability to capture healing throughout time, even though survivors captured the photos in the present. The photographs served as a reminder of the past while acknowledging current circumstances and future goals. Survivors used the photographs as reminders of their progress and strength. Past photography interventions have not studied this relationship in GBV recovery contexts.
Photo-elicitation has often been used as a data collection method, but few studies have tested its use as an intervention. Some similar studies have evaluated the impact of photography as a therapeutic tool more generally. For example, Glover-Graf Noreen and Miller (2006) analyzed the use of photography as a therapeutic tool to treat adults with chemical dependence and its impact on trauma-related symptoms. They found that the photos served as a vessel for self-expression and for participants to have a tangible product to discuss their path to recovery. All but one participant in this study showed a boost in self-esteem during post-evaluations. In addition, Prag & Vogel (2013) also examined the use of therapeutic photography to link visual awareness to self-awareness and indicators of posttraumatic growth in adolescent Shan migrants. The authors discovered five significant themes: increased gratitude in their lives, more intimate relationships, increased perception of personal strength, acceptance of new opportunities, and spiritual development. Due to the similar structure, PEARL may also have similar benefits.
Photography Can Help Restore Power Balances
Regaining power is essential to reestablishing and maintaining survivors’ self-worth and confidence while healing from GBV (Sinko et al., 2022). Survivors in this study mentioned that having control as a photographer aided in advancing their healing goals, further supporting the dynamic relationship between perceived power and healing. The present study's findings support the relationship between treatment engagement and power imbalance mitigation. Past research identified that power imbalance in treatment could lead to trauma entrapment in survivors, in which they feel pressured to “get better.” Pressure to no longer feel depressed gives providers power over the pace of treatment and may lead to unmet treatment goals for survivors (Taylor, 2020). Overall, survivors in the present study believed that PEARL gave them control over their stories and allowed them to depict what about their healing was most important to them at the time. As the photographer, survivors could capture their healing through their eyes. Without added pressure to “get better,” survivors could process at their own pace, limiting the risks of retraumatization.
Mannell et al. (2018) found that photography may allow participants to incorporate personal values into treatment, increasing cultural competency and engagement. Photographs in the present study represented the unique healing journey of each survivor, effectively making the survivor an expert in their experiences with the authority to direct their treatment direction. Through PEARL, survivors could capture the subject matter they were comfortable discussing and lead the discussion of the photographs. One survivor in the study disclosed that the discussion of the photographs became overwhelming at one point for her. Even in this case, she felt comfortable redirecting the conversation while recognizing and acknowledging her emotions. Ultimately, this choice and control may be protective for survivors who want to engage in their healing, but fear getting triggered by a provider's approach.
The Need to Promote Healing Beyond Symptom Reduction
Trauma healing is not linear, and there is no one-size-fits-all approach to addressing recovery after GBV. Because of the significant impact of GBV on mental health, even interventions beyond traditional trauma treatments typically focus on alleviating the mental health symptom burden alone. For example, several survivor-centered intervention studies have used improved depression, anxiety, or PTSD scores to determine recovery progress (Hansen et al., 2014; Hou et al., 2016; Ong et al., 2019). While these studies were able to uncover the importance of support groups, biodynamic psychotherapy, and trauma-sensitive yoga in improving symptom burden for survivors of GBV, focusing on recovery as simply the absence of symptoms “may not capture all relevant aspects of survivors’ reactions” and as such “may prevent an exploration of the full scope of what constitutes recovery” (Ranjbar & Speer, 2013).
Strengths and Limitations
A significant limitation of this study is the sample size (n = 20), all of whom were seeking services from domestic abuse and rape crisis organizations in Philadelphia. Since the recruitment of participants occurred in organizations where survivors actively disclosed their GBV experience, the sample for this study may not fully represent the unique circumstances of GBV survivors who often do not share their experiences. In addition, our sample consisted of primarily urban-dwelling, heterosexual cisgender women. Future research should be conducted to understand if this intervention resonates with survivors of other genders, sexual orientations, and geographic locations. Future research should also test this intervention with a randomized control group, to compare the results of PEARL to standard survivor healing approaches.
The sample population is also limited in the representation of GBV experiences. All participants of the study experienced intimate partner violence. Also, the study participants did not have recent experiences with GBV, with most experiences experiencing GBV over one year before the intervention. The effectiveness of PEARL may be different for those more proximal to their GBV experiences. Future research should explore this in more detail.
Due to COVID-19, PEARL intervention was conducted virtually via Zoom. The ability to participate in this study relied heavily on the participant's access to a stable internet connection and a private area to conduct the Zoom interview. Participants also had to possess a certain level of electronic literacy to complete the intervention. These restrictions may have been a barrier to survivors who would typically be able to participate in the intervention in person.
Despite limitations, the study provides insight into PEARL's potential to promote healing for survivors of GBV. The vast age range, racial differences, and educational levels of participants suggest that PEARL may be an accessible tool for survivors of many different backgrounds. Future research should explore this with a larger sample size and a more intentional intersectional lens to document differences in PEARL's impact based on survivor demographic characteristics and the hurdles they face unique to them and the interlocking systems of oppression they face.
Summary of New Knowledge
PEARL gives survivors of GBV authority over their healing journey by maintaining a survivor-driven and trauma-informed approach to understanding personal healing goals. PEARL was found to be a feasible and acceptable intervention for survivors of GBV. It seemed to aid in their abilities to process their healing journey on a continuum while minimizing power imbalances. Through PEARL, survivors can reflect on the past, connect to the present, and set goals for their future. Future research should include survivors of varying GBV experiences, sexual orientations, and gender identities to promote the generalizability of these findings to all women and gender-expansive survivors. PEARL has the potential to promote healing, but more testing is needed on a larger scale to understand its potential to complement current treatments for GBV survivors.
Conclusion
While there are various treatment options for GBV survivors, many can feel stuck at some point throughout their journey. They may need support identifying what they need to continue moving forward and what is getting in the way of them living the life they know they deserve. PEARL may be a low-cost, viable intervention to promote recovery engagement for GBV survivors by providing a tool for service providers to cocreate a personalized healing roadmap for the survivors they work with. Based on the results of this pilot study, future research will further evaluate the efficacy of this intervention using a larger survivor sample and a randomized design. By thinking creatively and bringing survivors’ healing environments into clinical and social service spaces, we can better meet survivors where they are, provide tailored resources and referrals, and help them develop unique strategies to heal, grow, and thrive after these experiences.
Footnotes
Acknowledgments
We would like to thank Women in Transition, Lutheran Settlement House, and the Philadelphia Center Against Sexual Violence (WOAR) for their partnership on this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was generously funded by the Ortner Center on Violence and Abuse at the University of Pennsylvania. Laura Sinko’s research time was funded by the National Clinician Scholars Program.