
Abstract
The COVID-19 pandemic intensified domestic violence and abuse (DVA) and limited access to face-to-face support, creating urgent challenges for survivors and services. This study explored stakeholder priorities for remote DVA support using a modified Delphi approach with 35 UK participants, including expert survivors, service providers, and commissioners. Findings highlighted increased isolation, stigma, and mental health impacts, alongside varied experiences of remote provision. Stakeholders emphasized safety-by-design, accessibility, and survivor-led decision-making as essential features of remote support. The study recommends blended, trauma-informed models that integrate digital and personal-contact options to enhance responsiveness, safety, and equity in DVA service delivery.
Introduction
Domestic violence and abuse (DVA) is a global public health issue that was significantly exacerbated by the COVID-19 pandemic. Domestic abuse is defined in UK statutory guidance as “any incident or pattern of incidents of controlling, coercive, threatening, degrading and violent behaviour, including sexual violence, between those aged 16 or over who are, or have been, intimate partners or family members” (Home Office, 2022). This definition reflects current UK legislation and policy.
DVA is associated with substantial morbidity and mortality (Chandan et al., 2020; Home Office, 2022; WHO, 2021). Addressing such a challenge requires the adoption of a multi-system public health approach consisting of primary, secondary and tertiary prevention (Bradbury-Jones and Isham, 2020). The COVID-19 pandemic affected all aspects of social and economic life, generating new health needs and risks and exacerbating existing inequalities (Bradbury-Jones & Isham, 2020). Evidence quickly accumulated on the pandemic's impacts globally and in the UK—including increased domestic responsibilities and mental load for women, escalation of violence within the home, more complex needs, rising service demand, and barriers to access. For example, US-based reports highlight gendered burdens and DVA risks (Alon et al., 2020; Kaukinen, 2020), whereas UK-focused analyses document increased calls and access challenges within national systems (Mahase, 2020; Speed et al., 2020). Distinguishing between international and UK evidence clarifies which findings are generalizable and which directly inform UK service responses.
During the COVID-19 pandemic, particularly under lockdowns and social distancing restrictions in 2020 and 2021, many DVA survivors were unable to access face-to-face services and instead relied on remote options such as helplines, online groups, and digital counseling. Demand on domestic abuse helplines increased in the year ending March 2021 with a 22% increase in people supported by the National Domestic Abuse Helpline in England (Elkin, 2021). Support was provided by agencies through webinars and online support groups (Caridade et al., 2021). This helped those who had access to digital media and devices to obtain help and for many, had the benefit of interaction with the other survivors in support groups. However, there were challenges with the changes to modes of service provision (Desai et al., 2022). For example, issues were directly related to the technology itself. A Portuguese report identified that 29.9% of survivors experienced difficulties in accessing remote services and using digital technologies with 28.5% experiencing the disadvantage of lack of knowledge in using digital technologies (Caridade et al., 2021). Additionally, services experienced challenges with information technology (IT) and Internet access, and practitioners raised concerns about client privacy and confidentiality, working at home and isolation. Initially, services shifted from preventative, early intervention approaches to more crisis-driven, reactive responses, driven by victim's isolation with perpetrators (Desai et al., 2022).
Widespread adoption of remote service delivery by domestic and family violence services through this period was a major development, yet it proceeded with little research guidance. Importantly, prior to the pandemic, using video calls and chat apps to provide support, information and counselling were already not universally accepted by practitioners. For example, Bayles (2012) questioned whether video calls were acceptable for providing therapeutic support, given the loss of physical connection and difficulties observing and interpreting clients’ non-verbal and physical cues without physical proximity. Although restrictions have eased, remote service delivery remains highly relevant as it can improve accessibility for survivors facing geographic, mobility, or safety barriers. Recent studies highlight the expansion and normalization of digital support options beyond the pandemic, underscoring their potential to complement face-to-face provision in the long term (e.g., Anderson et al., 2021).
Byrne and Kirwan (2019) found that despite embracing multiple communication tools, social workers were aware about conducting relational work electronically. Social workers used text messaging primarily administratively, for setting up meetings or coordinating teams, but avoided remote counselling, talking about personal matters or exchanging confidential information via these means, given the potential for misinterpretation. They questioned whether technology should be considered an “add-on” to existing practice, or a fundamentally different practice model which alters how people interact and relate, effectively depleting service quality. According to Women's Aid (2021), in their Shadow Pandemic report, DVA services, other sectors, policy makers and practitioners need to learn from the experience of lockdowns and COVID-19 pandemic more broadly, to ensure they are better prepared for surges in DVA, including high risk and high harm reports. This includes exploring and understanding new elements of service provision that improve accessibility, and to ensure that they are sustainable and beneficial. It also involves assessing existing and emerging virtual provision and processes to identify what digital service support should be continued, enhanced, or removed. With all this in mind, there was a clear need to examine how remote DVA services can be most effectively designed and delivered. Hence, in this study, we aimed to explore with key stakeholders (practitioners, survivors, and policymakers), what the most important features are to a remote support service for survivors of DVA. Thus, this study was guided by the following research question: What features and formats are considered most important for remote support services for survivors of DVA by key stakeholders (survivors, service providers, and commissioners)?
Methods
Overview of Study Design
This study used a modified Delphi approach to achieve consensus among key stakeholders on priorities for remote DVA support services. The process involved three sequential rounds: (i) an online survey to gather initial ratings and feedback on existing remote services, (ii) focus groups to explore survey findings and identify features of an ideal remote support solution, and (iii) a workshop to refine priorities and develop consensus on service format, content, and evaluation strategies. Each round built on the previous one, combining quantitative ratings with qualitative insights to ensure a comprehensive understanding of stakeholder perspectives.
Design
We undertook a modified Delphi study with key stakeholders involved in DVA support service provision in the UK. A Delphi study seeks consensus among experts through structured rounds of data collection, typically combining quantitative and qualitative input (Van Teijlingen et al., 2006). Our modified or “reactive” Delphi approach presented participants with pre-defined areas for evaluation rather than an entirely open first round (Tonni & Oliver, 2013), guided by our research question on experiences of DVA and priorities for remote support solutions.
Rationale for Expert Groups
We included three stakeholder groups; survivors, service providers, and commissioners because each brings unique expertise: survivors offer lived experience of accessing support, providers contribute operational knowledge of service delivery, and commissioners inform policy and funding priorities.
Tasks and Questions
In Round 1, participants rated 12 existing remote DVA services on five dimensions (usefulness, suitability for remote delivery, accessibility, effectiveness, and value for money) using a five-point Likert scale and provided open-text comments. In Round 2, focus group participants reflected on survey findings and discussed features of an ideal remote support solution. In Round 3, workshop participants ranked priorities for service format, content, and evaluation using an online polling tool (Mentimeter) and contributed qualitative feedback.
We defined consensus pragmatically as convergence of rankings and themes across rounds, indicated by stability in top-ranked items and thematic saturation during qualitative analysis. This approach aligns with recommendations for modified Delphi studies where strict statistical thresholds are not always feasible (Tonni & Oliver, 2013).
Ethical Considerations
Ethical approval was granted by Oxford Brookes University Research Ethics Committee (UREC Ref No: 221563) and University of Birmingham Research Ethics Committee (ERN_21-0619). Participant wellbeing was prioritized at all stages of research in line with the British Psychological Society code of human research ethics (British Psychological Society, 2014). Participants were informed of the anonymity and confidentiality of their data.
Round 1: Survey—Participants and Procedure
For the first round, we carried out a survey. The survey was designed and distributed using Qualtrics. We recruited participants using the existing network of survivors, intervention providers and commissioners (developed in other parts of the study), and our survivor panel.
Participants and Sampling
We recruited 40 participants across three key stakeholder groups:
An additional five participants identified as “Other,” representing roles such as researchers or practitioners in related fields. Of the 40 participants, 85% identified as female and 3% as male (12% did not disclose gender). By group: expert survivors (n = 20, 50%), service providers (n = 11, 27.5%), commissioners (n = 4, 10%), other (n = 5, 12.5%). Ethnicity: 66% White British, 5% Bangladeshi, 3% Black, and 26% other backgrounds.
Round 1: Survey—Purpose and Procedure
The aim of Round 1 was to gather initial stakeholder perspectives on existing remote DVA services and identify priorities for improvement. Participants completed an online survey rating 12 services on five dimensions (see below). These findings informed the design of Round 2 discussions.
Participants rated each service on five dimensions using a five-point Likert scale (1 = strongly disagree, 5 = strongly agree). Instructions clarified that “useful” referred to perceived benefit for survivors, “effective” to achieving intended outcomes, “accessible” to ease of use and availability, “suitable” to appropriateness for remote delivery, and “value for money” to cost-effectiveness. Respondents were also asked to provide demographic details at the end and to leave their contact details if they would like to take part in subsequent rounds of the study.
Round 2: Focus Groups—Purpose and Procedure
The primary aim of the focus groups was to explore stakeholder perspectives on remote DVA services in greater depth, building on survey findings from Round 1. All focus groups followed a similar protocol: participants were presented with quotes from earlier interviews to stimulate discussion, then reviewed survey results and reflected on priorities for remote support solutions. While expert survivor groups naturally included more discussion of lived experiences, the core questions about service features, accessibility, and ideal formats were consistent across all stakeholder groups. This ensured comparability of data while allowing each group to contribute its unique perspective. Data from all focus groups were analyzed together using thematic analysis, with attention to differences and commonalities across stakeholder types. Insights from these discussions shaped the priorities taken forward to Round 3.
Round 2: Focus Groups—Participants and Procedure
The focus group interviews were conducted online via Zoom to facilitate recruitment and participant safety. In total, 24 expert survivors and 6 service providers/commissioners took part. Five expert survivors chose not to provide demographic information. Of the remaining 19 their ages ranged from 26 to 52; 16 identified as white, 2 as Bangladeshi, and 1 as Black.
Each focus group began with a short presentation of quotes drawn from interviews conducted in an earlier stage of the project. These quotes illustrated expert survivors’ experiences of remote support during the pandemic and were used to “set the scene” by grounding the discussion in real-world perspectives. The facilitator invited participants to reflect on these quotes before reviewing survey findings, which helped to stimulate conversation and ensure that subsequent discussions were informed by authentic survivor voices (see Appendix 1).
They were then provided with a summary of the survey findings relating to the usefulness and remote suitability of the services in round 1 and asked to reflect on their views about what would make an ideal remote support solution. Each participant was asked to reflect in turn after each presentation and then all participants were invited to share further views or respond to other members of the group. Finally, each participant was invited to share any final thoughts.
Round 3: Workshops—Participants and Procedure
In the final part of the Delphi process, we conducted one workshop to critically discuss the findings of the previous rounds. In total, seven people took part; five expert survivors, one service provider and one service commissioner. All seven had taken part in round one and round two.
The aim of the workshop was to develop a consensus about the most appropriate format and content for an ideal remote support service. Building on the findings from previous rounds we also sought to identify priorities for training needs relating to external services, and to seek the participants’ views on how best to evaluate remote support services. The workshop took place on Zoom and lasted 90 minutes. Participants were asked to use Mentimeter—an online polling tool—to rank priorities for the most appropriate service format, the most important information, the highest priority for training needs and their preferred features. Participants could view the overall ranking from the group but could not see what each individual had entered. Following each ranking exercise, participants were invited to discuss their ranking and respond to each other's comments. Finally, they were asked to discuss their views about how services should be evaluated, and they could enter this information into a word cloud.
Findings
Round 1
Services rated highly for usefulness typically offered multicomponent, survivor-centered support (e.g., counseling, parenting advice, trauma recovery). “Effective” referred to perceived ability to improve safety, wellbeing, and empowerment. The highest ranked service for usefulness was aimed at children and young people aged 4 to 18 years who had experienced DVA. Their usual provision included counselling, play and music therapy, advice and information on coping strategies and signposting to other help sources. These services were delivered remotely in lockdown. The top ranked service for remote suitability provided a range of programs that were delivered remotely during the pandemic. The programs supported women to learn about the realities of domestic abuse in relationships, gain control over their lives, empower them as mothers, and recover from trauma. The highest ranked service for accessibility was specific to supporting Deaf people who were experiencing DVA and supported them remotely to access services such as immigration, police, housing, and social services. Another feature was the allocation of a qualified Deaf Independent Domestic Violence Advisor. The highest ranked service for effectiveness specifically focused on supporting LGTBQ+ people and provided emotional support, brief advice, signposting as well as housing support. They had an educational program to help people develop coping strategies and build their confidence and a 12-week resilience program. Alongside this they provided complementary therapies, acupuncture, mindfulness, and art/poetry. In lockdown, these services were delivered on the phone or via the web.
Round 2
We analyzed the qualitative data using an inductive thematic approach, following Braun and Clarke's six-step process for identifying, analyzing, and reporting patterns in the data (Braun & Clarke, 2006, 2019). This means themes were developed from the data rather than imposed from a pre-existing framework. The final themes were: Impact of DVA (pandemic-related challenges and mental health), Help-seeking challenges (barriers to accessing support), Experiences of services (positive and negative aspects of remote provision).
Overview of Findings
The focus groups were conducted to explore priorities for remote DVA services, building on survey results from Round 1. While the primary aim was to assess remote service provision, participants, particularly expert survivors, often discussed the broader impacts of DVA during the pandemic as context for their views on service needs. These reflections informed their recommendations for remote support features and accessibility. Data from all stakeholder groups were analyzed together using inductive thematic analysis, with attention to differences and commonalities across expert survivors, service providers, and commissioners.
Impact of DVA
The impacts of DVA are always distressing and wide reaching, as all our participants recounted in this study. However, it was very clear that the pandemic had a great number of additional negative consequences for DVA survivors and services. The experience of DVA meant missing social interaction and communications and led to feelings of isolation and loneliness. “…it was in the middle of COVID. I just become a first-time mom to a new bairn. I think she was two. She was two months old when I suddenly like it all kicked off and I had to leave. So, I was fully isolated because it was in the middle of COVID, and there was no community as such…it's the most isolating thing on your own, like, say, in COVID or in a pandemic where you've literally got no one” (Expert Survivor focus group 2)
Many reported that perpetrators were able to take advantage of being in a more powerful position due to the lockdown conditions. Furthermore, survivors frequently mentioned experiencing stigma and shame, which was exacerbated by lockdown conditions. Most of the survivors talked about the impact of experiencing DVA on their mental health and the mental health of their children. “…if you're in a coercive, controlling relationship, you can't so think for yourself so. And I think that is so common, and they just keep saying you’re slipping up. You're doing this wrong. You're doing that instead of this… everything is negative against you constantly, and you don't see any positives. And I think that's why so many children end up in care, and that I think that in the long run, then the children will end up with mental health issues as well as the parents having mental health issues” (Expert Survivor focus group 3)
Service providers and commissioners reflected on their awareness at the start of the pandemic that the situation was going to be incredibly challenging. They recognized that violence would escalate, and it would be important to try new ways of working in order to reach vulnerable people. So, I think anyone who works in domestic abuse, or has any experience of domestic abuse, understood really quickly how devastating the lockdown was going to be” (Service Provider, Focus Group)
Help-Seeking Challenges
Survivors often reported that they were not always able to recognize that what they were experiencing was abuse straight away, and had only come to realize this much later. For this reason, many participants discussed the need for information about DVA to be widely available so that help could be sought earlier. “We do need to know how to access the support when before things hit the fire, because most of us doesn’t actually realise in that situation that it is abuse. So it's getting the information at the right time…so it does need to be in GP services. It needs to be in supermarkets. Because these places that we normally go to (Expert Survivor, focus group 1)
Some focus group participants felt that gender stereotyping and the stigma related to DVA was made worse during the pandemic and affected their ability to seek help. Experiences of stigma and shame were linked with a lack of awareness of DVA that affected survivors’ ability to seek help But then there's also one side where you think you can be a bit in denial, because when you're dealing with narcissistic behaviour, you tend to think ‘it's you, you’re not a victim’, so it's quite hard to then seek help, you think it's not happening to you” (Expert Survivor. focus group 3)
Other significant challenges were felt in relation to seeking financial and legal help. For example, many survivors felt unprepared for the battles they had to face when identifying the benefits they were entitled to and reported that perpetrators could be very devious about financial matters and used their charms to ensure they did not have to support the family. They [perpetrators] can be very good at hiding finances…(Survivor focus group 2)
Legal professionals were repeatedly discussed in focus groups; some had paid large sums for legal advice and felt that this should be free. Once in the legal system, survivors felt that legal professionals did not have enough information on DVA and that family courts were not sufficiently aware of and minimized DVA. Additionally, social services, housing services and the police were frequently mentioned by participants as having training needs in order that they were able support survivors of DVA more effectively. Service providers faced numerous challenges, including those related to having adequate resources available. We’re all desperately trying to make the most of the resources that we’ve got, and I’ve seen that happening from the frontline, as well (Service Provider, Focus Group)
Furthermore, the shift to home working and school closures during lockdown put pressure on the overstretched workforce. They’re trying to juggle looking after children—professionals are committed to delivering the services, but the IT and the skill-set around working from home needs to be very quickly much better than it is (Service Provider, Focus Group)
Experiences of Services
Survivors reported a range of experiences with services they had encountered. Those services that engendered a sense of community were perceived as being the most helpful. These services tended to be survivor led, which meant they felt that the person they were speaking to had direct experience of understanding what they were going through and could empathize. [Name of service] literally saved my life and my children's lives. So regardless of the other places that have sometimes let us down. I think if we look at [the service] as an organization on the kinds of things that they have done, and the things that we have found helpful, that sense of belonging of community of just allowing us to be who we are without having to put on a brave face. I think I think we've been just really really lucky (Expert Survivor, focus group5)
However, there were many reports of negative experiences with various services. Many felt that services did not work well with other services and that they were often signposted to services that did not help or signposted them to yet more services. Often survivors spoke about feeling not feeling heard or being misunderstood. “I did seek help at [service]. I really regretted with my going there. I had finally worked up the nerve to seek help. I’d finally agreed to speak with someone. When I got there, I was nervous and scared, and I was greeted by a cold receptionist. I was made to fill out paperwork. Then, when I met with one of the women that worked there, she asked me about my situation. I’d begin to explain, and she would interrupt. Then she asked me what exactly I wanted or needed from them. I asked about counselling, and she said they couldn’t help me there, I’d have to go elsewhere” (Expert Survivor focus group 1)
In all focus groups, survivors talked about experiencing difficulties with accessing useful support to help them with matters relating post separation abuse when there were children involved. This included a number who had lost contact with children who were in custody of the perpetrator despite having had shared custody granted to them. Nobody helps you with parental alienation. Nobody seems to know anything about it and organizations that do say oh, you know, send fifty pounds to this book. I don't need another book on it. I'm an expert on it, but nobody's helping (Expert Survivor focus group 5)
Further to this, the length of time to receive support was frequently discussed as a major issue when trying to access support and leaves an abusive relationship. It was almost too late, and I was almost back in the relationship because it took so long to get anywhere (Expert Survivor focus group 2)
Service providers felt that there were some aspects of the shift to remote services during the pandemic that had gone well, for example, being able to use video chats. “During the pandemic, we'd never worked remotely before, and the first that we did was to find out how we could do that. So, we used Zoom as a platform and Teams. And we also did a lot of phone calls…and to just be able to provide a crisis calls service so that we could pick up the phone when somebody reached out (Service Provider, Focus Group)
However, service providers and survivors also cautioned that the use of remote tools should not be used a replacement for face-to-face services. For example, some discussed the difficulty of knowing if someone was safe online, or if a perpetrator would know what they were doing. There could be internet connectivity issues, and this meant that it was difficult to know if someone had lost access to a session or there had been a safety incident. In addition, people noted that the sheer wealth of online information could be overwhelming. There's no single point of access. So like I say someone types in domestic abuse on the Internet, and lots of different stuff comes up one of the probably the top. One may well be women's aid or something like that. But it depends on where someone is in the country (Service Provider, Focus Group)
In addition to identifying themes within the focus group transcripts, we also constructed a list of suggestions that were discussed in the focus groups for what an ‘ideal’ remote support solution would look like. This information was broken into categories relating to the format of remote support; information needs; external agencies/groups who would benefit from further training; and specific content for a remote support tool. This information was taken forward to the workshop in round three.
Round 3
Service Format
Service formats were ranked in the following order: website, telephone chat, text service, smart phone app, social media, public advertisements, video chat (Figure 1).
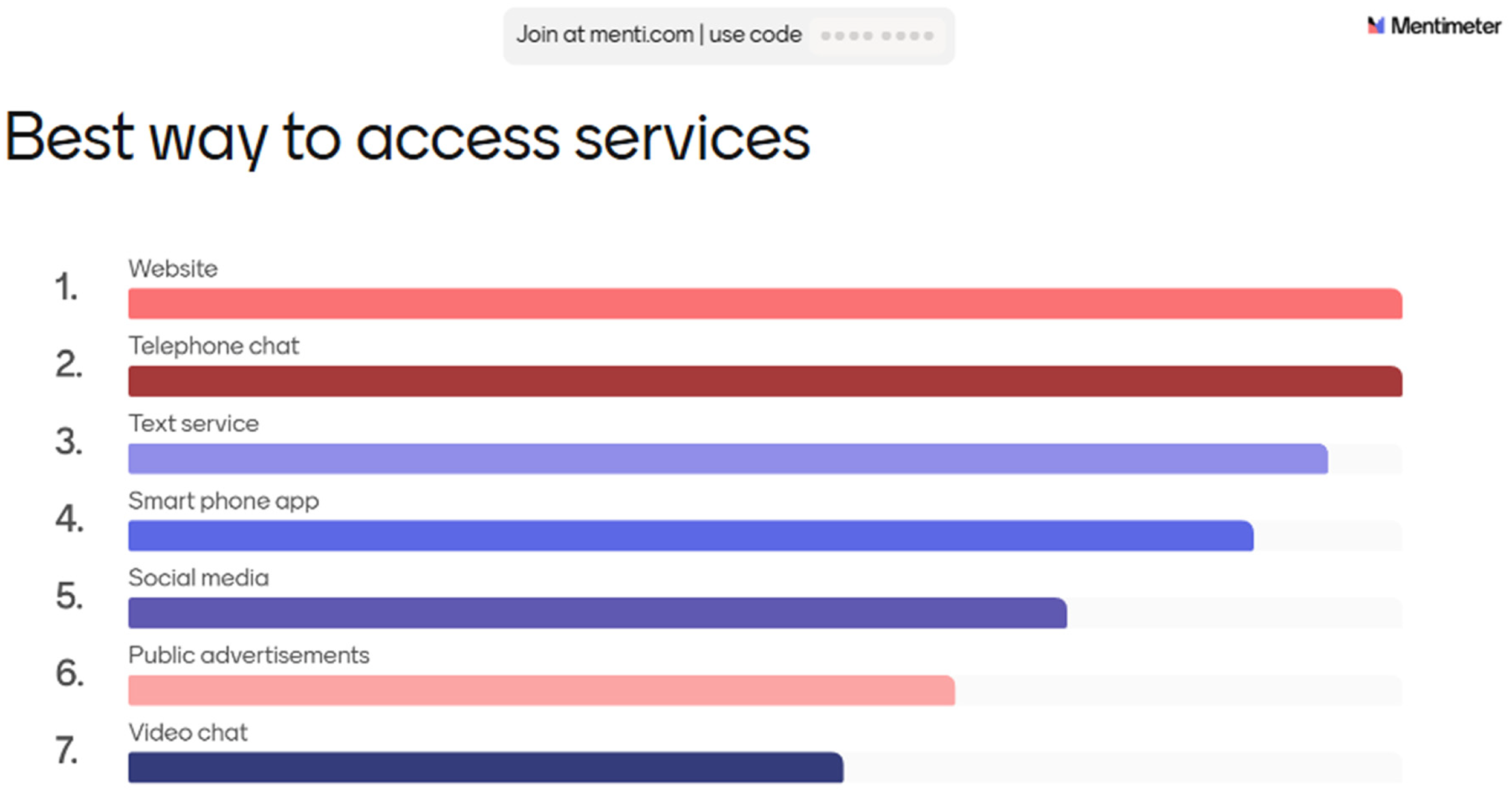
Workshop ranking of preferred access routes to services (bars represent number of votes; larger bars indicate higher ranking).
Discussions revealed that some participants were concerned about a lack of access to the internet or smartphones and the ability to chat with someone was a priority. I suppose most people have some sort of form of telephone. So that is the reason why I would probably go for a telephone service first of all, because it's accessible to the majority of people (Service provider/commissioner) So long as it's safe to call (Expert Survivor)
However, social media was recognized as potentially useful. I know we've talked about people's access to the Internet etc. Putting that aside. I know when I was smack bang in the middle of the pandemic. One evening I just everything was getting a bit too much, and there was an option on social media from my local children's centre and we set up a conversation for that evening and that was really useful, really useful. So it's nice to see that on there (Expert Survivor)
A further suggestion not included in the ranking exercise was to include information about DVA support within leaflets or letters that contained other information, such as within household bills, or fire safety information. However, participants wanted to underscore the importance of having personal contact, even if that could be tricky with the need for childcare. And I do understand it's come out of the COVID pandemic, but I think there should always be the opportunity for people to have the opportunities to have face to face (Service provider/commissioner) The option to see somebody face to face should be there, most of the time, especially before separation, as it will be really difficult to speak to somebody on the phone whole the other person is in the house and significantly increase their risk of further abuse. I think it is vital to have that option and also safety is paramount, as still three women are being killed a week by their current or former partner and I think we need to take it really seriously (Expert survivor).
Information
Information to access remotely was ranked in the following order: mental health support, legal advice, parenting support, financial advice, support with children, local support groups, emergency services, social services (Figure 2).
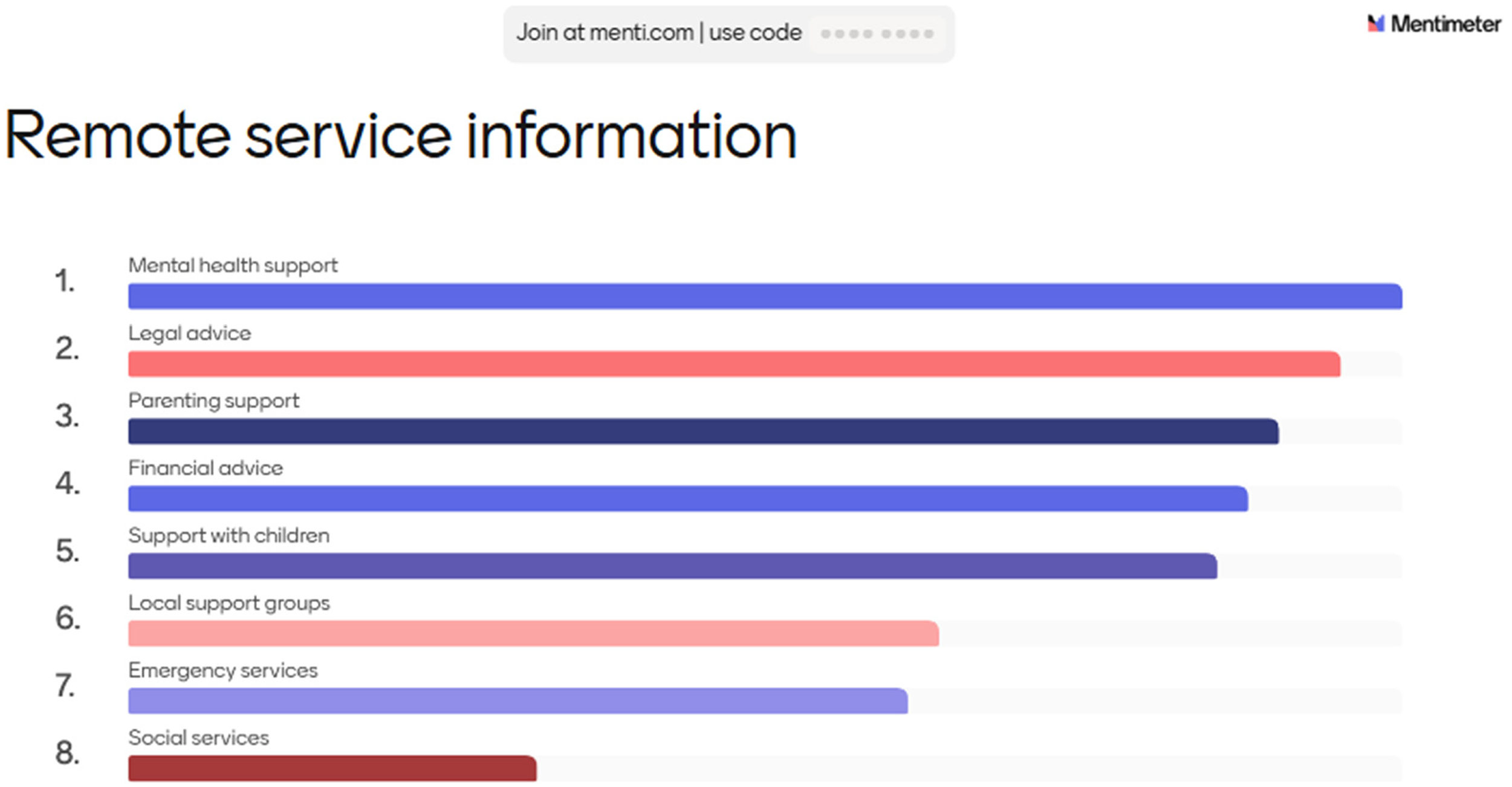
Workshop ranking of information needs for remote access (bars represent number of votes; larger bars indicate higher ranking).
Discussions began by highlighting the importance of accessing mental health support I found mental health support the most important thing to access, because without my head being able to function properly, I couldn't do anything else (Expert survivor)
An explanation for social and emergency services being rated at the bottom was that some survivors had poor experiences with social services in the past. A further suggestion that was not included in the ranking exercise was that people may need information on target hardening (providing additional security at a survivor's home) or sanctuary services.
Training
The discussion about information needs led onto a discussion about which services had the least amount of knowledge or experience with DVA in the participants’ views. Training needs for external agencies/groups were ranked in the following order: police, legal profession, teachers/schools, social services, GP/health professionals, children, general public, and employers (Figure 3).
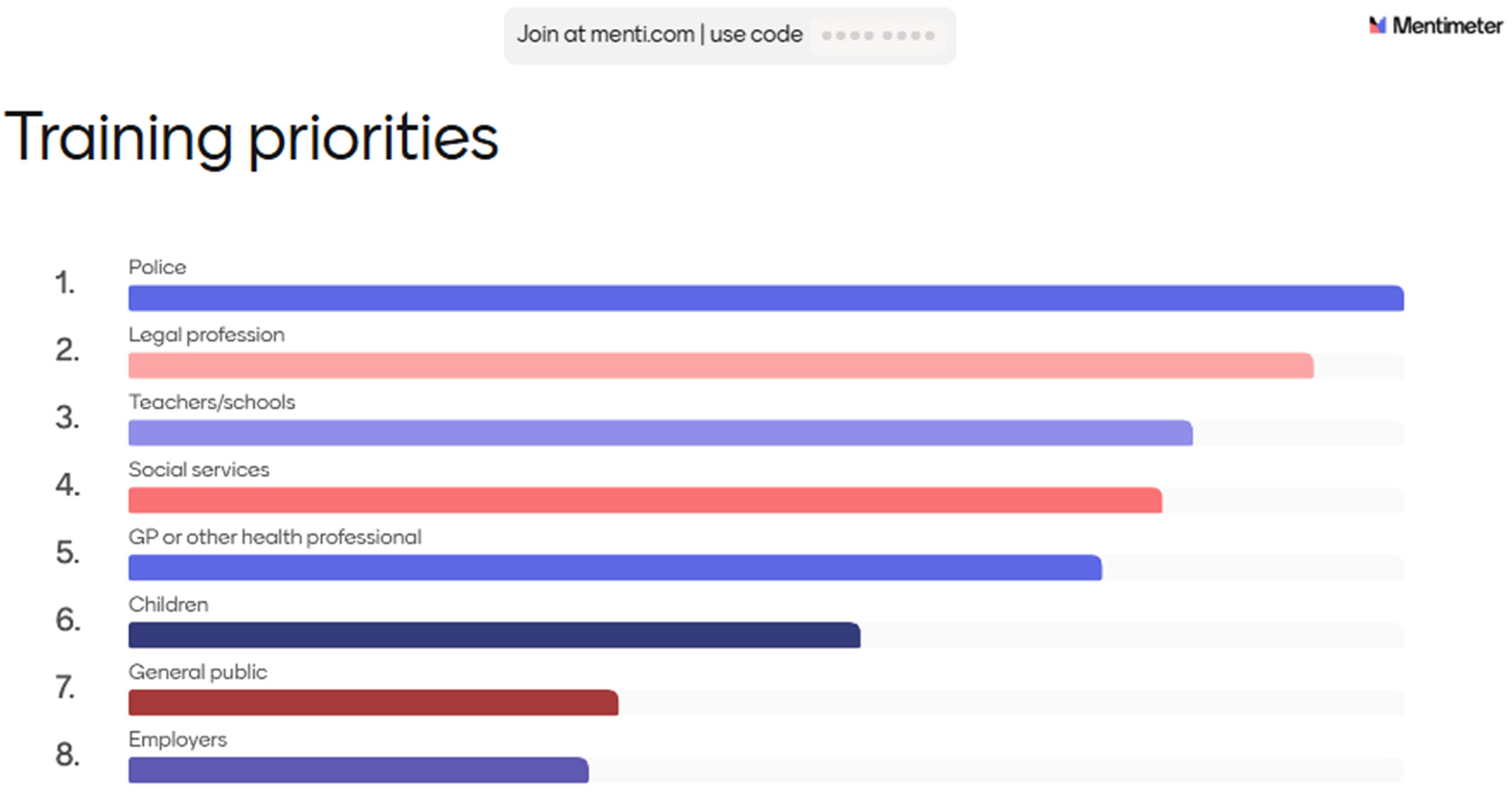
Workshop ranking of training priorities for external agencies (bars represent number of votes; larger bars indicate higher ranking).
Discussions revealed some negative experiences with the police when they were called to a DVA incident and had been perceived to side with the perpetrator or had too stringently followed the letter of the law, leaving the survivor in a difficult situation. We have had a consultation with community police, which is a really good way of building up and relationship between police and survivors, and they come in and they listen to survivor feedback, which is really good. We have some female police come in, and there was three of them, and they were really really shocked at some of the things that their colleagues had been actioning or actioning in such as like breaches of restraining orders and things like that, and not actually not arresting the person (Service provider/commissioner)
Previous experiences with the legal profession left survivors feeling let down and unheard, particularly in the case of emotional and psychological abuse. They do not understand coercive control. They do not understand trauma, so they're not trauma-informed organizations, and it just makes the situation so much worse. Again (Expert Survivor)
Content
The list of possible content for remote support solutions was ranked in the following order: 24/7 access to chat, journaling, chat with survivors, training courses, chat with professionals, videos to identify abuse, activities for stress, messaging functions (Figure 4).

Workshop ranking of remote support content features (bars represent number of votes; larger bars indicate higher ranking).
Discussion revealed a range of experiences that had been helpful for the survivors. So for me meditation was really helpful, because when I start to meditate I became less depressed, and not only did it calm myself down it also helped me to understand what was going on inside my head. As a result I became less depressed. I could also see what was happening around me without judging, like you know having a kind of degree of detachment (Expert survivor)
However, while most activities received some positive comments, the most highly endorsed feature was talking to other survivors. I think the chatting with the survivors is humongous. You’ve got a risk of, kind of overload, with somebody else's situation, but at the same time you can talk quite freely with someone who gets what you’re saying (Expert Survivor) Yes I agree, it's a balance as you can scare yourself listening to other peoples bad experiences but at the same time it can be very validating (Expert Survivor)
Discussions also centered on the need for more education in schools for children to understand what constitutes abuse, and for open conversations about healthy relationships to be more widespread.
Evaluation
Finally, we asked the participants to discuss how they would evaluate the success of a remote support solution. They strongly endorsed asking for feedback from the service users as the main priority (Figure 5). The word cloud visualizes priorities for evaluation, with larger words indicating higher frequency of endorsement. When participants endorsed “feedback from service users,” they suggested anonymous surveys and integrated feedback tools within digital platforms to inform service improvement.
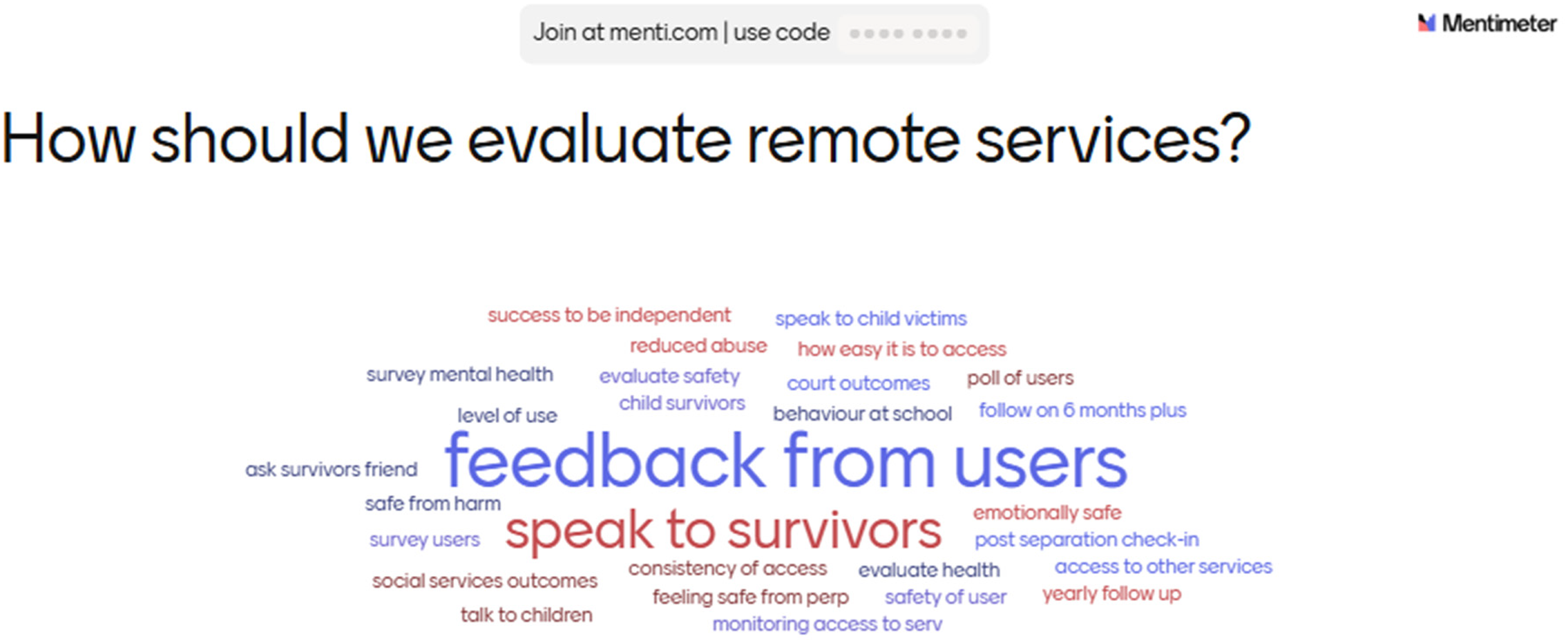
Evaluation priorities word cloud from workshop (larger words indicate more frequent endorsement).
Other suggestions focused on specific measures including feelings of emotional safety and mental health. Discussion centered on whether access to digital tools could be anonymously monitored to see how many people had engaged. I think it's really important to speak to the people who are accessing the service, because if you speak to the professionals, the police and things like that, a lot of their data sometimes is skewed, and it's skewed, because we're relying on them to report things accurately which I know they don't from my personal experience (Expert survivor).
Discussion
This modified Delphi study synthesized ratings and qualitative insights across survivors, service providers, and commissioners to identify priorities for remote DVA support. We found strong, convergent support for blended, survivor-centered services that combine accessible digital entry points with opportunities for personal contact, alongside explicit attention to safety in technology use. Several standout services excelled in specific areas. For example, services accommodating children and young people, offering women's empowerment programs, superior accessibility, especially for Deaf individuals experiencing DVA and LGTBQ+ individuals. Services supporting children and promoting empowerment were rated effective because they combined practical help (e.g., parenting support) with emotional recovery and confidence-building. These findings suggest practitioners should integrate trauma-informed approaches and flexible formats.
We then were able to delve in further to understand the pandemic's impact on DVA survivors, accentuating increased isolation, loneliness, and the heightened vulnerability of survivors. Challenges in recognizing abuse, overcoming stigma, and accessing legal and financial support were identified. Survivors reported varied experiences with support services during this time. Survivor-led services provided a sense of community and understanding, while others left survivors feeling unheard. The study acknowledges the shift to remote support services, but participants emphasized the importance of maintaining personal contact and face-to-face options, especially pre-separation. In discussions, participants detailed the ideal format for remote support, information needs, training requirements, and service evaluation. A recurring theme was the need for personal contact, particularly pre-separation. This study underscores the complexity of DVA survivor support during the pandemic and the necessity for improved service access. Understanding survivor experiences and feedback is critical in shaping effective remote support solutions for the modern challenges faced by DVA survivors.
These findings align with current literature, which also recognized the impact of the pandemic on DVA. In their reflections of working with DVA survivors during the COVID-19 pandemic lockdown, Proudman and Lloyd (2023) conclude that there was a “devastating impact” on vulnerable women particularly in relation to their access to justice. Findings from our study concur with this viewpoint. DVA survivors reported increased isolation, loneliness, which heightened their vulnerability. Challenges in recognizing abuse, overcoming stigma, and accessing legal and financial support were also identified. Proudman and Lloyd (2023) go on to say that the UK government and support agencies of failure to provide enough support to prevent significant harm to DVA service users during COVID-19 lockdown. In our study survivors reported varied experiences with support services during this time. For some there were difficulties in accessing remote services, privacy issues at home and several saying that it was difficult to maintain relationships remotely. Similar negative effects were reported in a recent focus group study of 57 female survivors of DVA and their children (Foster et al., 2022). However, we also found that female survivors reported positive outcomes as well. Remote support did maintain relationships with services in the absence of face-to-face contact. This finding was similar to that reported by Foster et al. (2022) and Tarzia et al. (2018).
The importance of tailored support services and the need for innovative approaches were evident in our study. Some DVA services were more successful in overcoming the challenge of needing to develop remote communication with service users at short notice because of COVID-19 lockdown. When these could be developed to meet the specific needs of users the more useful and effective they were reported to be. The most successful services demonstrated that it was possible to deliver complex interventions in a safe and secure way. Many reported that they will continue to deliver remote options even with the reinstatement of face-to-face services.
The study found that digital (interactive websites, texting services and telephone chat) service formats were most popular with service users. Telephone assistance is a very used service that has been delivered in several countries for a relatively long period (Reese et al., 2006). The literature also shows that it is feasible to use different forms of remote support (e.g., telephone, email and chat), to provide help (Haberstroh et al., 2008), as well as mixing online and face-to-face approaches (Wentzel et al., 2016).
Study participants thought that remote services could be developed further to enable access to other service users at all times and specialist practitioners at specific time. The main concern about this expressed by stakeholders related to the safety of DVA survivors either because offenders can remotely monitor their devices, such as computers, phones and home security systems or because of perpetrators locating individuals putting their physical safety at risk. Refuge (2022) reports an increasing problem of coercive control of women through social media. The existence of the potential risks and obstacles associated with the use of remote solutions, should not, however, lead to avoiding and disregarding the potential of digital solutions in supporting survivors of DVA (Finn & Atkinson, 2009). Strategies have been pointed out to promote the safety of victims when using digital platforms, for instance: using applications that increase the protection of the victims, such as password protected sites, “quick exit” buttons on sites, particularly relevant when the victim still lives with the abuser (Sorenson et al., 2014) or promoting e-literacy skills to minimize the risk (e.g., teaching about online privacy settings, providing information about password protection, locking and filtering the software used in online contact) (Rempel et al., 2018).
Service users thought that they had accumulated a wealth of lived experience and expertise that it would be useful to record and that remote services offered an opportunity do this. Providing information via remote services was felt to be particularly important particularly in relation to mental health support, legal advice and parenting support. Often, survivors of DVA find themselves in a situation of great isolation, due to the victimization process instigated by their partners and with reduced access to social support resources (Capaldi et al., 2012), so digital solutions are an important resource for obtaining information or even sharing experiences of violence and seeking help (Anderson et al., 2021). Also, Constantino et al. (2014) reported that online environments can reduce social risk and inhibition and promote the sharing of unwanted thoughts and feelings by victims.
Implications
The study contributes to the ongoing discourse on effective strategies to address DVA and highlights the critical role of remote support services in the evolving landscape of public health. It underscores the complexity of the DVA survivor experience during the pandemic and emphasizes the need for accessible, adaptable, and survivor-focused solutions to meet the growing challenges of this public health crisis. Future efforts should aim to build on these findings, incorporating survivor feedback and experiences to further refine and enhance remote support services for DVA survivors in a changing world. These findings are important because they highlight actionable priorities for service design, such as maintaining personal contact options alongside digital formats and addressing safety concerns related to technology monitoring. For practitioners, this means integrating flexible, multi-channel approaches and ensuring training for external agencies.
Limitations
Firstly, it is noteworthy that the sample for this study was drawn entirely from the United Kingdom. While this was consistent with the study's specific objectives, it does imply that the findings may not be universally applicable to other geographic regions with potentially distinct contextual factors. The issue of selection bias merits further consideration as it pertains to participant demographics. The study primarily engaged with survivors, practitioners, and policymakers deeply embedded in the field of DVA support services. This inherent focus may have inadvertently excluded the perspectives and experiences of individuals who, for various reasons, did not avail themselves of such services during the pandemic. Survivor participants may have had a degree of digital literacy, given their engagement with remote support services. Digital literacy may act as a further barrier should services move more of their support online. Consequently, the challenges faced by survivors lacking digital access may be underrepresented in the findings. Furthermore, while the study engaged service providers to some extent, the perspectives and challenges faced by this group were not exhaustively elucidated. A more thorough exploration of the service providers’ experiences and perspectives could potentially yield further valuable insights into the dynamics of service provision during the pandemic. We acknowledge potential bias introduced by presenting quotes before discussion in Round 2, the relatively small number of workshop participants, and the implications of combining survivors and practitioners in the same discussion space. Lastly, the nature of the pandemic was characterized by rapid evolution and development, challenges may have emerged that were not captured in this study. Therefore, the study's findings must be interpreted within the specific timeframe and context in which the research was conducted.
Conclusion
This study illuminates the complexities of remote support services for DVA survivors amidst the backdrop of the COVID-19 pandemic. It underscores the value of these services, particularly when survivor-led and fostering a sense of community. The study calls for a comprehensive, survivor-centric approach that combines remote and face-to-face services, inclusive design, and broad-based training initiatives. These findings provide a vital foundation for addressing the multifaceted challenges of DVA and guiding future research in this evolving landscape.
Footnotes
Ethical Approval
Ethical approval was granted by Oxford Brookes University Research Ethics Committee (UREC Ref No: 221563) and University of Birmingham Research Ethics Committee (ERN_21-0619). Participant wellbeing was prioritized at all stages of research in line with the British Psychological Society code of human research ethics (British Psychological Society, 2014). Participants were informed of the anonymity and confidentiality of their data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institute for Health and Care Research (NIHR) Policy Research Programme (project reference NIHR202707). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Biographies
Appendix 1
Quotes presented at the start of focus group discussions:
The biggest problem was trying to speak to someone who was knowledgeable enough to point you in the right direction. I think everyone's just signposting you all over the place, and you end up ringing around with no help and having wasted a lot of time. And time is something you don’t often have.
It takes women maybe seven times to leave a relationship, it took me three, but you need to get people at the point that they’re asking for help, like and it has to be near instant and I know that's impossible but you don’t get many opportunities, so when someone is reaching out for help, it really needs to be timely, because you’ve got them at that point where they’re open and receptive and most people turn around and that openness, that receptiveness disappears pretty quickly.
There should be a one stop shop like citizens advice bureau for people to access multiple services, being a victim of DVA I am anyways tired of repeating myself and then having to deal with court cases, sorting out benefits, childcare, solicitors, counselling makes it more difficult.
The entry point should be a less bumpy and seamless, because at that point you are at your lowest and you don’t want hurdles and don’t want to go around looking for help.