
Abstract
Intimate partner violence (IPV) is a major global health concern and is particularly high among adolescents in sub-Saharan Africa. We collected weekly surveys for one year from 421 South African adolescent boys and conducted interviews with 48 participants. Quantitative analyses revealed that daily fluctuations in negative emotions were associated with higher odds of IPV perpetration, but binge drinking was not. Qualitative analyses highlighted anger, perceived infidelity, and emotional (dys)regulation as drivers of perpetration. South African adolescent boys exhibit unique risk factors for IPV compared to adult samples. Interventions for adolescents should incorporate emotional regulation and conflict management strategies.
Intimate partner violence (IPV) remains a major global health concern and is associated with severe consequences, including physical injury and pain, mental illness, and sexually transmitted infections such as human immunodeficiency virus (HIV) (WHO, 2021). IPV is particularly common in South Africa; recent estimates of past-year IPV perpetration among adult men range from 18% to 48% (Bhushan et al., 2023; Hatcher et al., 2019). Researchers have identified several contributors to the high levels of perpetration in South Africa, including the prevalence of common risk factors such as socioeconomic disadvantages (Hatcher et al., 2022; Zharima et al., 2024), cultural attitudes and gender norms (Mthembu et al., 2014), and exposure to adversity and abuse in childhood (Treves-Kagan et al., 2021). IPV perpetration is also shaped by contextual factors unique to South Africa, including men's experiences with apartheid-related violence (Gupta et al., 2012).
Research on IPV correlates, prevention, and intervention typically focuses on adult relationships (Johnson et al., 2023, 2024). However, IPV victimization is actually highest among adolescent girls (Stöckl et al., 2014). Thus, it is critically important to identify the unique risk factors for IPV perpetration among their partners: adolescent boys and young men. Adolescents are engaging in romantic relationships for the first time, while also experiencing emotional volatility and learning to regulate difficult feelings like anger and frustration (Schweizer et al., 2020). Similarly, they experience a stronger desire for risk taking than either children or older adults and navigate curiosity around risky behaviors like alcohol use (Spear, 2011).
The intensity of these experiences may be heightened for South African youth. South African adolescents experience high levels of early adversity, including witnessing violence in their communities, and alcohol misuse among adults is common (Boua et al., 2021; Magidson et al., 2017; Otwombe et al., 2015). Both anger and alcohol misuses are shaped by early adversity and parental alcoholism, as well as by high levels of stress (Mahon et al., 2010; Moustafa et al., 2021). The HIV epidemic may further exacerbate these risk factors. South Africa is home to the largest population of adolescents living with HIV (Johannesburg, 2020; UNICEF, 2023). In addition to the physical toll of the virus, the HIV epidemic has exacerbated adversity among adolescents, many of whom have experienced orphanhood, poverty, and social stigma (Boyes & Cluver, 2013; Cluver et al., 2013). As these social conditions intensify negative emotions and alcohol misuse, they may also increase the risk of IPV perpetration.
There are significant associations between negative emotions, like anger and stress, and IPV perpetration in North American samples (Birkley & Eckhardt, 2015). This may be because when emotional regulation is low, as is common during adolescence, it is difficult to interrupt the pathway between angry feelings and aggressive behavior (Finkel, 2008). Anger management programs can help adolescents regulate and redirect this aggression, but these interventions typically require resources (e.g., school psychologists) that are expensive and inaccessible (Candelaria et al., 2012). Moderate associations between alcohol misuse and IPV perpetration have also been observed (Foran & O'Leary, 2008). Alcohol intoxication impairs emotional regulation and cognitive processes, like judgment and decision-making, which may lead individuals to misread social cues and overreact in aggressive ways (Klostermann & Fals-Stewart, 2006). Among adolescents in sub-Saharan Africa, mental health symptoms, substance use, and relationship dynamics (e.g., relationship conflict and communication) have been identified as correlates of IPV perpetration in cross-sectional studies (Johnson et al., 2023). However, cross-sectional research fails to capture the dynamic nature of these emotional and behavioral factors. For example, both trait-level anger and situation-level anger have been identified as correlates of IPV perpetration among American adolescents (Giordano et al., 2016). It is important to appropriately model time-varying factors to clearly identify those important to IPV perpetration in the African context.
Ecological momentary assessment (EMA) methodologies collect data at multiple timepoints and in real time, allowing for more accurate estimates than typical cross-sectional research with the opportunity to model associations both within (i.e., situation-level) and between (i.e., trait-level) adolescents over time (Shiffman et al., 2008). EMA methods have been leveraged to identify important situation-level correlates of IPV among adolescents and young adults, including negative or hostile emotions during conflict and high drinking days (Ha et al., 2019; Moore et al., 2011). Critically, because EMA research requires more sophisticated technology and infrastructure (i.e., smartphones, internet connectivity) most of this work has been conducted among samples in high-income countries. It is not sufficient to assume that these findings generalize to adolescents in low- and middle-income countries (LMICs), whose experiences are shaped by higher levels of adversity and unique sociopolitical stressors.
Given the high prevalence of IPV among adolescents in South Africa, and implications for HIV transmission, additional work is needed to identify and understand predictors of perpetration in this population. The present study leverages a convergent parallel mixed-methods design to test three risk factors for IPV perpetration (i.e., anger, stress, and binge drinking) among South African adolescent boys with and without HIV. Using an EMA method, we separate these risk factors into trait-level and situation-level components to identify stable versus time-varying correlates of perpetration. We use qualitative interviews to contextualize results and explore reasons for perpetration from participants’ perspectives.
Methods
Study Setting
This study was conducted in Soweto, South Africa. Soweto was developed as a township in Johannesburg during the apartheid era to segregate Black Africans (Philip, 2014) and was a hub of political resistance against the apartheid government (Ndlovu, 2006). This legacy of colonialism and segregation provides important context for current conditions (Hoosen et al., 2022). Violence is common in Soweto and many boys report witnessing violence in their community (Otwombe et al., 2015). Moreover, rates of IPV perpetration are particularly high among adolescent boys in Johannesburg, compared to similar cities in other countries (Peitzmeier et al., 2016). Approximately 13% of Johannesburg's population is HIV-positive (Johannesburg, 2020). Because IPV victimization is a risk factor for HIV transmission, identifying the correlates of IPV perpetration in this population is critically important for developing interventions that might decrease transmission risk.
Quantitative Survey
Participant Recruitment and Data Collection
Study recruitment and data collection occurred between November 2020 and June 2023, as part of a study on violence and HIV transmission. Recruitment was stratified by participant HIV status. Study staff visited public HIV care clinics to recruit adolescents living with HIV and community places frequented by youth to recruit adolescents without HIV. Those who were interested in the study were screened at the Perinatal HIV Research Unit located at Chris Hani Baragwanath Hospital in Soweto. Participants were eligible for the study if they were male, between 15 and 19 years of age, living in and around Soweto, and in a dating or sexual relationship. For participants living with HIV, an additional criterion was a documented history of HIV infection before the age of 10, indicating likely perinatally-acquired HIV. Participants enrolled in the HIV-negative group completed an HIV test at baseline to confirm their negative status. Adolescents completed informed consent or assent procedures and caregivers provided informed consent for those under 18 years old.
At enrollment, participants completed a baseline survey on a tablet in a private room in the clinic, with staff nearby to answer questions, and received a smartphone to complete weekly surveys. For a more detailed description of the mobile survey methods, see Dietrich et al. (2024). Participants received a reminder to complete the weekly mobile surveys every week for the following year. Throughout the study, participants were able to communicate with the study team through WhatsApp and a 24-hour hotline. Survey responses were monitored for potential psychological risks (e.g., suicidality). In those cases, a counselor contacted the participant to assess their state and provide referrals for additional care. IRB approval for the study was obtained by the University of the Witwatersrand in South Africa and by Stony Brook University in the United States.
Measures
Outcome
IPV perpetration was assessed at each weekly survey with two questions adapted from the WHO Violence against Women Assessment (García-Moreno et al., 2005). To measure physical IPV perpetration, participants were asked “In the past 24 hours, did you slap, shove, hit, kick, or otherwise physically hurt your partner?” To measure sexual IPV perpetration, participants who reported sexual behavior in the past 24 h were asked “Did you use violence or coercion/threats to get them [your partner] to have sex?” Participants who answered yes to either or both questions were categorized as perpetrating IPV that week.
To better understand participants’ motivations for engaging in violence, those who reported any physical IPV perpetration were asked to choose their reason for the incident from a list, adapted from Whitaker (2014). Potential reasons included “I lost my temper,” “I was stressed or frustrated,” and “I was drunk or high.”
Exposure Variables
Participants’ anger and stress levels were assessed at each weekly survey with two items from the Screening Tool for Psychological Distress (Young et al., 2007). These were: “In the past 24 hours, how much have you been bothered by feeling angry?” and “In the past 24 hours, how much have you been bothered by feeling stressed?” Participants who indicated feeling “moderately” or “severely” angry or stressed were categorized as experiencing anger or stress, respectively. Additionally, they were presented with a list of emojis depicting various moods (e.g., happy, angry, sad, stressed) and asked to choose which one represented their mood at the time of the survey.
Binge drinking was assessed at each weekly survey with a single item, adapted from the Alcohol Use Disorders Identification Test (Saunders et al., 1993): “In the past 24 hours, how many alcoholic drinks did you have?” Participants who reported consuming four or more alcoholic drinks in the past 24 hours were categorized as engaging in binge drinking (Donovan, 2009).
Quantitative Survey Analyses
Descriptive statistics were used to characterize the sociodemographic characteristics of the analytic sample and the variables of interest. Due to the nested structure of the weekly survey data, we used generalized linear mixed models (GLMMs) to quantify the associations between the exposure variables and IPV perpetration (Diez-Roux, 2000). Each exposure variable was split into a between-person (i.e., the mean frequency of the variable over the weekly surveys for each participant, unit = 0.10 to model a 10% increase in the level of exposure) and a within-person (i.e., the deviation of that week's score from the participant's mean, unit = 1.0) component. Both components were entered into the GLMM, with weekly reports of past 24-hour perpetration as the outcome. All models include a random intercept at the participant level and control for the survey week (continuous), participant age (continuous), participant race (dichotomous, Black African or other), participant enrollment in school (dichotomous, enrolled or not enrolled), and HIV status (dichotomous, HIV-negative or HIV-positive).
To better understand the temporal ordering of participant emotions and IPV perpetration, we conducted two sets of exploratory analyses. First, we sought to test whether participants’ negative emotions in the past 24 hours aligned with their motivations for perpetrating IPV in the past 24 hours. We reviewed participants’ self-reported reasons for perpetration, totaling the incidents that participants attributed to anger (e.g., “I lost my temper”) or stress (e.g., “I felt stressed or frustrated”), and created new outcomes based on these categories (i.e., perpetrating IPV because of anger and perpetrating IPV because of stress). We then ran a new set of GLMMs using these outcomes, with past 24-hour anger (stress) predicting IPV perpetration attributed to anger (stress). Exploratory models include a random intercept at the participant level and control for survey week (continuous). We examined the results of these models to explore whether participants’ self-reported emotions aligned with their motivations for perpetration.
Second, we sought to test whether participants’ current negative mood (i.e., at the time of the survey) was associated with their motivations for perpetrating IPV in the past 24 hours. Because we hypothesize participants’ negative emotions preceded their perpetration behaviors, we would expect a stronger association between a measure of their mood in the past 24 hours and perpetrating IPV as compared to the association between their current mood and perpetrating IPV. We ran an additional set of GLMMs with current anger (or stress) predicting IPV perpetration attributed to anger (or stress) in the past 24 hours. We then compared the two sets of exploratory models to determine whether current mood or past 24-hour mood had a stronger association with IPV perpetration attributed to negative mood.
Qualitative Interviews
Participant Recruitment and Data Collection
Participants who completed the quantitative surveys were categorized into groups according to their experiences with violence (low, medium, high), HIV status (positive, negative), and age (15–17 years old, 18+ years old). Within each subcategory, participants were randomly contacted to participate in the qualitative interviews. In-depth interviews were conducted by four research assistants (three with graduate-level education, one with grade 12 education) with previous interviewing experience. They received additional training on asking sensitive questions from members of the senior research team and conducted pilot interviews with boys from the Perinatal HIV Research Unit adolescent advisory board prior to the start of the study.
The semistructured interviews included questions about participants’ interactions with their families, friends, and intimate partners, their experiences with violence, and their drug and alcohol use and motivations for use. Interviews lasted approximately one hour (M = 60 min; median = 59 min; range = 21–96 min). During the data collection process, quality checks were performed on the interviews by senior members of the research team. Interviewers met with the research team biweekly to discuss challenging experiences and emerging themes. Interviews were primarily conducted in English, with interviewers using participants’ preferred local languages (e.g., Zulu, Tswana, Sotho) as needed.
Qualitative Interview Analyses
The research team conducted semistructured interviews with 48 participants from the quantitative study. These interviews were analyzed using a thematic analysis. First, a subset of these transcripts was reviewed and recurring themes were noted. Thereafter, two research assistants reviewed all interview transcripts and compiled a coding framework. The full research team refined these codes and created a final codebook with 16 codes and subcodes. Two research assistants uploaded the interview transcripts into NVivo and coded each transcript according to the codebook. Frequent meetings were held between the research team and research assistants to ensure the quality of the coding and discuss coding decisions and emerging themes. After all transcripts were coded, a subset of 20 was randomly chosen for verification by the senior researchers. For the purposes of this paper, the first author reviewed those codes capturing experiences with relationship conflict and substance use to explore responses that provided context for participants’ experiences with IPV perpetration.
Results
Quantitative Survey Results
We collected 12,603 weekly mobile surveys from 466 participants, with participants completing an average of 27 out of the 52 weekly surveys. For these analyses, we limited our analytic sample to surveys in which participants reported seeing their intimate partner in the past 24 hours and answered the questions about IPV perpetration, resulting in 5,037 survey observations (O) from 421 participants. Most participants identified as Black African (92%, N = 389) with a mean age of 16.5 years at baseline. Participants living with HIV made up about half (51%, N = 215) of the sample. For a description of the analytic sample, see Table 1.
Sociodemographic Characteristics of the Analytic Sample (N = 421).
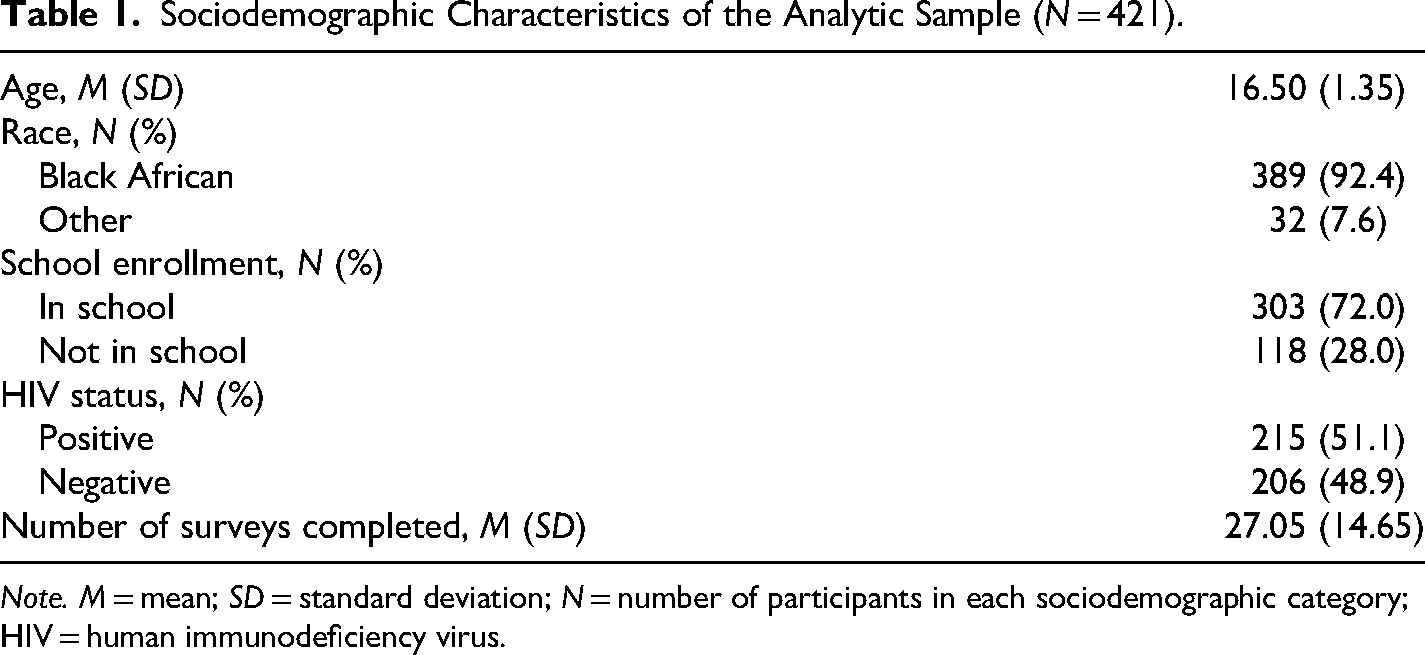
Note. M = mean; SD = standard deviation; N = number of participants in each sociodemographic category; HIV = human immunodeficiency virus.
Many participants reported feeling angry (37%, N = 156), feeling stressed (43%, N = 179), and binge drinking (38%, N = 161) in at least one of their weekly surveys. We averaged across surveys within participants to calculate intraindividual means for anger (M = 0.10), stress (M = 0.13), and binge drinking (M = 0.09). Seventy (17%) participants reported perpetrating IPV in the past 24 hours at least once during the study period (M = 0.05). Participant-level descriptive statistics for the study variables are presented in Table 2.
Person-Level Descriptive Statistics.
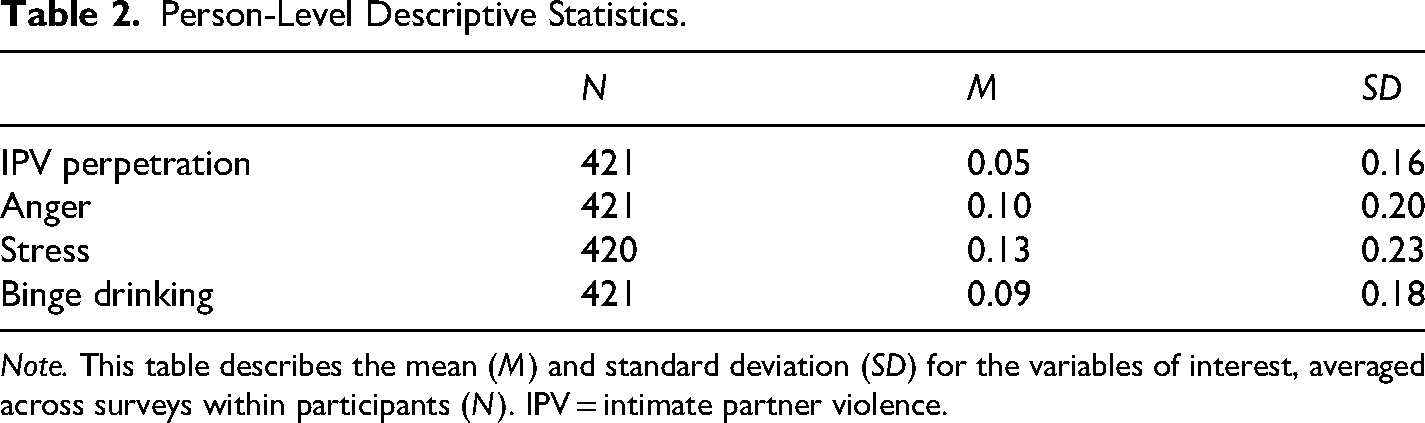
Note. This table describes the mean (M) and standard deviation (SD) for the variables of interest, averaged across surveys within participants (N). IPV = intimate partner violence.
There was a significant positive association between the within-person component of anger and IPV perpetration, such that reporting higher than usual anger in the past 24 hours was associated with a significant increase in the odds of perpetrating IPV against a partner in the past 24 hours (adjusted odds ratio [OR] = 3.22, 95% confidence interval [CI]: 1.71, 6.08). There was no significant association between the between-person component of anger and IPV perpetration, such that individuals with higher average levels of anger did not perpetrate IPV at higher levels than their peers. See Table 3 for model results for all outcomes.
Predictors of Past 24-h IPV Perpetration.
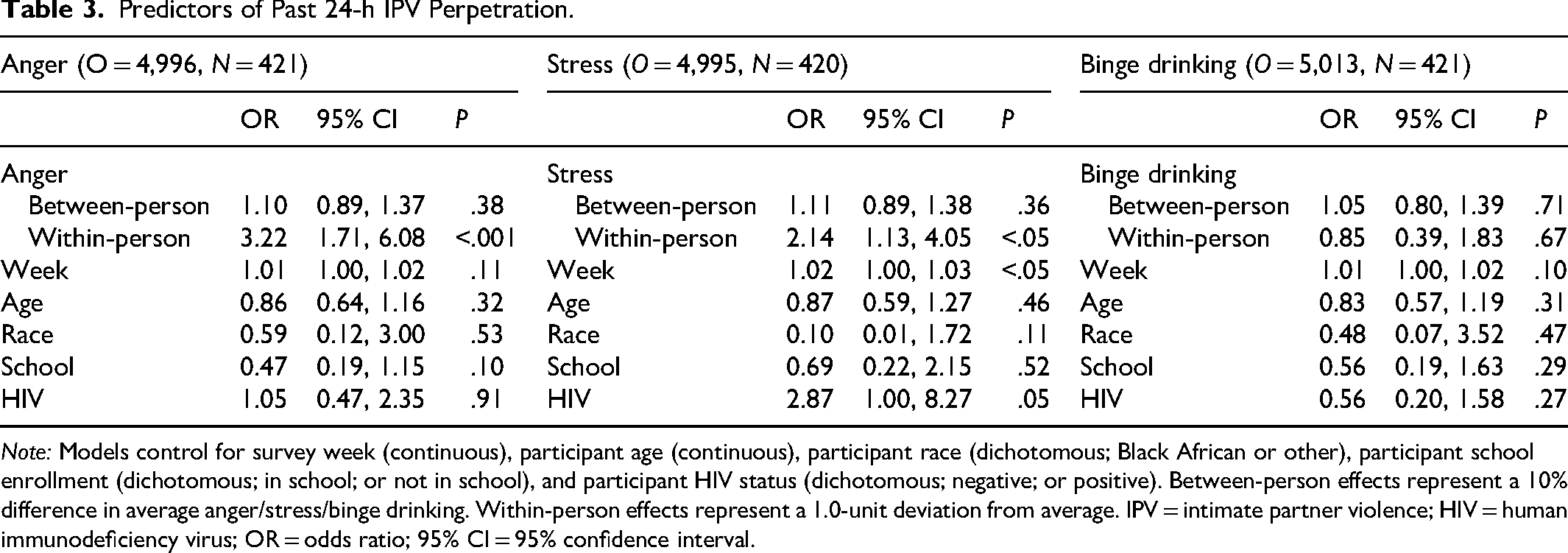
Note: Models control for survey week (continuous), participant age (continuous), participant race (dichotomous; Black African or other), participant school enrollment (dichotomous; in school; or not in school), and participant HIV status (dichotomous; negative; or positive). Between-person effects represent a 10% difference in average anger/stress/binge drinking. Within-person effects represent a 1.0-unit deviation from average. IPV = intimate partner violence; HIV = human immunodeficiency virus; OR = odds ratio; 95% CI = 95% confidence interval.
Similarly, there was a significant positive association between the within-person component of stress and IPV perpetration, such that reporting higher than usual stress in the past 24 hours was associated with significantly higher odds of perpetrating IPV against a partner in the past 24 hours (OR = 2.14, 95% CI: 1.13, 4.05). There was not a significant association between the between-person component of stress and IPV perpetration.
Contrary to our hypotheses, there were no significant associations between binge drinking and IPV perpetration at the within-person or between-person level.
Understanding Timing
To explore whether participants’ negative mood in the past 24 hours aligned with their motivations for perpetration, we reviewed the exploratory models with past 24-hour anger predicting IPV perpetration attributed to anger and past 24-hour stress predicting IPV perpetration attributed to stress. There was a significant positive association between the within-person component of anger and IPV perpetration due to anger, such that reporting higher than usual anger in the past 24 hours was associated with a significant increase in the odds of perpetrating IPV in the past 24 hours and attributing the perpetration to feeling angry (OR = 4.64, 95% CI: 1.65, 13.03). Similarly, there was a significant positive association between the within-person component of stress and IPV perpetration due to stress (OR = 4.49, 95% CI: 1.18, 17.05) (see Table 4).
Past 24-h Mood Predicting Reason for Past 24-h Perpetration.
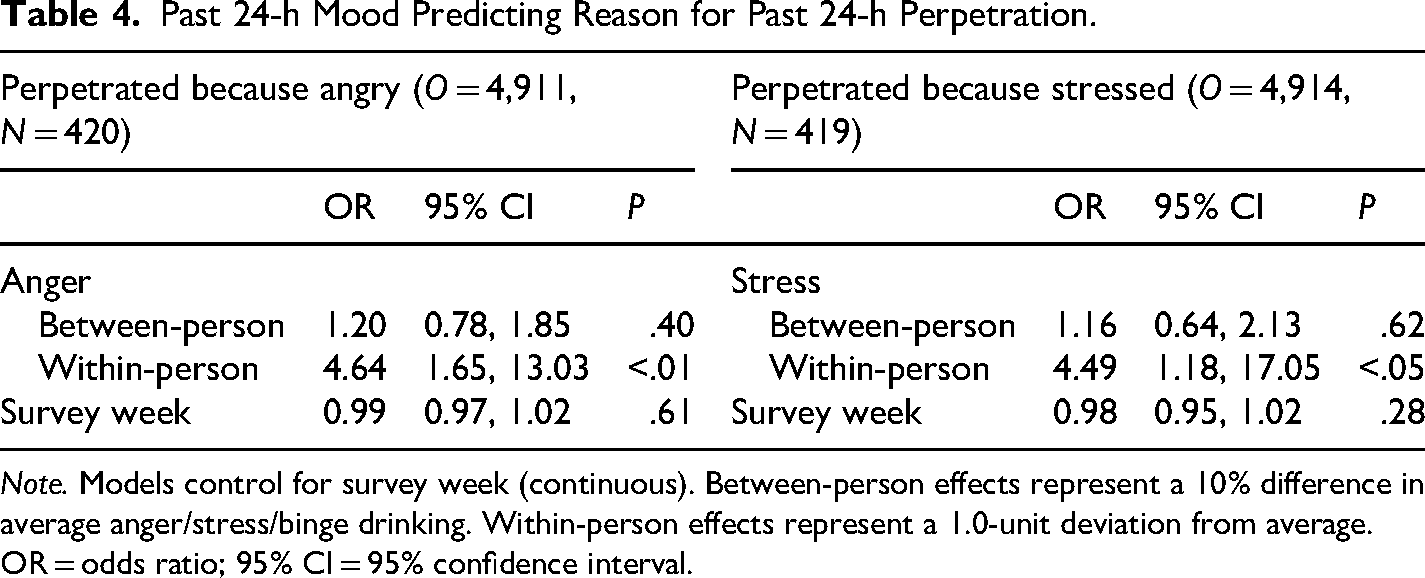
Note. Models control for survey week (continuous). Between-person effects represent a 10% difference in average anger/stress/binge drinking. Within-person effects represent a 1.0-unit deviation from average.
OR = odds ratio; 95% CI = 95% confidence interval.
To further probe the temporal ordering of participant mood and perpetration, we reviewed the exploratory models with current anger predicting IPV perpetration in the past 24 hours attributed to anger and with current stress predicting IPV perpetration in the past 24 hours attributed to stress. We did not find a significant within-person association between current anger and IPV perpetration due to anger in the past 24 hours, nor did we find a significant within-person association between current stress and IPV perpetration due to stress in the past 24 hours (see Table 5). These results suggest that participant anger and stress are preceding violence, rather than violence preceding mood.
Today's Mood Predicting Reason for Past 24-h Perpetration.
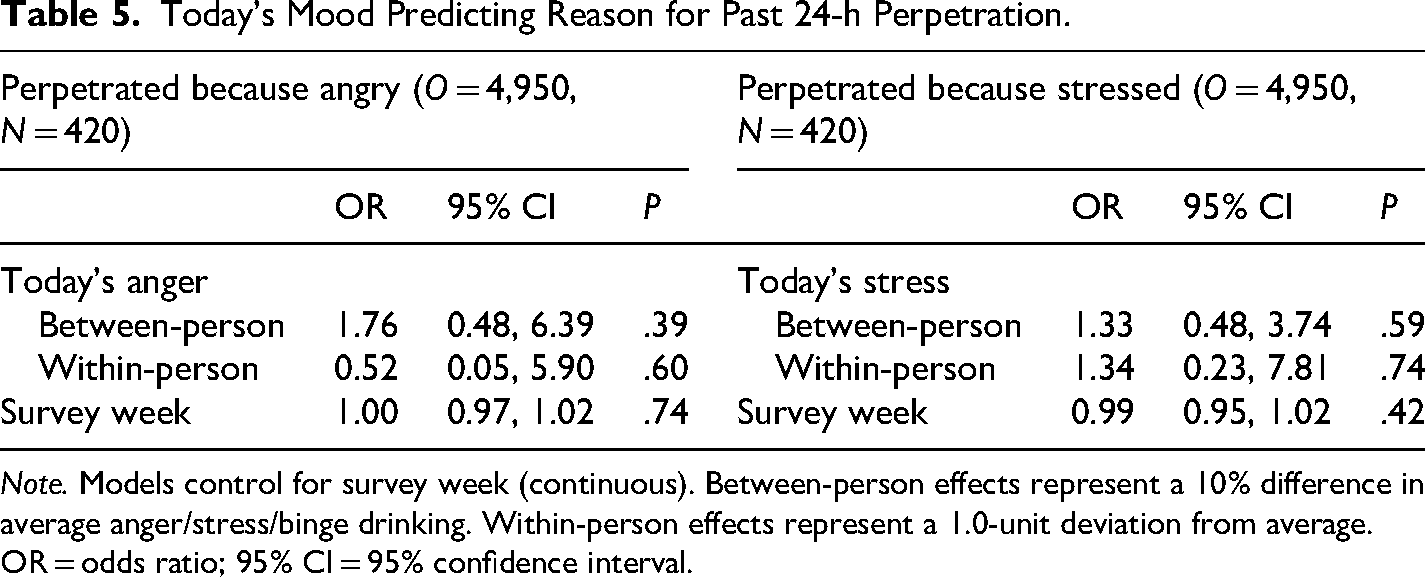
Note. Models control for survey week (continuous). Between-person effects represent a 10% difference in average anger/stress/binge drinking. Within-person effects represent a 1.0-unit deviation from average.
OR = odds ratio; 95% CI = 95% confidence interval.
Qualitative Interview Results
In-depth interviews were conducted with a subset of 48 participants selected from the full study sample. Interview participants were representative of the full study sample in their age, race, education, and HIV status. See Table 6 for a description of their sociodemographic characteristics. Interviews highlighted several common perceptions among participants about IPV perpetration. See Table 7 for participant quotes, organized by theme.
Baseline Sociodemographic Characteristics of Qualitative Interview Sample (N = 48).
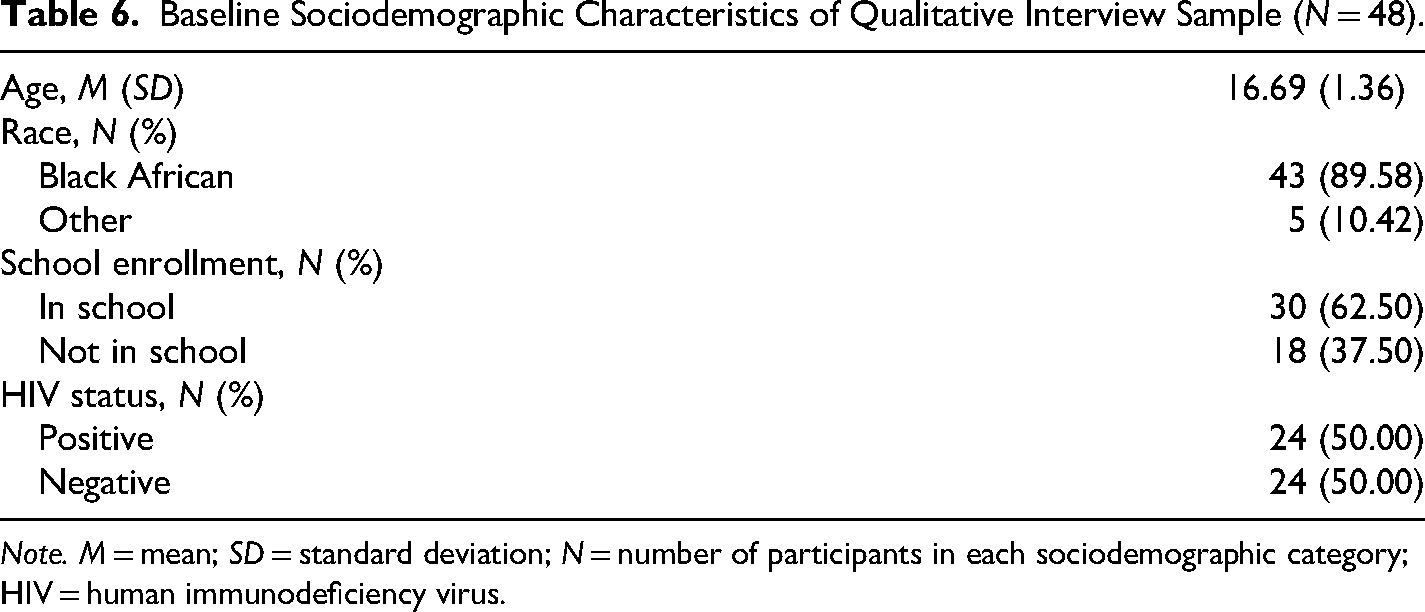
Note. M = mean; SD = standard deviation; N = number of participants in each sociodemographic category; HIV = human immunodeficiency virus.
Participant Quotes From Qualitative Interviews.
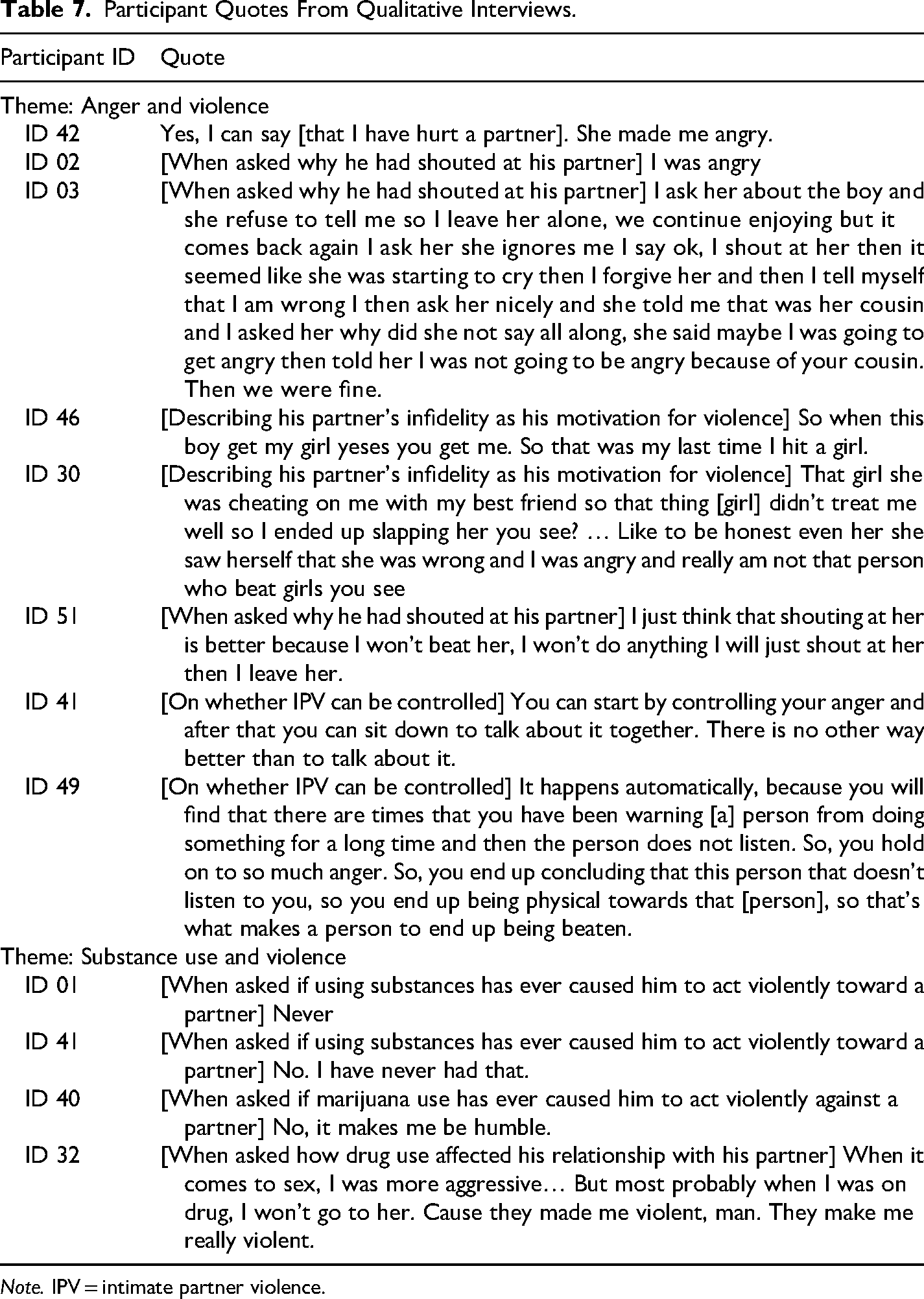
Note. IPV = intimate partner violence.
Anger and Violence
The majority of participants who recalled previous IPV perpetration cited anger as their main motivation for violence. One participant (ID 42) described the last time he yelled at his partner as the result of her making him angry. Another participant (ID 02), who had recalled shouting at a partner, said “I just wanted her to leave. I was angry.” Importantly, most participants focused on feelings of anger toward their partner or caused by a partner's actions, rather than generalized anger from other sources, such as family, school, or financial triggers.
Participants specifically identified cheating or perceived infidelity from a partner as a source of anger and trigger for violence. For example, one participant (ID 03) recalled shouting at his partner after seeing her walking with a boy, after which she revealed that the boy was a cousin. Another (ID 46) became angry when his partner was also dating another boy and responded by hitting her: “So when this boy get my girl yeses you get me. So that was my last time I hit a girl.” A third participant (ID 30) said, “That girl she was cheating on me with my best friend so that thing [girl] didn’t treat me well so I ended up slapping her you see?”
Many respondents highlighted a perceived distinction between IPV perpetration as a character trait versus IPV perpetration as an occasional, justifiable behavior. For example, when asked about his partner's response to his physical violence, one participant (ID 30) said, “Like to be honest even her she saw herself that she was wrong and I was angry and really am not that person who beat girls you see.” Many participants communicated similar ideas. They believed that violence against women was morally wrong and they did not want to identify as “someone who” perpetrates violence. At the same time, many struggled with regulating intense emotions and had difficulty controlling their behaviors. One participant (ID 51) revealed that he occasionally yells at his partner to relieve his anger without physical violence, a strategy he had learned from his friends.
Participants who did not report previous IPV perpetration also acknowledged anger as a source of potential violence. One participant (ID 41) believed IPV could be controlled and prevented in a relationship: “You can start by controlling your anger and after that you can sit down to talk about it together. There is no other way better than to talk about it.” Conversely, another participant (ID 49) believed that IPV cannot be controlled in relationships because anger can be uncontrollable: It happens automatically, because you will find that there are times that you have been warning [a] person from doing something for a long time and then the person does not listen. So, you hold on to so much anger. So, you end up concluding that this person that doesn't listen to you, so you end up being physical towards that [person], so that's what makes a person to end up being beaten.
Stress and Violence
Participants were not explicitly asked about the role of stress in their intimate relationships, though they were asked about the influence of external stressors, like witnessing violence in the community and family, on their behaviors. Although we reviewed participant interviews for connections between stress and IPV perpetration, we did not find any. Participants were aware of stress in other areas of their lives, including their family dynamics and school, but did not cite stress as a motivation for IPV perpetration.
Substance Use and Violence
Most participants who reported using drugs or alcohol said that substance use did not cause them to be more violent or aggressive toward their partners. One participant (ID 01) said alcohol “never” made him violent with his partner. Another (ID 41) was asked if he had ever had an experience where he acted sexually aggressive with a partner under the influence of alcohol, and he responded “No. I have never had that.” A third participant (ID 40) said that smoking marijuana does not make him feel aggressive with his partner, but rather makes him feel “humble.” There was one exception to this trend, with a participant (ID 32) recalling that his previous drug and alcohol use increased his violence toward his partner: “When it comes to sex, I was more aggressive.” However, when his partner confronted him about his behavior, he tried to avoid seeing her while under the influence: “But most probably when I was on drug, I won’t go to her. Cause they made me violent, man. They make me really violent.” Many participants identified substance use as a coping mechanism but did not identify intimate relationships specifically as stressors that prompted substance use.
Discussion
In this study of adolescent boys in South Africa, we found that daily changes in negative emotions, but not in binge drinking, were significantly associated with IPV perpetration. IPV is shaped by factors at multiple levels, including cultural and institutional norms and sociopolitical movements (Bazaanah & Ngcobo, 2024). We also find that individual-level factors, including mood, play an important role. Adolescent girls, particularly in sub-Saharan Africa, experience some of the highest levels of IPV globally (Stöckl et al., 2014). This makes IPV prevention a pressing public health challenge. Additionally, HIV incidence in South Africa is highest among adolescents and young adults, compared to other age groups (UNICEF, 2023). IPV is an established driver of HIV transmission; therefore our results have critical implications for slowing HIV transmission in this population.
First, we found an association between anger and IPV perpetration in our quantitative and qualitative analyses. Previous research has established an association between negative emotions, like anger, and IPV perpetration, though much of this work has been conducted among adults and in Western contexts (Birkley & Eckhardt, 2015). This study confirms this association in a population of adolescents from a middle-income country with high HIV and IPV prevalence. The process by which anger escalates into IPV remains unclear, but Finkel (2007) hypothesizes that relationship conflict leads to aggression through a host of impelling or inhibiting forces, including anger and self-control. Therefore, it is possible that anger reduces adolescent boys’ ability to effectively manage conflict with their partners, leading to IPV. In fact, researchers have identified poor conflict management as a predictor of perpetration in studies of adolescents (Malhi et al., 2020; Russell et al., 2014). Future work should consider clarifying the role of anger in conflict management and aggression, particularly among adolescents.
Importantly, our quantitative analyses revealed a significant within-person effect of anger, but no significant between-person effect; this suggests that IPV perpetration may be the result of a temporary emotional state of anger, rather than anger as a personality trait. This finding is also reflected in the qualitative interviews. Participants who had engaged in IPV believed that IPV was “wrong” and did not identify themselves as perpetrators, but engaged in violence when their emotions exceeded their ability to cope. These findings suggest that participants are not entering their interpersonal interactions angry, but that their anger flares during interactions in response to cues from their partner, again highlighting the potential role of conflict management and communication within the relationship.
Further, cheating emerged in the qualitative interviews as a cause of anger and a precursor to perpetration. There are established associations between (perceptions of) infidelity, jealousy, and IPV (Pichon et al., 2020). Further, in recent qualitative work, Rwandan and South African women identify men's romantic, professional, and economic jealousy as motivation for abusive behavior (Stern et al., 2019). Jealousy may spark relationship conflict, which, if poorly managed, can lead to violence. This might be exacerbated by cultural norms that respect multiple concurrent sexual partners for men, while viewing the same behavior in women as immoral and shameful (Onoya et al., 2015).
When we examined the association between stress and IPV perpetration, we also found a significant within-person effect of stress, but no significant between-person effect of stress. This again highlights the role of situation-level changes in negative mood rather than trait-level changes. Unlike anger, we did not find any mention of stress in the qualitative interviews as it related to IPV perpetration, although participants did talk about stress in other areas of their life, including school and family. It is possible that stress from life experiences outside the relationship is spilling over into the relationship and contributing to IPV but that participants do not see a connection between those experiences. It is also possible that “angry” and “mad” are catch-all words for multiple negative emotions, including stress, and that these feelings are only differentiated when specifically asked about. The participants may have conflated all negative emotions, including stress, with externally focused anger.
The within-person effects of anger and stress on IPV perpetration reveal several potential opportunities for intervention. Although many IPV interventions focus on gendered attitudes, these results highlight the importance of identifying and regulating negative emotions and improving conflict management. Effective interventions for improving emotional regulation among adolescents include elements of mindfulness, cognitive behavioral therapy, emotional awareness and identification, and communication skills (Eadeh et al., 2021). Similarly, there are several conflict resolution programs for students, including those that use role playing, multiplayer virtual games, and online educational interventions (Bosworth et al., 1996; Cheong et al., 2015; Graves et al., 2007). Researchers should aim to adapt existing programs to align with South African contexts and to meet the specific needs of boys. This could include helping boys identify emotions that are typically considered less masculine and engaging boys in role playing scenarios where they discuss infidelity, coping with jealousy and anger, and gender norms around cheating.
More broadly, there is a need for increased research and intervention work on adolescent mental health, particularly in LMICs like South Africa. Globally, about 14% of adolescents report mood disorders like depression and anxiety, but the prevalence of these disorders is higher in LMICs where factors like violence, poverty, and HIV exacerbate mental health challenges (Shorey et al., 2022). In a recent study among adolescents in Soweto, almost one-quarter of participants reported posttraumatic stress disorder symptoms and over one-third reported suicidal ideation (Buckley et al., 2020). Further, there has been little work specifically focused on mental health among adolescent boys. There are gendered differences in mental health conditions, with boys typically reporting more externalizing symptoms (e.g., aggression) than girls (Card et al., 2008). Expanded access to evidence-based mental health interventions targeting boys’ experiences and symptoms would likely have downstream effects on IPV victimization among women, in addition to the salubrious effects on boys’ mental health. However, access to mental health treatment is limited and underfunded in South Africa and other LMICs. Instead, it may be beneficial to pair school-based emotional regulation and conflict resolution interventions with peer-led mental health interventions, like the Friendship Bench or targeted soccer programs (Chibanda, 2017; Peacock-Villada et al., 2007).
Finally, we did not find any associations between binge drinking and IPV perpetration in our quantitative or qualitative analyses. This is in contrast to other work, which does find a link between alcohol misuse and IPV perpetration among South African men (Jewkes et al., 2011; Mthembu et al., 2014). However, those were cross-sectional studies among adult men. There may be something unique about the context in which adolescents are drinking. For example, because many adolescents still live with family members and not with their partners, they may be drinking in single-sex friend groups and do not see their partners after a night out, a common occurrence described by several of the interviewees. A recent systematic review concluded a need for more work on the context in which African youth are drinking, including where they are obtaining alcohol and how they think about drinking (Seekles et al., 2023). Alternatively, our qualitative interviews only recorded perspectives from boys, and it is possible their female partners might have different interpretations of their encounters after drinking. For example, in interviews with South African adolescent girls, participants reported reduced ability to negotiate condom use or refuse sex with a boy who has bought them a drink (Letsela et al., 2019). It is possible for the same sexual encounter to be viewed differently across partners—as consensual for boys but coercive for girls. Educators and clinicians should address the role of alcohol in decision-making and risk-taking, including in relationships, with adolescents.
There were several notable strengths to this study. The EMA structure of the study allowed us to separately capture the variation in risk factors both between- and within-participants over the course of a year, revealing important state versus trait differences. Additional analyses provided insight into the likely timing of participant emotions and perpetration, lending support to the hypothesis that reported anger and stress preceded perpetration. Our exploratory qualitative analyses provided culturally relevant context and revealed additional insights (e.g., the role of perceived or actual cheating in anger and IPV) that we had not identified in our survey questions. Further, by recruiting a large sample of participants already in an intimate relationship, there were more opportunities to collect event-level data on IPV perpetration than in a typical sample.
With these strengths in mind, there are also a few limitations to consider. Because the survey and interview questions relied on self-report, it is possible that participants avoided reporting all perpetration behavior, either due to social desirability bias or because they did not consider their behavior to align with the acts we asked about. Perpetration questions also asked participants about their behavior in the past 24 hours, not in the past week, so we are missing perpetration events that fell outside this window. This means that our estimates of perpetration are highly conservative (they represent acts over an average of 27 days, rather than a full year), but should have no bearing on the associations reported. While stress was identified as antecedent to IPV perpetration in the quantitative data, we were not able to deepen our understanding of how it manifested in participants’ relationships using the qualitative data, as this topic was not probed during the interviews. Finally, the qualitative interviews were not conducted or coded by the first author; however, their analysis was conducted with the input of coauthors who were intimately involved in all stages of the qualitative data collection and analysis.
In this mixed-methods study among South African adolescent boys in intimate relationships, we found that daily fluctuations in anger and stress were associated with same-day increases in IPV perpetration. Interviews with the boys revealed that they have difficulty regulating their emotions and managing conflict with their partners, especially when they perceive infidelity. Interventions that strengthen boys’ abilities to identify, regulate, and cope with their emotions could decrease IPV perpetration, leading to improvements in adolescent wellbeing and lowering the risk of HIV transmission.
Footnotes
Acknowledgments
The authors would like to thank the members of the study staff at PHRU and the University of the Witwatersrand, including Phumla Madi, Candice Ramsammy, Stefanie Vermaak, and Busisiwe Nkala-Dlamini. The authors would also like to thank all participants for their time and effort in this study.
Ethical Considerations
Approval was obtained from the ethics committee of the University of the Witwatersrand in South Africa (Approval ID: 191001) and by Stony Brook University in the United States (Approval ID: FWA# 00000125, IRB2019-00567).
Consent to Participate
Participants provided written consent to participate in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Mental Health of the National Institutes of Health under Award Number R01MH119878. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This paper uses data from a highly vulnerable population (i.e., minors with HIV) and their experiences with sensitive topics, including violence. Therefore, the data that support the findings from this study are not publicly available to protect participant privacy.