
Abstract
Responses to sexual victimization disclosure play a significant role in recovery. In a sample of 138 survivors who disclosed their experience both online and in-person, the current study examined the association between online social reactions to the disclosure of sexual victimization and symptoms of posttraumatic stress disorder (PTSD) while accounting for social reactions to in-person disclosure and sexual victimization severity. Multivariate regression analyses indicated receiving in-person responses involving unsupportive acknowledgment, as well as receipt of online social reactions to disclosure via #MeToo that made fun, insulted, or said something to hurt the survivor were associated with increased PTSD symptoms.
The occurrence of sexual victimization is a significant public health problem (Dworkin et al., 2023; Fedina et al., 2018). Sexual victimization involves any attempted or completed sexual act, ranging from unwanted sexual contact to rape, that is committed against someone without a person's freely given consent (Basile et al., 2014; World Health Organization, 2017). According to the National Intimate Partner and Sexual Violence Survey (Smith et al., 2018) 43.6% of women (nearly 52.2 million) and 24.8% of men (nearly 27.6 million) within the United States experience some form of unwanted sexual contact in their lifetime. Sexual victimization is associated with a range of negative psychological consequences, particularly symptoms of posttraumatic stress disorder (PTSD; Dworkin, 2020; Khadr et al., 2018). A meta-analysis of 22 studies examining the intersection of sexual victimization and PTSD found that 74.6% of individuals met the diagnostic criteria for PTSD in the first month following sexual victimization, and 41.5% met the diagnostic criteria for PTSD one year following the event (Dworkin et al., 2023). Thus, research that seeks to identify factors that contribute to PTSD symptoms following sexual victimization is important for understanding how best to support survivors in recovery.
How others respond to the disclosure of sexual victimization plays a salient role in healing from sexual trauma (Dworkin et al., 2019). When disclosing personal experiences of sexual victimization, survivors often receive a combination of both positive and negative reactions from others (Ullman, 2023). Positive social reactions to disclosure of sexual victimization include providing legal, medical, or other kinds of resources as well as providing emotional support to the survivor (Ullman, 2000, p. 2023). Negative reactions to disclosure of sexual victimization include responses that blame the survivor fully or partially for the assault, attempt to control a survivor's decisions, attempt to distract the survivor from their experience or focus on supporting the needs of the disclosure recipient rather than the survivor (Ullman, 2000, p. 2023).
It is important to note that research on social reactions to disclosure of sexual victimization first developed in an era when social media and online forums were not yet widespread. Thus, early conceptualizations of the ways in which others respond to disclosure of sexual victimization were specific to conversations that occurred in person. However, numerous studies now document the use of social media to disclose experiences of sexual victimization; potentially to connect with others (Abavi et al., 2020; Fawcett & Shrestha, 2016; Lowenstein-Barkai, 2021; Masciantonio et al., 2021; Mendes et al., 2019; Moors & Webber, 2013; O’Neill, 2018; Webber & Wilmot, 2012; Yeo & Chu, 2024). The #MeToo movement, initiated by Tarana Burke's use of the hashtag #MeToo on MySpace in 2006 (JustBe Inc., 2006), catalyzed a significant increase in online disclosures of sexual victimization in 2017 following an exposé published by The New York Times on Harvey Weinstein's alleged sexual misconduct (Kantor & Twohey, 2017). In response, actress Alyssa Milano tweeted, “If you’ve been sexually harassed or assaulted, write ‘me too’ as a reply to this tweet,” a call to action that resulted in approximately 85 million social media posts featuring the #MeToo hashtag within 45 days (Sayej, 2017). Accordingly, research has now begun to explore the ways in which social reactions to online disclosure of sexual victimization might vary from social reactions to disclosure that occurs in person, as well as the impact of online disclosure on psychological well-being (Bogen et al., 2021a, 2021b).
Like conceptualization of in-person social reactions to disclosure of sexual victimization, social reactions to the disclosure of sexual victimization online reflect both positive as well as negative reactions (Bogen et al., 2019; Gorissen et al., 2021; Gundersen & Zaleski, 2020; Hosterman et al., 2018; Loney-Howes, 2018; Manikonda et al., 2018; Schneider & Carpenter, 2020). In an examination of 1,660 posters using the hashtag #MeToo, Bogen and colleagues (2021a) reported that whereas some X (formerly Twitter) users provided positive reactions (e.g., expressing validation and belief), some users responded with negative reactions (e.g., egocentric and distracting reactions). Another examination of 2,102 social media posts in response to the hashtag #MeToo found that 42.2% of posts were classified as positive social reactions (e.g., expressing validation and belief, advocating for social change) whereas 14.2% were classified as negative social reactions (e.g., egocentric reactions, disbelief) (Schneider & Carpenter, 2020). Given that survivors of sexual victimization may disclose – and receive reactions to disclosure – both in person and online, it is important that research explore how survivors are impacted in each of these contexts.
Numerous studies suggest that social reactions to in-person disclosure of sexual victimization influence healing following sexual trauma (Dworkin et al., 2019). Empirical evidence demonstrates that increased negative reactions to in-person disclosure are associated with increased PTSD symptoms (Bhuptani & Messman, 2021; Dworkin et al., 2019; Littleton, 2010; Orchowski et al., 2013; Ullman & Peter-Hagene, 2014; Ullman & Relyea, 2016). Longitudinal studies also show that receipt of higher levels of negative social reactions to in-person disclosure of sexual victimization are associated with increased PTSD symptoms over time (Andrews et al., 2003; Ullman & Peter-Hagene, 2014; Zoellner et al., 1999). In contrast, studies examining the association between positive social reactions to in-person disclosure of sexual victimization and PTSD symptoms show mixed results (Ahrens, 2006; Campbell et al., 2001; DiMauro & Renshaw, 2021; Orchowski & Gidycz, 2015; Sigurvinsdottir & Ullman, 2016; Ullman & Peter-Hagene, 2014, 2016). Specifically, whereas a small portion of studies document a negative association between positive social reactions and PTSD symptoms (e.g., Sigurvinsdottir & Ullman, 2016), most cross-sectional studies document no association between positive social reactions and PTSD (Littleton, 2010; Orchowski & Gidycz, 2015; Ullman, 2010; Ullman & Relyea, 2016). Although some studies report positive cross-sectional associations between positive social reactions and worsened psychopathology (DiMauro & Renshaw, 2021; Ullman, 1996; Ullman & Peter-Hagene, 2016), such associations are rendered to non-significant when examined in a prospective design (Ullman & Peter-Hagene, 2016).
A small number of research studies also document the impact of social reactions to online disclosure of sexual victimization. Specifically, four qualitative studies have examined the impact of social reactions to online disclosure of sexual victimization (Barta, 2019; Gundersen & Zaleski, 2020; Loney-Howes, 2018; PettyJohn et al., 2022). Survivors noted that receiving positive reactions to online disclosure of sexual victimization led to increased validation and decreased shame about the experience (Gundersen & Zaleski, 2020; Loney-Howes, 2018). Another study found that negative social reactions to online disclosure were perceived to be harmful and discouraged survivors from telling others in the future (Barta, 2019). Research also indicates that survivors may experience distress upon witnessing negative social reactions toward online disclosures by other survivors of sexual victimization (PettyJohn et al., 2022). The impact of negative reactions on survivors’ well-being is particularly concerning as studies have found that social media users who engaged in harmful negative responses, such as victim-blaming, were more likely to be retweeted and have more followers relative to social media users who shared positive reactions (Stubbs-Richardson et al., 2018).
Whereas the aforementioned qualitative studies provide information to characterize the impact of positive and negative reactions to online disclosure of sexual victimization, quantitative studies examining these constructs are currently lacking. In fact, to our knowledge, only one study (masked citation) has examined the impact of social reactions to online disclosure of sexual victimization on psychological outcomes and found that negative reactions to online disclosure were positively associated with increased PTSD symptoms, even after controlling for sexual victimization severity. However, this study only examined social reactions to online disclosure in the context of sexual victimization severity. Survivors may have disclosed in-person and online and thus, received reactions upon both types of disclosures. Indeed, studies find that nearly half of the survivors who disclosed their experience online had disclosed before in-person (Moors & Webber, 2013; Webber, 2014; Webber & Wilmot, 2012). Thus, it is important to investigate whether social reactions to online disclosure have an impact on psychological outcomes, even after controlling for the impact of social reactions received upon in-person disclosure.
Purpose of the Current Study
The current study aimed to investigate the impact of social reactions to online disclosure of sexual victimization, while accounting for other social reactions to in-person disclosure and sexual victimization severity. Given the limited prior research on the impact of social reaction to the online disclosure of sexual victimization, we expected that results would mirror prior studies addressing the association between social reactions to in-person disclosure of sexual victimization and PTSD among survivors of sexual victimization (Dworkin et al., 2019). Specifically, we hypothesized that accounting for in person reactions to disclosure, higher levels of negative social reactions to online disclosure of sexual victimization will be associated with elevated PTSD symptoms while accounting for sexual victimization severity.
Methods
Participants
Participants were recruited via social media platforms. Participants were required to report being 18 or older to participate. In total, 17.99% (n = 138) of participants within the total sample (N = 767) reported past disclosure of an unwanted sexual experience both online using #MeToo and in-person. Most participants were college educated: 5.8% (n = 8) possessed an associate degree; 35.5% (n = 49) a bachelor's degree; 23.9% (n = 33) a master's degree; 0.7% (n = 1) a doctorate degree; and 2.9% (n = 4) had undergone post-doctoral training. Of the remaining participants, 2.9% (n = 4) reported having trade/technical/vocational training, 6.5% (n = 9) a high school diploma or equivalent, and 4.3% (n = 6) some high school education. Most participants in the sample self-identified as White (58.0%, n = 80), with remaining participants self-identifying as Black (5.1%, n = 7), Latinx or Hispanic (8.7%, n = 12), Native American/American Indian (7.2%, n = 10), Asian/Pacific Islander (2.9%, n = 4), and multiracial (1.4%, n = 2), with 0.7% preferring not to answer (n = 1) and 2.9% (n = 4) listing “other” as their race. A majority of participants self-reported identifying as cisgender women (74.6%, n = 103), with other participants identifying a nonbinary (15.2%, n = 21), cisgender men (5.1%, n = 7), transgender men (3.6%, n = 5), and “other” (1.4%, n = 2). In regards to sexual identity, participants self-identified as heterosexual (38.4%, n = 53), bisexual (35.5%, n = 49), pansexual (10.1%, n = 14), lesbian (5.1%, n = 7), gay (2.9%, n = 4), and asexual (0.7%, n = 1). Additionally, participants listed “other” (5.8%, n = 8) and “prefer not to answer” (1.4%, n = 2) in regards to sexual identity.
Procedure
All study procedures received approval from the Institutional Review Board. Participants were recruited via social media advertisements within the United States. Compensation consisted of a $10 Amazon gift card. RedCap was used in the study for survey distribution. Participants were provided a detailed informed consent document and were required to consent to participate in the study before accessing survey items.
Participants were required to check a reCAPTCHA box before accessing survey items to prevent the possibility of bots. Researchers conducted a quality control check, which included examining each response and flagging suspicious response patterns (e.g., inconsistent or nonsensical answers in open-text fields, selecting the same option for every question), inconsistencies, and suspected ballot stuffing (i.e., one respondent completing the survey multiple times). Any survey that was flagged with at least one response quality concern was omitted in the analysis of data. Of the responses collected, 64.3% (n = 767) out of the total 1,191 responses passed the quality control check.
Measures
Sexual Victimization Severity
To determine participants’ experience of sexual victimization, as well as the severity of such experiences, the study used The Sexual Experiences Survey-Short Form (SES-SFV; Johnson et al., 2017; Koss et al., 2007). The SES-SFV assesses experiences of unwanted sexual contact since the age of 14 via self-report. Widely recognized as the gold standard in sexual victimization research, the SES-SFV is a valid and reliable measure of sexual victimization (Johnson et al., 2017; Koss et al., 2007). Participants had to report having at least one sexual victimization experience (i.e., unwanted sexual contact/sexual coercion or attempted rape/rape) to be eligible for the present study.
Symptoms of Posttraumatic Stress Disorder
A six-item abbreviated version of the PTSD Checklist (PCL-6) was used to assess symptoms associated with posttraumatic stress disorder (Lang & Stein, 2005; Lang et al., 2012). Each of the six items is a 5-point Likert scale ranging from 1 (not at all) to 5 (extremely), with higher scores indicating higher levels of symptoms. A mean score and Cronbach's alpha (α = 0.87) were both calculated. The PCL-6 has demonstrated good reliability and validity as a brief screening tool for PTSD symptoms in prior studies (Han et al., 2016; Lang et al., 2012).
Disclosure of Sexual Victimization
A single-item question assessed past occurrence and medium (i.e., in-person and/or online via MeToo) of participants’ disclosure of unwanted sexual experiences. The measure asked participants, “Earlier in the survey, you shared that you had an unwanted sexual experience. Have you told anyone about this experience? Please indicate whether you told anyone in-person (only), online via MeToo (only), both in-person and online via MeToo, or never (not at all).” Participants were then instructed to choose from one of the following four responses: “No, I did not disclose online via MeToo nor have I told anyone in-person,” “Yes - I disclosed in-person, but NOT via MeToo,” “Yes - I disclosed online via MeToo but NOT in-person,” and “Yes - I disclosed in-person AS WELL AS online using MeToo.”
In-Person Social Reactions to Disclosure
To understand the social reactions participants received upon disclosure of their sexual victimization experience (s), the current study used The Social Reactions Questionnaire-Shortened (SRQ-S) (Ullman et al., 2017). Participants were specifically asked, “The following is a list of reactions that other people sometimes have when responding to a person with this experience. Please indicate how often you experienced each of the listed responses from other people.” Three subscales make up the SRQ-S: Turning Against, Unsupportive Acknowledgment, and Positive Reactions. Items on the measure were 5-point Likert scale from 1 (never) to 5 (always). Subscale scores were used to calculate the average of subscale items. Both the SRQ-S Turning Against subscale and the SRQ-S demonstrated good internal consistency in the current sample (α = 0.91, α = 0.77). The SRQ-S Positive Reactions, relabeled the “general emotional and informational support” subscale, displayed acceptable internal consistency (α = .72). Prior studies have documented the reliability and validity of the SRQ-S (Forkus et al., 2024; Salim et al., 2022).
Online Social Reactions to Disclosure
The Online Social Reactions Questionnaire (OSRQ) was used to assess additional social reactions unique to online spaces. The OSRQ was developed for the present study and consists of 24 brief items. The 24 items consist of items from the SRQ modified to be specific to online social reactions, as well as items generated from prior qualitative findings regarding online social reactions to sexual victimization disclosure (Bogen et al., 2019). For the generated items, participants indicated responses on a 5-point Likert scale from 1 (never) to 5 (always) to eight items: “Shared a relevant link with you,” “Shared your tweet (s) with other people,” “Retweeted your #MeToo tweet (s),” “Liked your #MeToo tweet (s),” “Directed you to a web page of resources,” “Shared their own experience with you in solidarity,” “Made fun of you, insulted you, or said something to hurt you,” and “Defended you to other people.” To create the provision of online resources subscale, two items were grouped together based on Ullman's seminal social reactions research (Ullman, 2000): “Shared a relevant link with you” and “Directed you to a web page of.” The average of the two subscale items were used to calculate the subscale score. In the current sample, the provision of online resources subscale demonstrated good reliability (α = .81). An emotional support subscale was similarly created through grouping items “Liked your #MeToo tweet (s),” “Shared their own experience with you in solidarity,” and “Defended you to other people.” The subscale score, also calculated using the average of subscale items, demonstrated adequate reliability (α = .64). The three remaining items (“Made fun of you, insulted you, or said something to hurt you,” “Retweeted your #MeToo tweet (s),” “Shared your tweet (s) with other people”) were individually analyzed. Both the OSRQ-S online-turning against and the OSRQ-S online-unsupportive acknowledgment subscales demonstrated good internal consistency (α = .91, α = .89) in the current sample. The OSRQ-S positive reactions subscale, hereby referred to as “online-general emotional and informational support” to distinguish the items from other online social reactions assessments, demonstrated acceptable internal consistency (α = .78).
Data Analysis Plan
Bivariate correlations among all variables of interest (sexual victimization severity, online social reactions, in-person social reactions, and PTSD symptoms) were calculated. Prior to conducting the multivariate linear regression analysis, assumptions of linear regression (e.g., normality of residuals, lack of multicollinearity, and homoscedasticity) were checked. A linear regression was used to examine the association between the dependent variable (PTSD symptoms) and independent variables (sexual victimization severity, in person social reactions to disclosure, and online social reactions). The independent variables were entered using ENTER method.
Results
Descriptive Statistics and Bivariate Correlations
Descriptive statistics of key study variables among individuals with sexual victimization experiences and who disclosed using #MeToo are presented in Table 1. Among the study sample of individuals who disclosed sexual victimization online using #MeToo and/or disclosed sexual victimization in person (N = 138), the attempted rape/rape (86.2%, n = 119), and the remaining experienced unwanted sexual contact/sexual coercion (13.8%, n = 19). Bivariate correlations among study variables are presented in Table 1. In-person reactions involving turning against the survivor (r = .43) and providing unsupportive acknowledgment (r = .43) were positively associated with PTSD symptoms. The following online reactions were associated with PTSD symptoms: online reactions that involve turning against the survivor (r = .28), online reactions involving unsupportive acknowledgment (r = .23), and reactions involving making fun of reactions, insulting them, or saying something to hurt them (r = .36). No other negative or positive reactions were associated with PTSD symptoms. Notably, online turning against the survivor social reaction and online unsupportive acknowledgment were highly correlated (r = .84).
Bivariate Correlations and Descriptive Statistics.
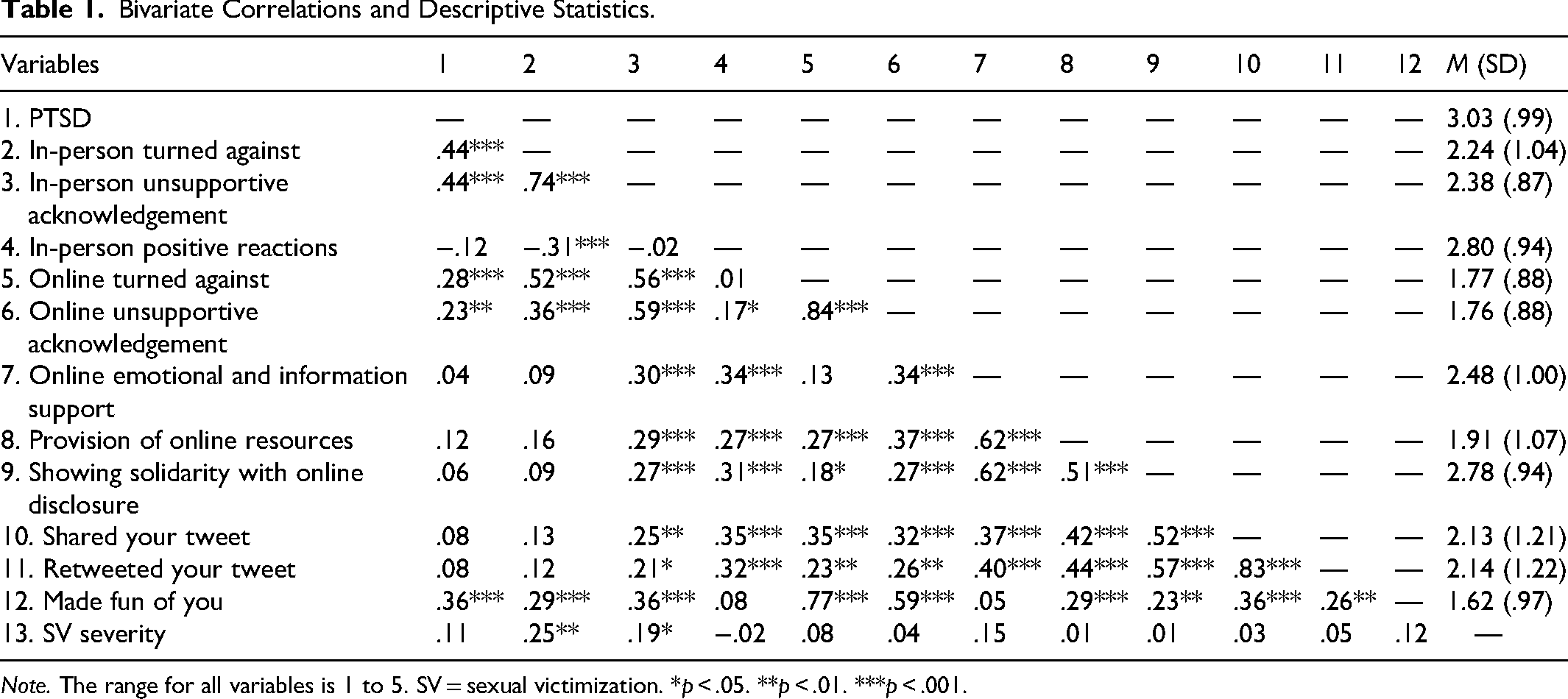
Note. The range for all variables is 1 to 5. SV = sexual victimization. *p < .05. **p < .01. ***p < .001.
Linear Regression
Prior to conducting a linear regression analysis, assumptions of linear regression (e.g., normality of residuals, lack of multicollinearity, and homoscedasticity) were checked. The normality of residuals for the dependent variable was confirmed visually via a normal P–P plot of standardized residuals, which showed points that were not completely on the line, but close. A visual screen of the scatterplot suggested the data were homoscedastic as the scatter plot took the (approximate) shape of a rectangular; scores were concentrated in the center (about the zero point and less than the absolute value of 3) and distributed in a rectangular pattern. The diagnostic checks indicated no serious violations of the assumptions for linear regression, suggesting that the model was appropriate for the data (Casson & Farmer, 2014).
The variance inflation factor (VIF) values for all variables (except for online turned against) ranged from 1.9 to 5.7, indicating a lack of multicollinearity (Vittinghoff et al., 2006). However, the VIF value for online turned against reaction was 8.64. The high VIF value combined with a high correlation value between online turned against social reaction and online unsupportive acknowledgement social reaction (r = .84) indicated multicollinearity. Thus, the online turned against response was removed from the model.
A simple linear regression was used to examine associations between PTSD symptoms (dependent variable) and in-person and online social reactions to assault disclosure (independent variables) along with sexual victimization severity (independent variable). The overall model was significant (F [11, 124] = 4.82, p < .001), with the predictors in the model accounting for 30% of the variation in PTSD symptoms (see Table 2). Specifically, in the presence of the other predictors, only in-person reactions involving unsupportive acknowledgment (b = .36, SE = .15, p = .02) and online reactions involving making fun of the survivor, insulting them or saying something to hurt them (b = .38, SE = .11, p < .001) were positively associated with PTSD symptoms.
Multivariate Linear Regression (N = 138).
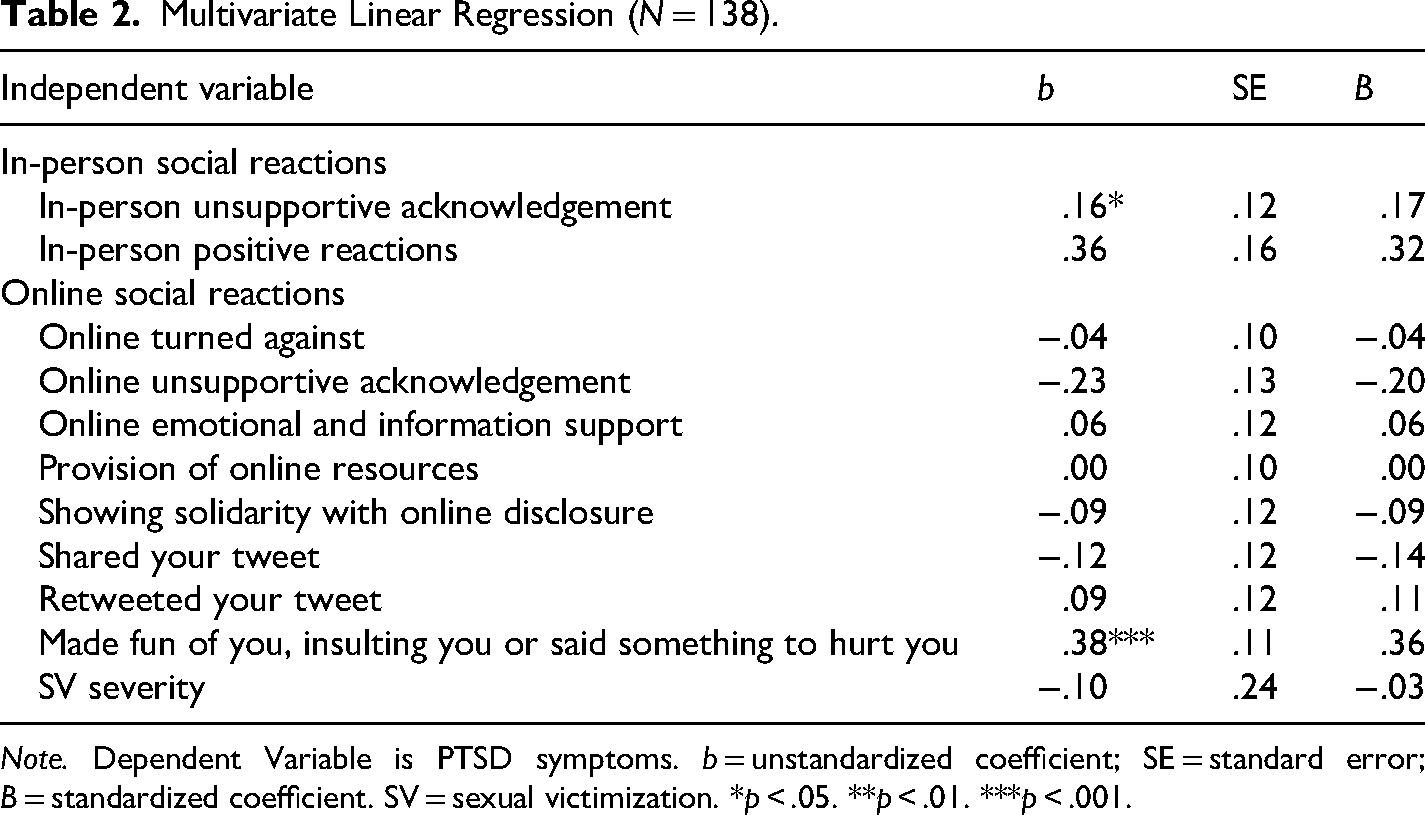
Note. Dependent Variable is PTSD symptoms. b = unstandardized coefficient; SE = standard error; B = standardized coefficient. SV = sexual victimization. *p < .05. **p < .01. ***p < .001.
Discussion
The current study investigated the impact of social reactions to online disclosure of sexual victimization on PTSD symptoms, while accounting for social reactions to in-person disclosure and sexual victimization severity. Given that survivors of sexual victimization may disclose both online and in person, ensuring that examination of the impact of social reaction attends to both in-person and online disclosure experiences is an important advancement in the field. Several notable findings were revealed.
Multivariate linear regression revealed that in-person responses involving unsupportive acknowledgment and online social reactions that included making fun of the survivor were associated with higher PTSD. The current literature suggests that any negative reaction to in-person disclosure is associated with increased PTSD symptoms (Bhuptani & Messman, 2021; Dworkin et al., 2019; Littleton, 2010; Orchowski et al., 2013; Ullman & Peter-Hagene, 2014; Ullman & Relyea, 2016) even despite controlling for survivors’ sexual victimization severity (Littleton, 2010; Ullman et al., 2007a). Findings highlight the detrimental impact of both in-person and online negative social reactions. Negative responses to survivors often reflect the broader societal stigma surrounding sexual assault (Krahé et al., 2008; McKimmie et al., 2014). These responses are particularly concerning, as research has shown that social media users who engage in harmful behaviors—such as posting negative or abusive comments—online tend to have more followers and are more likely to be retweeted than those who offer supportive reactions (Stubbs-Richardson et al., 2018). Scholars have documented that the anonymity afforded by social media platforms often encourages such harmful behaviors, enabling users to mock, insult, or attack survivors without the fear of direct accountability (Barlett & Gentile, 2012; Barlett et al., 2016; Diakopoulos & Naaman, 2011; Lapidot-Lefler & Barak, 2012). Our results in conjunction with prior literature (Dworkin et al., 2019) emphasizes the serious implications of negative social reactions to victimization disclosure for survivors’ mental health.
It is important to note that participants in the current sample had primarily experienced more severe types of sexual victimization such as rape and attempted rape (n = 119). Despite this higher level of severity, not all types of negative social reactions were associated with PTSD symptoms. It is possible that participants shared disclosure experiences that happen much longer after their most severe sexual victimization experience and as such it did not affect their PTSD symptomatology significantly. Indeed, many survivors of sexual violence do not go on to develop PTSD or PTSD symptoms (Dworkin et al., 2023). Additionally, it is possible that survivors that have worse PTSD symptomatology might not be willing to participate in a study on sexual victimization disclosure online or in-person.
Whereas the literature is mixed (Ahrens, 2006; Campbell et al., 2001; DiMauro & Renshaw, 2021; Orchowski & Gidycz, 2015; Sigurvinsdottir & Ullman, 2016; Ullman & Peter-Hagene, 2014, 2016), our findings are consistent with prior work that have shown no association between positive in-person social reactions and PTSD (Littleton, 2010; Orchowski & Gidycz, 2015; Ullman, 2010; Ullman & Relyea, 2016). Our work adds to the literature by documenting that there was no association between positive online social reaction to disclosure and PTSD symptoms. Research with a larger sample size is needed to replicate this finding. Although positive in-person or online reactions may not demonstrate an association with PTSD, positive social reactions may still be helpful for survivors by increasing validation and decreasing shame around their sexual victimization experience (Gundersen & Zaleski, 2020; Loney-Howes, 2018). More work may be needed to understand whether receiving in-person and online positive social reactions may have an effect on other factors, such as post-traumatic growth.
The current findings have several implications. It may be useful for mental health providers, especially those working with sexual victimization survivors, to be mindful of the social contexts in which individuals disclose their experiences. Mental health professionals should explore how survivors have sought support online and assess whether these experiences have been beneficial or detrimental to their recovery. If disclosing experiences in online forums proves harmful, providers may assist survivors in setting boundaries around their social media use. It may also be helpful for survivors to process any negative reactions they have received online and to build stronger, more supportive networks. Even if survivors do not share their own experiences online, they may still witness harmful social reactions directed at other survivors in digital spaces. In fact, a qualitative study revealed that survivors can experience psychological distress simply by observing negative reactions toward fellow survivors of sexual assault (PettyJohn et al., 2022).
Limitations and Future Directions
This study is not without limitations. First, this is a cross-sectional data set, and as such, causality cannot be assumed from the study findings. Second, most participants reported more severe types of sexual victimization, and as such results of the current study may not generalize to survivors with less severe types of sexual victimization. Third, we exclusively looked at social reactions that were only negative or positive, and it is possible that survivors received other types of reactions that would not neatly fall into the negative or positive binary. Indeed, there is some data that suggests that survivors do not perceive social reactions as binary (positive/negative) (Campbell et al., 2001). It may be more important to consider the relationship the survivor has with the person they are disclosing to as this may be more salient to survivors’ recovery. For example, a supportive reaction from a close friend may be more meaningful to a survivor than a negative reaction from a stranger. This explanation is speculative, and empirical research needs to be conducted to examine whether the relationship with the survivor influences the perception of responses received. Furthermore, future research may endeavor to examine negative reactions and PTSD symptoms closer in time to the sexual victimization experience (at least 3 months after) to determine whether there is a true association present. Lastly, we did not specifically examine the length of time between victimization and disclosure, which could influence the relationship between disclosure reactions and PTSD symptoms (e.g., Ullman et al., 2007b). Thus, future studies could benefit from investigating the impact of time since victimization on the outcomes we observed. As such, the potential role of the time between victimization and disclosure should be considered as a plausible but untested explanation for our results
Footnotes
Ethical Considerations
The Rhode Island Hospital Institutional Review Board [Protocol Number: 1472511] approved the study.
Consent to Participate
All participants provided written informed consent prior to participation.
Consent for Publication
Not applicable
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Efforts on this publication was supported by the National Institute on Drug Abuse (NIDA; K99DA057993; PI: Bhuptani, Principal Investigator).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.