
Abstract
Intimate partner violence (IPV) is a preventable public health problem with documented negative effects on well-being. The perinatal period represents a time of increased stress for partners, which can increase the likelihood of IPV. Economic support policies, like paid family leave (PFL), may reduce family violence, including IPV. Using data from the Pregnancy Risk Assessment Monitoring System, we examine the association between receipt of PFL and IPV for women employed during the perinatal period. Results indicate reduced odds of IPV for employed women who received PFL. PFL may reduce IPV victimization for women employed during the perinatal period.
Introduction
Intimate partner violence (IPV) is a common, yet preventable, public health problem in the United States with lasting effects for individuals and for society (Niolon et al., 2017). Efforts to eradicate its occurrence have primarily focused on treatment and protection for victims and legal sanctions for perpetrators. However, less has been done to reduce IPV victimization. Recently, concrete and economic support policies, such as paid family leave (PFL), have been explored as potential strategies for addressing key risk factors (i.e., financial stress) for family violence (Bullinger et al., 2024). Early findings suggest that PFL is associated with reductions in family violence, including abusive head trauma (Klevens et al., 2016) and infant maltreatment (Tanis et al., 2024). In this article, we explore the association between the receipt of PFL and IPV victimization for women employed during the perinatal period (i.e., from pregnancy to postpartum) using data from the Pregnancy Risk Assessment Monitoring System (PRAMS). Further, we examine the role of relational conflict (i.e., arguing) as a potential mediator of this association.
Background and Significance
IPV Victimization and Prevention
IPV refers to “any physical or sexual violence, stalking, and/or psychological aggression by a current or former dating partner” (Leemis et al., 2022). IPV can occur at multiple points within one's life and happen in all types of relationships, including heterosexual and same-sex relationships (Leemis et al., 2022). Data from the National Intimate Partner and Sexual Violence Survey (NISVS) suggest that nearly one in two women and one in four men report having experienced contact sexual violence, physical violence, and/or stalking from a partner in their lifetime, with many reporting that violence began before the age of 18 years (Leemis et al., 2022). The perinatal period, including the year before, the time during, and the year after pregnancy, represents a unique period of risk for IPV (Hahn et al., 2018). Population studies have estimated that between 3% and 9% of women experience IPV during the perinatal period (Saltzman et al., 2003; Silverman et al., 2006), compounding the stress felt by pregnant and parenting people.
IPV victimization increases the risk of adverse outcomes. For example, IPV victimization has been found to increase problems of mental health (e.g., posttraumatic stress disorder, depression), physical health (e.g., cardiovascular, reproductive issues), and health risk behaviors (e.g., smoking, binge drinking) (Breiding et al., 2008; Fogarty et al., 2023; Stubbs & Szoeke, 2022; Warshaw et al., 2009). Women who experience IPV seek prenatal care at a lower rate than their nonvictimized counterparts, which has deleterious implications for the pregnant person and their unborn child (Cha & Masho, 2014). In addition, IPV victimization during the perinatal period has been linked to adverse birth outcomes, including child death (Currie et al., 2022; Hahn et al., 2018).
To reduce IPV victimization, it is essential to identify and address risk and protective factors associated with its occurrence. Risk factors at the individual (e.g., history of violence in the family of origin, unemployment), relationship (e.g., conflict and discord), and community/societal (e.g., poverty, social norms) levels are associated with IPV (Niolon et al., 2017). A growing body of research continues to demonstrate that stress, particularly financial stress associated with conditions of poverty, is one of the key risk factors associated with multiple forms of violence, including child maltreatment and IPV (Niolon et al., 2017). Unemployment, low income, and poverty, all being forms of financial stress, have been shown to increase the likelihood of IPV (Ahmadabadi et al., 2020; Keilholtz et al., 2023). During the perinatal period, many of these risk factors can be magnified as partners navigate the physical, relational, and financial changes brought on by having a child. Addressing financial stress through social policies (e.g., PFL) has become a cornerstone of family violence prevention strategies (Fortson et al., 2016) in the United States. Yet, there is limited research on these social policies’ preventative efficacy, specifically for IPV.
Family Leave in the United States
The United States does not currently provide a universal, federal PFL benefit to workers. The Family Medical Leave Act (FMLA) is often touted as a solution, providing job protection for workers who experience the birth of a child or the need to care for themselves or a family member who is ill (Berger et al., 2005; Berger & Waldfogel, 2004; Winston et al., 2019). FMLA does not provide wage replacement for time taken, nor does it apply universally to all workers. To qualify for FMLA, certain conditions must be met, including working for an organization with over 50 employees for at least 1,250 h in the past 12 months. Only 59% of the workforce is eligible to access unpaid employment protection under the FMLA. A U.S. Department of Labor survey found that only 66% of respondents could afford to take unpaid time off work to care for a new child (Brown et al., 2020). For many families, especially those with low income, and those who otherwise do not meet the eligibility criteria, FMLA provides little to no financial relief following the birth of a child or in the unforeseen event of a medical emergency, highlighting the urgent need for a more comprehensive and inclusive federal PFL benefit.
Some private employers offer different types of paid leave for employees. However, only a quarter of private sector employees have access to employer-sponsored PFL, with under half having access to employer-sponsored short-term disability insurance (United States Department of Labor, Women's Bureau, 2024). Six percent of low-wage workers, predominantly women and workers of color, have access to PFL, with only 11% having access to short-term disability insurance. This disparity in access to paid leave further deepens the financial burden on low-wage workers, making it even more difficult for them to balance work and family responsibilities.
Increasingly, states are beginning to provide universal options for PFL separate from the benefits that workers receive through their employers. PFL generally refers to providing an employee with wage replacement for a predetermined amount of time (e.g., 6 weeks) following the birth of a child or for personal or family medical reasons. Fourteen states (i.e., CA, CO, CT, DC, DE, MA, MD, ME, MN, NJ, NY, OR, RI, and WA) have enacted state PFL options, providing some level of wage replacement to workers who temporarily leave the workforce for family or medical reasons. The comprehensiveness of these policies, including the length of leave, the percentage of wage replacement, and the definition of events qualifying for leave, varies by state (Bullinger et al., 2024).
PFL is associated with positive maternal and child outcomes (Bullinger et al., 2024). Winston et al. (2019) investigated maternal perceptions of how PFL aids low-income mothers in reentering the workforce after childbirth. This qualitative study found that PFL was essential for low-income mothers, as it provided supplemental income that allowed them to stay home with their newborns. This time was crucial not only for bonding with their children but also for physical recovery from childbirth. Additionally, PFL enabled mothers to establish breastfeeding routines and secure childcare arrangements before returning to work. Despite these benefits, the income support from PFL was often insufficient, leading many women to return to work earlier than desired.
PFL in California has been studied more than other state programs in the United States due to its early policy adoption. PFL in California has been shown to increase the duration of leave-taking among mothers by 3–6 weeks (Rossin-Slater et al., 2013), and leave-taking by both mothers and fathers independently (Baum & Ruhm, 2016). Parents were also more likely to take leave simultaneously (Bartel et al., 2018). Research indicates a strengthened link to the labor force due to PFL in the short-term (Baum & Ruhm, 2016; Byker, 2016; Rossin-Slater et al., 2013). However, findings regarding long-term maternal employment outcomes vary (Bailey et al., 2019; Baum & Ruhm, 2016; Rossin-Slater et al., 2013). Possibly because of higher employment rates, research suggests that the introduction of PFL boosted family income and decreased family poverty, particularly among single mothers with lower education and income levels (Stanczyk, 2019).
Moreover, after the introduction of PFL in 2004, California saw notable reductions in hospital admissions for abusive head trauma when compared to states lacking similar policies (Klevens et al., 2016). A national study using data from the National Child Abuse and Neglect Data System recently found that states with PFL have decreasing rates of infant child maltreatment following the implementation of the policy (Tanis et al., 2024). Despite growing evidence of concrete and economic support policies reducing child abuse and neglect (Fortson et al., 2016), less research has explored the role of these policies, like PFL, in reducing IPV. One exception from an Australian study found that women who received PFL benefits had lower odds of IPV victimization in the 12-month postpartum (Gartland et al., 2011). In this article, we focus explicitly on the role of PFL as a strategy for reducing IPV victimization for U.S. women employed during the perinatal period.
Family Stress Model
The Family Stress Model (FSM) (Masarik & Conger, 2017) explains the complex pathways leading from financial hardships in a family to interparental relationship problems and more severe forms of interparental conflict, such as IPV. In the FSM, experiences of unemployment, having insufficient income to pay for necessities, or lacking family-friendly work policies (e.g., paid time off and flexible work schedule) create economic pressures on the family as they struggle to pay bills, meet the needs of their children, and ensure safe care for their children to maintain employment. Masarik and Conger (2017, p. 86) note that these “economic pressures … give psychological meaning to financial hardship.” Parents, especially during the perinatal period, experience a considerable amount of distress trying to balance the material and emotional needs of the family. This distress can lead to conflict within intimate relationships. Knowing that one will receive paid leave after the birth of a child may reduce anticipatory stress during pregnancy (Farina et al., 2023). By reducing the anticipatory stress associated with impending economic hardship, it is possible that conflict within intimate relationships will lessen prior to the actual receipt of paid leave. It is therefore hypothesized that the effects of PFL may be observed during pregnancy, in addition to after birth, due to the reduction in anticipatory stress brought about by knowing that one will receive paid leave after the birth of their child.
In this article, we test the association between receipt of PFL and IPV for women employed during the perinatal period. Using the FSM, we hypothesize that the reduction in distress brought about by the receipt of PFL will reduce conflict in relationships, resulting in reduced IPV during the perinatal period.
Research Questions
Research Question 1: Compared to unpaid leave or no leave, is PFL associated with reduced odds of IPV victimization for women employed during the perinatal period? Research Question 2: Does arguing less with an intimate partner associate with both PFL and IPV victimization (provide partial evidence of mediation) for women employed during the perinatal period?
Method
Data
All study protocols were approved via an independent review board. Individual-level data for this study were obtained, with permission, from the PRAMS study. PRAMS is a self-reported, state-based survey of maternal behaviors, experiences, and health-related indicators before, during, and shortly after pregnancy (Shulman et al., 2018). Starting in 1987, PRAMS is an ongoing, collaborative research study between the Centers for Disease Control and Prevention (CDC) and individual state health departments. Participating regional sites include 47 states, the District of Columbia, Puerto Rico, and New York City. Birth-certificate-record-based recruitment is used to select samples representative of all women who delivered an infant each year (Shulman et al., 2018). The survey covers roughly 83% of all U.S. births, with a stratified design such that oversampling occurs for subpopulations of interest. Approximately 1,000–3,000 mothers per year per region participate. To date, this is a combined sample size of over one million mothers. A set of “core” items is asked in every participating region with a high degree of continuity across study phases. States frequently choose to include additional state-specific items referred to as “standard” questions. This study focuses on the association between mothers taking PFL and self-reported IPV during the perinatal period (i.e., from pregnancy through post-partum). Figure 1 outlines how we narrowed the entire PRAMS dataset to a subset of working mothers. Appendix A details the PRAMS work leave and IPV survey questions used to derive our final analytic sample.
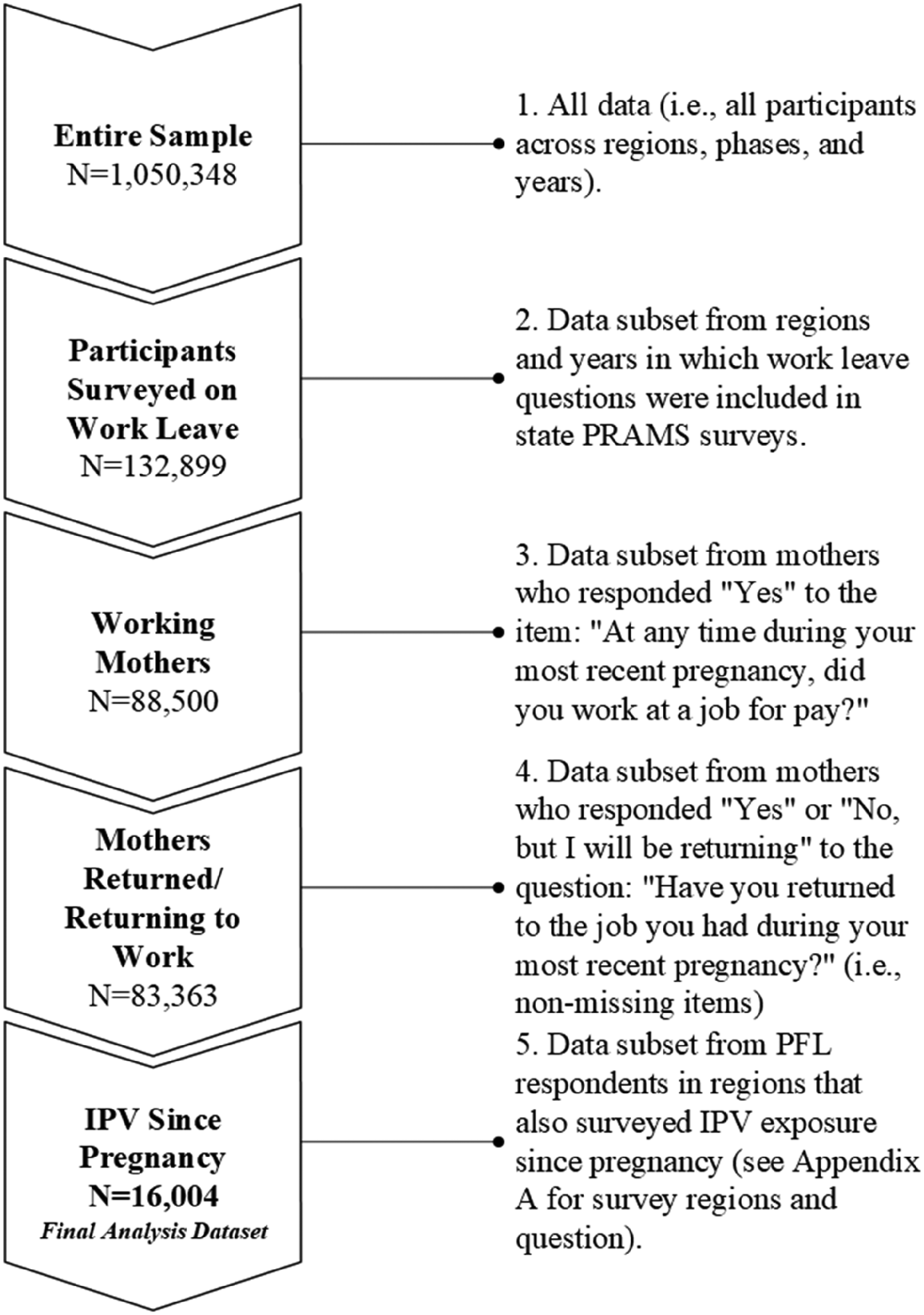
Describing the PRAMS analysis sample.
Measures
IPV during the perinatal period (primary outcome)
IPV victimization during pregnancy was measured using the following “core” item from PRAMS: “During your most recent pregnancy, did any of the following people [current or former husband or partner] push, hit, slap, kick, choke, or physically hurt you in any other way? For each person, check ‘No’ if they did not hurt you during this time or ‘Yes’ if they did.”
IPV victimization since pregnancy was measured using the following “standard” state-specific items. We selected these items because they were the only IPV “since pregnancy” items included in surveys from states that also had items regarding PFL. To further harmonize our measurement of IPV, we limit data from item response choices that were consistent across the two items (i.e., “yes” or “no”):
“This question is about things that may have happened since your new baby was born …” (AK, MD, NM, OH)
Used: “My husband or partner threatened me or made me feel unsafe in some way.” Used: “I was frightened for my safety or my family's safety because of the anger or threats of my husband or partner.” Used: “My husband or partner tried to control my daily activities, for example, controlling who I could talk to or where I could go.” Not used: “My husband or partner forced me to take part in touching or any sexual activity when I did not want to.” “During any of the following time periods, did your husband or partner threaten you, limit your activities against your will, or make you feel unsafe in any other way?” (LA, MN).
Not used: “During the 12 months before I got pregnant.” Not used: “During my most recent pregnancy.” Used: “Since my new baby was born.”
Any IPV reported (from the selected items above) during and/or since pregnancy was coded as 1, and no IPV reported during and/or since pregnancy was coded as 0.
PFL (primary predictor)
Family leave was considered paid leave (coded as 1) if mothers reported taking any paid leave, alone or in combination with unpaid leave (see coding strategy used in Hawkins, 2020). See above for state-specific options that were also considered “paid leave.” Mothers who took unpaid leave only or no leave (collapsed together due to small sample size) were considered as having taken no paid leave (coded as 0).
Arguing with partner (exploratory mediator)
One item from a collection of stressful life event questions concerning experiences during the 12 months before the baby was born was examined as a potential mediating factor: “I argued with my husband or partner more than usual.” Because this item surveys arguing behaviors in the 12 months prior to birth, we are unable to test for “pure” mediation effects. More exploratory analyses may prove helpful in identifying a potential candidate mechanism that supports our theoretical framework related to the FSM. This item was only asked during select years in each state, reducing the analytic sample size to N = 13,148:
Alaska (2012–2015) Louisiana (2016–2021) Maryland (2012–2015) Minnesota (2018–2021) New Mexico (2012–2015) Ohio (2012, 2014, 2015)
Control Variables
We selected covariates based on the relevant literature, in particular, those associated with PFL uptake, socioeconomic status, and child maltreatment (Dennison et al., 2022; Esposito et al., 2022). These covariates may not all be true confounders; however, in structural equation modeling (SEM), these variables may contribute to more precise estimates given their shared variance.
Socioeconomic status (SES) latent variable indicators. All indicators are coded in such a way that higher values indicate lower SES. Insurance/Medicaid status. PRAMS provides insurance/Medicaid status items at various perinatal timepoints. We used three insurance status variables for prenatal care, at birth, and for postnatal care. Insurance/Medicaid status at each perinatal time point was coded as “private insurance” = 0, “uninsured” = 1, or “Medicaid” = 2. We coded this way as Medicaid respondents reported the lowest income levels, followed by uninsured respondents. Family income as a percent of the federal poverty level. PRAMS items included data on family income and family size, which, in combination with the year of survey collection, we coded as a percentage of the federal poverty level (FPL), accounting for different FPL thresholds in Hawaii and Alaska. Family income ranges were specified in the item. We used the median income value for each income range to calculate the percent of FPL. This item was reverse-coded such that higher values indicated a lower income as a percent of FPL. Maternal educational attainment. Maternal educational attainment was coded as “college graduate” = 0, “some college” = 1, “high school/GED graduate only” = 2, and “less than high school/GED” = 3. Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). WIC was only asked consistently for the perinatal timepoint of “during pregnancy” and was coded as “not receiving WIC” = 0, “receiving WIC” = 1.
Manifest control variables. Additionally maternal marital status (“not married” = 0, “married” = 1), maternal age (PRAMS used age categories “≤17 years” = 1, “18–19 years” = 2, “20–24 years” = 3, “25–29 years” = 4, “30–34 years” = 5, “35–39 years” = 6, and “40+years” = 7), and maternal race/ethnicity were included as control variables. We followed the approach of Hawkins (2020), which examined disparities in maternal leave using PRAMS data, and categorized race/ethnicity as one dummy coded variable with the following categories: Hispanic or Latinx (Latino, Latina, and Spanish); Black, non-Hispanic; Asian, non-Hispanic; Native American/Alaskan Native/Hawaiian, non-Hispanic; and other/unknown/mixed race, non-Hispanic, with White, non-Hispanic as the referent. These racial categories provide a mutually exclusive means of coding race, consistent with the relevant literature (Hawkins, 2020).
Analysis
R statistical software, Version 4.3.2 (R Core Team, 2023), and Mplus version 8.10 (Muthén & Muthén, 1998–2017) were used. R was primarily used for data cleaning and coding, whereas Mplus was used for all modeling. We utilize two different methods of estimating (i.e., Average Treatment Effect [ATE]) of PFL on IPV during and/or since pregnancy. Converging results between the two methods would strengthen conclusions as well as provide a balance between the strengths and weaknesses of each approach individually. The first approach is a standard multiple regression with the inclusion of a latent variable capturing SES as a control variable (see Kline, 2023, for general information on SEM). The second approach uses the same variables, but instead of running a multiple regression, a propensity score analysis with inverse probability weights (IPW) is used. Both models benefit from the use of a latent variable capturing SES. The benefits of including a latent variable are: (a) data dimension reduction (taking several indicators of SES and modeling just one latent variable), (b) adjustment of measure error (each manifest indicator of SES imperfectly measures the latent construct of SES), (c) reduction of omitted variable bias in propensity score analyses (Leite et al., 2019), and (d) missing data on SES manifest indicators is accounted for using full-information maximum likelihood estimation (Little et al., 2014). An additional reason for running a multiple regression with an SEM framework is the ability to model the effects of a potential mediator simultaneously. The methods of each approach are described below. For each analysis, appropriate sampling weights, strata, and cluster variables were utilized to account for the PRAMS complex survey design. Subpopulation commands were used so that the full sample of all participants in a given year and region was fed into Mplus, but only the select samples were used for analysis, thus preserving the correct adjustment for the complex survey design.
Regression Approach
Measurement model. First, each of the SES indicators listed above—which include binary, ordinal, and continuous variables—was modeled as one continuous latent variable through an unconditional confirmatory factor analysis (CFA) measurement model. Here, model fit statistics were examined to check for satisfactory model fit before including additional variables in a larger structural model (additional manifest control variables, a PFL predictor variable, and an IPV outcome variable). Weighted least squares (WLSMV in Mplus) was used as an estimator.
Structural models. Two regression models were fit. The first included IPV during and/or since pregnancy as a binary outcome with PFL as the primary predictor, controlling for SES as a latent variable, maternal age, maternal marital status, and dummy coded race/ethnicity variables. The probit (probit models are the only binary outcome models when running a WLSMV in Mplus) coefficient of PFL predicting IPV was the primary effect of interest. Next, a mediation model was run. This model included an “exploratory” mediator, “arguing with a partner” (i.e., IPV), regressed onto mediator, PFL, and control variables; and the mediator was regressed onto PFL and control variables. Indirect and direct effects were estimated by Mplus (i.e., the indirect effect of PFL on IPV via arguing with a partner) along with bootstrapped confidence intervals (N = 5,000 bootstrapping runs).
Propensity Score Weighting Approach
To estimate the ATE using a propensity score/IPW approach, we combined the methods described by Leite et al. (2019), which outlines how to conduct a propensity score analysis on a complex survey-designed study (e.g., PRAMS) with one or more latent covariates in Mplus (e.g., the use of SES as a latent variable), with the methods outlined by Nguyen and Stuart (2020), which make use of “inclusive factor scores.” Propensity score analyses with a latent variable model with inclusive factor scores (PSIF) have been shown to outperform other latent variable propensity score methods at reducing bias in the estimated “treatment” effects (see Nguyen & Stuart, 2020; Zhang & Leite, 2026). We carried out the following general steps to estimate the ATE using a PSIF approach with a complex survey methodology:
Run a conditional CFA (with the SES latent variable regressed onto all control variables listed above), and PFL regressed onto the latent variable and control variables, utilizing survey weights, strata, and cluster variables provided by PRAMS. “Factor scores” from this model were saved by Mplus. Regress PFL variable on covariates and the latent variable (using the saved “factor scores” from step 1), again using survey weights, strata, and cluster variables. “Propensity scores” from this model were saved by Mplus. Calculate inverse propensity weights and multiply them by the sampling weights provided by PRAMS. Use the new weighted data to check for a covariate balance between the paid and unpaid/no leave groups. Use the new weighted data to run a multiple-group analysis (i.e., paid vs. unpaid/no leave) to estimate the ATE by examining the mean difference in the IPV variable and obtain a P value from nested model comparison.
Results
For descriptive statistics, see Tables 1 and 2.
Univariate Proportions for Categorical Variables.
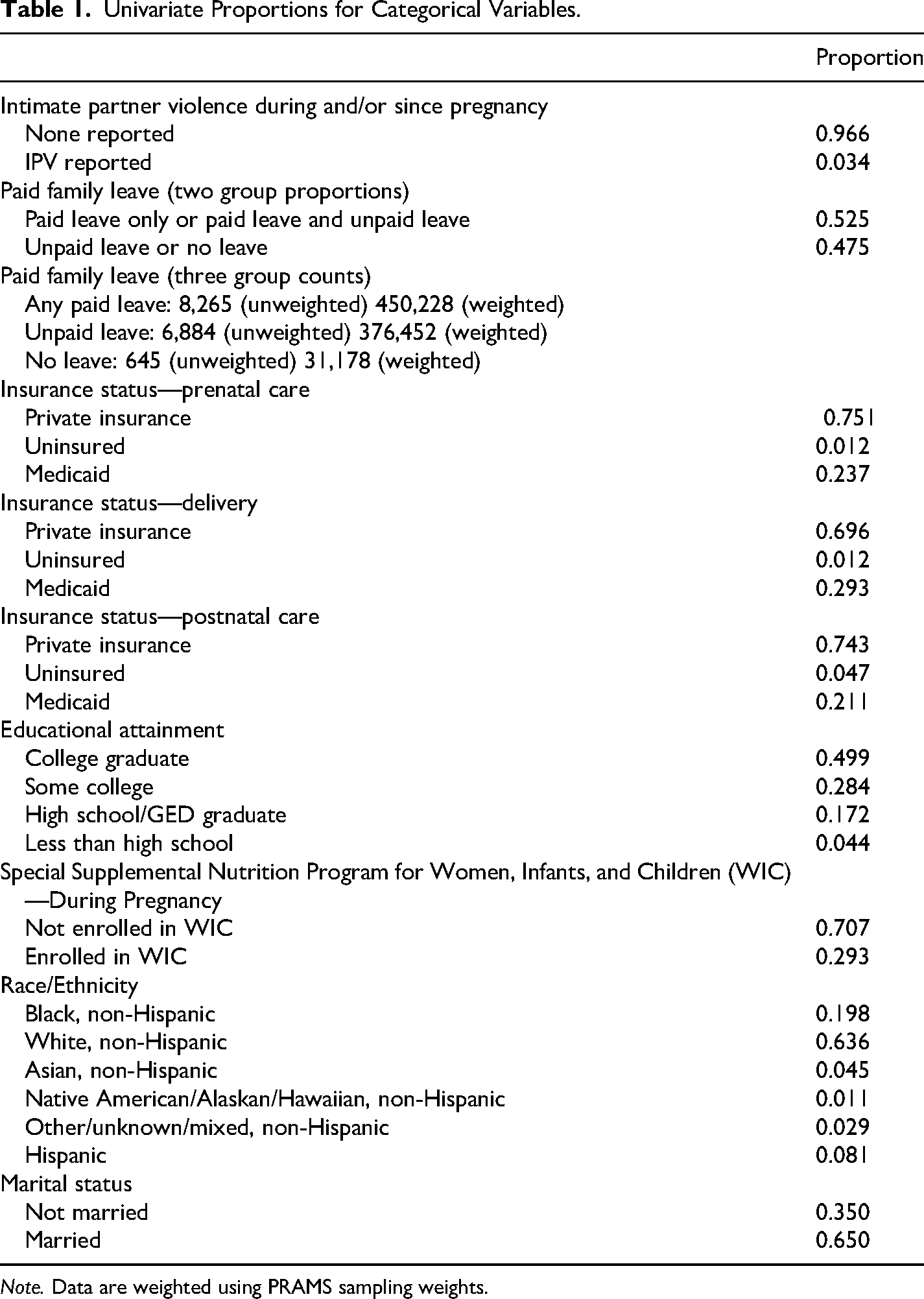
Note. Data are weighted using PRAMS sampling weights.
Descriptive Statistics for Continuous Variables.
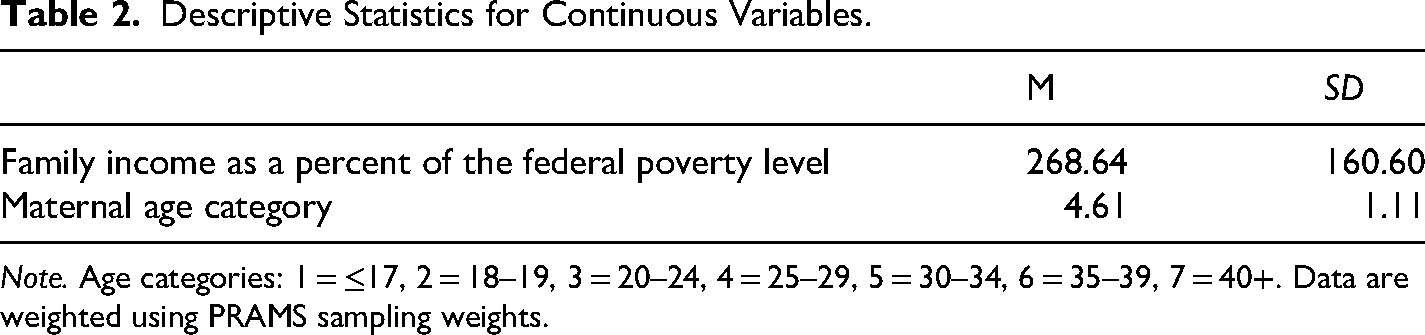
Note. Age categories: 1 = ≤17, 2 = 18–19, 3 = 20–24, 4 = 25–29, 5 = 30–34, 6 = 35–39, 7 = 40+. Data are weighted using PRAMS sampling weights.
CFA Measurement Model Results
A single, continuous latent variable representing SES was modeled in an unconditional CFA with the following observed indicators: insurance/Medicaid status for prenatal care (ordinal), insurance/Medicaid status at birth (ordinal), insurance/Medicaid status for postnatal care (ordinal), WIC status during pregnancy (binary), maternal education (ordinal), and family income as a percent of the FPL (continuous). Model fit was adequate/good with a RMSEA = 0.058, CFI = 0.998, TLI = 0.997, SRMR = 0.028. However, as is common with large sample size CFAs, the Chi-Square test of model fit for the baseline model was equal to 272379.116, with 15 degrees of freedom and a P < .0001. All standardized loadings were significant and ranged in size from 0.739 to 0.997. These can be difficult to interpret in a CFA that includes binary, ordinal, and continuous variables. However, the R-squared/explained variance of each indicator from the latent variable was all significant and ranged from 0.683 to 0.994.
Regression Model—Without Exploratory Mediation Results
For results of regression analyses, see Table 3. After adjusting for socioeconomic status, maternal age, marital status, and race/ethnicity, PFL was a significant predictor of IPV during or since pregnancy (probit coefficient = −0.189, 95% CI [−0.305, −0.074], P = .001). When we calculated model-based predicted probabilities, they indicated that mothers who took paid leave had an estimated IPV probability of 2.4%, compared to 3.7% among mothers who took unpaid leave or no leave. This corresponds to an average marginal effect of −1.23 percentage points, representing approximately a 33% lower predicted probability of IPV victimization among mothers who took paid leave. In a sensitivity analysis, using model constraints and a dummy coded variable, paid leave (vs. no leave) was associated with reduced IPV during/since pregnancy (b = −0.316, SE = 0.134, P = .018). Unpaid leave (vs. no leave) did not exhibit a statistically significant effect (b = −0.145, SE = 0.131, P = .269). Finally, a direct contrast between paid leave and unpaid leave indicated that paid leave had a significantly stronger protective association than unpaid leave (b_paid − b_unpaid = −0.171, SE = 0.059, P = .004; 95% CI [−0.287, −0.055]).
Structural Model Results.
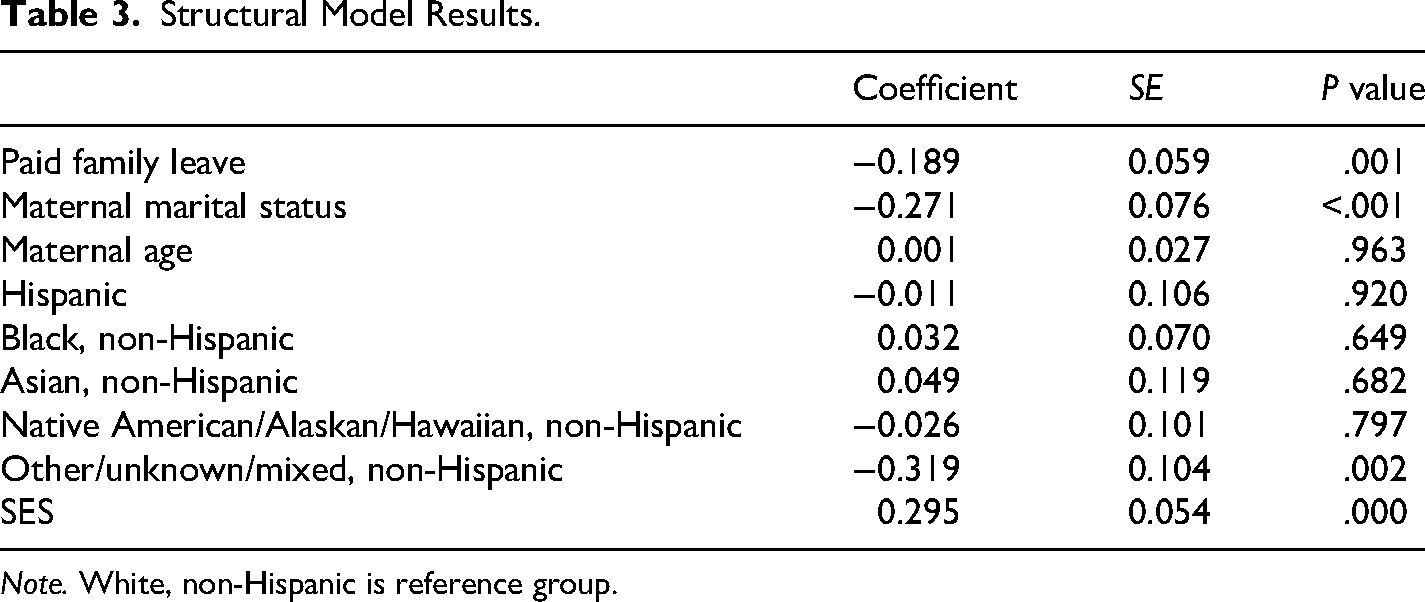
Note. White, non-Hispanic is reference group.
Regression Model—With Exploratory Mediation Results
For the results of the mediation analysis, see Table 4. A stressful life event item measuring whether mothers reported arguing with their partner more frequently in the 12 months before their baby was born was used as a mediator in our second regression analysis. This was done simply by adding this new mediator to the model presented above. Using N = 5,000 bootstrapped confidence interval estimation, the indirect effect (i.e., mediation effect) estimate was −0.062 (95% CIs [−0.101, −0.018]) (P = .008). The direct effect (i.e., remaining association between PFL and IPV victimization after accounting for the mediator) was −0.125 (95% CIs [−0.275, 0.029]) and not significant (P = .106). This nonsignificant direct effect and significant indirect effect implies a “full” mediation. However, we caution against using any strict casual inference, as these data are cross-sectional. See plot B2 in the appendix for a SEM path analysis depiction.
Mediation Results-Arguing With Partner.
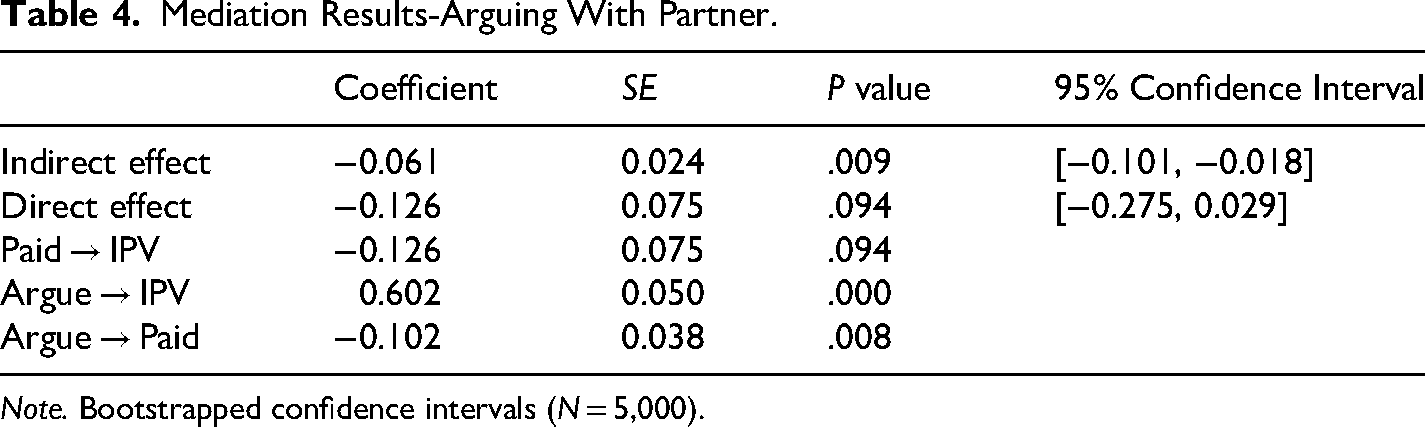
Note. Bootstrapped confidence intervals (N = 5,000).
Propensity Score IPW Results
A propensity score analysis with a latent variable model with inclusive factor scores (PSIF) was run. This model used the same set of variables as the regression models above (i.e., binary PFL predictor, binary IPV outcome, and a set of both manifest control variables and a latent control variable). For details, see the Methods section. Step 5 of the PSIF involves running a multiple-group analysis (i.e., “treatment” grouping by mothers who took PFL as one group and “untreated” grouping by mothers who took unpaid leave only or no leave) with inverse probability weighting combined with complex survey weights applied to the data, comparing estimated thresholds/means of IPV during and/or since pregnancy. A nested model comparison was used, in which IPV variable thresholds across the two groups were constrained to equality in one model and freely estimated in a second model. A significant “chi-square test for difference testing” value of 8.998, with 1 degree of freedom, and a P value of .0027 suggested that model fit was significantly better when IPV thresholds/means across groups (i.e., paid vs. unpaid/no leave) were allowed to be different, suggesting a significant difference between groups in terms of self-reported IPV, weighted by the IPW using all control variables. The mean IPV value for the paid leave group was 0.028 (2.8% reporting IPV victimization) versus the mean IPV value for the unpaid/no leave group, which was 0.040 (4.0% reporting IPV victimization), corresponding to a 30% difference. This converges closely with the SEM approach, which estimated a 33% lower predicted probability of IPV victimization among mothers who took paid leave. See Appendix B (Table B1 and Plot B1) for covariate balance information, which is presented as standardized mean differences. No standardized mean difference is larger than 0.25 SDs (Stuart & Rubin, 2008).
Discussion
IPV is a preventable public health problem (Niolon et al., 2017) that remains a significant issue. Decades of research document the deleterious effects of IPV (Breiding et al., 2008; Fogarty et al., 2023; Stubbs & Szoeke, 2022; Warshaw et al., 2009). When IPV occurs during the perinatal period, women can experience increased mental and physical health problems, which may lead to adverse birth outcomes (Currie et al., 2022; Hahn et al., 2018). While much progress has been made to develop treatment and response protocols for those who experience IPV, less work has identified ways to prevent IPV from occurring (i.e., primary prevention). In this article, we examined the association between PFL and IPV victimization for women who were employed during the perinatal period.
Based on the FSM, it was hypothesized that receipt of PFL would be associated with reduced IPV victimization for women employed during the perinatal period. To strengthen our methodology, we employed two approaches of estimating the ATE of the receipt of PFL on reductions in perinatal IPV: (a) SEM and (b) propensity score analyses with a latent variable model with PSIF. Without the ability to use an experimental design, these models instead controlled for several relevant covariate differences between those who took PFL versus those who took unpaid leave only or no workplace leave. Furthermore, these approaches make use of latent variables, representing SES, which adjust for measurement error within control variables, reduce the number of data dimensions (i.e., combining several covariates into one latent variable), and minimize omitted variable bias (Leite et al., 2019). Our results suggest converging lines of evidence with a 28.9% reduction in the odds of reporting IPV during the perinatal period for those who received PFL based on the SEM results and, similarly, a 30% reduction in IPV for PFL recipients based on the PSIF approach. Moreover, the association between PFL receipt and IPV victimization was strongly associated with a decrease in romantic partner arguments. Because of the potential for overlapping measurement occasion and therefore uncertain temporal ordering of effects, causal inference is very limited. However, the pattern of findings (e.g., PFL negatively associated with arguing, whereas arguing was positively associated with IPV) along with the strength of those associations holding with a strong set of covariates, suggests that measures of romantic partner conflict, such as argumentative behaviors, may be suitable candidates for mechanistic-focused research. Likewise, these findings are consistent with those of Gartland et al. (2011), who found a reduced odds of IPV victimization in the 12 months following birth for those women who received PFL. We found a nearly 30% reduction in the odds of IPV for women employed during the perinatal period who received paid leave. Additionally, our findings are consistent with the FSM, which posits that financial hardship can create stress and conflict in relationships. IPV may be reduced by eliminating economic pressure on families through PFL policies compensating them for time away from work. Providing concrete and economic support to families during highly stressful periods (e.g., perinatal period) may reduce some of the most severe forms of family violence, including IPV, at a critical period in the lives of developing children and their families.
Limitations
There are noteworthy limitations of this study. First, it is well understood that the research field lacks quality, robust, representative, and consistent IPV data across the country, making its study quite challenging. The PRAMS study is focused on collecting a large number of self-reported surveys from mothers each year, in each state. What PRAMS doesn’t lack in sample size it lacks in scope and depth, with respect to any particular outcome. PRAMS surveys are only required to include two IPV items, which focus on physical abuse. Only a handful of states add additional items. We are therefore not able to present IPV data, with much reliability, by type of abuse. Moreover, PRAMS data are almost entirely self-reported. Second, our study was non-experimental in design, which increases the potential for omitted variable bias. While several covariate adjustments were made ranging from race/ethnicity to socio-economic differences, which is well-established confounders in the IPV literature, the study design was, in part, limited by the measures collected by PRAMS. While our study did incorporate data from different years and study waves, it is important to point out that the PRAMS study does not involve repeated measurement at the individual level. New cohorts of participants provide data each year. We do, however, make use of retrospective data, which captures variation across the perinatal period. Third, only six states provided sufficient data on both family leave and perinatal IPV; therefore, these results may not be nationally representative. Lastly, our focus on perinatal IPV has both strengths and weaknesses. We know of no other data sources, other than PRAMS, that measure IPV consistently across time, across states, and across the perinatal time-period. Retrospective reports from multiple perinatal time points allow us to model outcomes across the entire perinatal period. We combine self-reported IPV from two different, retrospectively reported time points in the perinatal period, namely IPV during and/or since pregnancy. By casting a slightly wider net to capture more of the perinatal period, our results do not distinguish whether PFL may impact different points in the perinatal period more than others. For example, PFL may impact outcomes more strongly after childbirth than during pregnancy. Conversely, PFL may have unexpected and overlooked effects that occur prior to childbirth, such as anticipatory impacts on family stress and IPV prior to utilization of leave even begins. Mothers employed during the perinatal period may be less likely to quit their job and leave the workforce if they anticipate being able to take PFL. Knowing PFL is an option might increase feelings of economic security and reduce anxiety in the household, even before birth. Future research directions may focus on isolating specific, within perinatal period effects. Additionally, future research would benefit from repeated-measures data that can more accurately measure the potential mechanistic effect that reduced arguing may have on the relation between PFL receipt and IPV. The “arguing” measure was collected in the 12 months before a child was born, which may overlap or precede any anticipatory effects of PFL, making strict conclusions regarding mechanistic factors challenging.
Conclusion
IPV is a public health problem with long-term consequences associated with its occurrence. Concrete and economic support policies are promoted as a child maltreatment prevention solution; however, less research has examined their effects specifically on IPV. The current analysis found that one concrete and economic support policy, PFL, was associated with lower odds of IPV victimization during the perinatal period. This association was mediated by arguing among partners. These findings are promising and point to the power of public health strategies for the primary prevention of family violence.
Footnotes
Ethical Considerations
This study was deemed exempt by an independent review board (BRANY IRB).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the Centers for Disease Control and Prevention (R01CE003178) of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award totaling $977,677 with 100% funded by CDC/HHS. The contents are those of the authors and do not necessarily represent the official views of nor an endorsement by CDC/HHS or the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
We thank the PRAMS Working Group, which includes the PRAMS Team, Division of Reproductive Health, CDC and the following PRAMS sites for their role in conducting PRAMS surveillance and allowing the use of their data.
Author Biographies
Appendix A
For the PRAMS family leave responses and “IPV Since Pregnancy” final analyses dataset (n = 16,004), we used the following survey regions and questions:
Family leave respondents. Subset to mothers who responded to the question “Did you take leave from work after your new baby was born?”
Paid—yes, no; Unpaid—yes, no; no leave—yes, no; And four regional options (see Kortsmit et al., 2021):
New Jersey state option: Temporary Disability Insurance (considered paid leave) New Jersey state option: Family Leave Insurance (considered paid leave) Missouri option: Family Medical Leave (considered unpaid leave) New York City: Temporary Disability Insurance (considered paid leave)
IPV Since Pregnancy (final analysis dataset): Subset to data from states that had IPV “since pregnancy” data: N = 16,004 individual regions (6) and years (from PRAMS Phases 7 and 8) include:
Alaska (2012–2015) Louisiana (2016–2021) Maryland (2012–2020) Minnesota (2018–2021) New Mexico (2012–2015) Ohio (2012, 2014, 2015)
Appendix B
Table B1. Covariate Balance (Standardized Mean Difference).
Plot B1. Covariate Balance (love plot).
Plot B2. Mediation SEM Path Model.