
Abstract
Obstetric violence is linked to postpartum depression, yet the mechanisms underlying this relationship remain underexplored. This study examined perceived partner support as a mediating mechanism among 535 women who had given birth within the past 18 months. Results indicated that obstetric violence was associated with higher postpartum depression and lower perceived partner support. Perceived partner support was negatively related to depression. Mediation analyses showed that perceived partner support partially mediated the association between obstetric abuse and violence and postpartum depression and fully mediated the link between perceived obstetric violence and postpartum depression. These findings suggest that obstetric violence may contribute to depressive symptoms partly by undermining women's perceptions of partner support.
The concept of obstetric violence was formally introduced in 2007 when the Venezuelan government recognized it as one of the 19 legally defined forms of violence against women (D’Gregorio, 2010). In the contemporary literature, obstetric violence is broadly defined as the inhumane treatment or neglect of women by healthcare professionals during reproductive processes such as pregnancy and childbirth (Bohren et al., 2015; Ferrão et al., 2022). This includes, but is not limited to, physical or psychological abuse, violations of privacy, violations of personal autonomy, the unnecessary pathologization or overmedicalization of childbirth, and disrespectful or coercive care practices.
Such violence can manifest in various ways, ranging from overt physical mistreatment, such as slapping, to more subtle yet harmful actions like denying pain relief when clinically needed or behaving harshly during routine procedures. Psychological abuse in obstetric violence often manifests through behaviors such as mocking the woman's appearance, using accusatory or threatening language, or shouting at her during the childbirth process (Hakimi et al., 2025; WHO, 2014). Informed consent violations, such as performing medical interventions without prior explanation or approval, are also common, as are breaches of privacy (e.g., failing to draw a curtain during examinations or allowing multiple unfamiliar providers to conduct assessments; Ravaldi et al., 2018; Sando et al., 2017). Structural and institutional barriers, including resource shortages and systemic inefficiencies, can further exacerbate the experience of coercive or neglectful care (Bohren et al., 2015; Tach et al., 2020).
While physical forms of obstetric violence can have immediate consequences for women's physical health, there is growing evidence that such experiences also contribute to emotional, behavioral, and cognitive difficulties. Women who are exposed to obstetric violence may be at an increased risk for psychological distress, including symptoms of postpartum depression, anxiety, and trauma-related responses (Kohan et al., 2025; Silva-Fernandez et al., 2023). Therefore, understanding the link between obstetric violence and postpartum depression has become the focus of the current research.
Obstetric Violence and Postpartum Depression
Postpartum depression is associated with a range of symptoms, including anhedonia, disturbances in sleep or appetite, persistent anxiety, difficulty concentrating, intrusive or distressing thoughts, feelings of guilt or worthlessness, agitation, uncontrollable crying, concerns about parenting ability, fear of being alone with the baby, emotional detachment, and thoughts of self-harm or harming the baby (APA, 2013). These symptoms often emerge in the context of significant psychological, emotional, and social changes that women undergo in the postpartum period. These changes stem from both the physical transformations following childbirth and the new responsibilities that come with caring for an infant (Yavuz & Bilge, 2022). Pitt (1973) defined early emotional disturbances in the postpartum period as “maternity blues,” typically occurring within 3 to 10 days after birth. When such mood disturbances extend beyond the initial 2 weeks, they may signal an increased risk for postpartum depression (O'Hara & Wisner, 2014; Zanardo et al., 2020).
There is no strict consensus in the literature on the time frame that defines postpartum depression. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; APA, 2013), postpartum depression can emerge within the first 4 weeks following childbirth and must persist for at least 2 weeks. However, the duration of symptoms may vary. Some researchers limit their samples to women within 6 months postpartum (Miller, 2002; Pearlstein et al., 2009), while others emphasize that depressive symptoms may persist or even emerge for the first time up to 12–18 months postpartum (Goodman, 2004; Horowitz & Goodman, 2004; Lumley, 2005). In line with this broader temporal perspective, Monti and colleagues (2008) highlighted the potential psychological vulnerability of mothers during the 9- to 18-month period, referencing Brazelton and Greenspan's (2000) concept of “touchpoints”—developmental phases in which children may exhibit regression, thereby disrupting established family dynamics and routines. Such disruptions may contribute to increased maternal stress and psychological difficulties. As a result, a number of studies have extended the assessment window for postpartum depression to include mothers of infants up to 18 months of age (Durukan et al., 2011; Monti et al., 2008). This extended time frame was also adopted in the current study.
In addition to biological and hormonal changes, several psychosocial risk factors for postpartum depression have been identified, including unplanned pregnancy, a history of depression or anxiety, and limited social support (Henshaw, 2003; O'Hara & McCabe, 2013). Given the wide range of psychosocial influences on postpartum depression, one increasingly recognized yet still underrepresented factor in the psychological literature is obstetric violence. As previously described, this term refers to the mistreatment of women by healthcare professionals during childbirth and may include physical abuse, verbal humiliation, neglect, or denial of informed consent (Bohren et al., 2015). Recent research has begun to examine the mental health consequences of such mistreatment. For example, a review by Silva-Fernandez et al. (2023) emphasized the psychological toll of obstetric violence, linking it to both postpartum depression and postpartum posttraumatic stress disorder (PTSD). The authors identified risk pathways such as medical coercion and dissatisfaction with newborn care as key contributors. Similarly, O’Neill (2023) demonstrated that obstetric violence significantly predicted both postpartum depression and anxiety.
Building on this growing body of evidence, the present study aims to examine the psychological processes through which obstetric violence may be associated with postpartum mental health outcomes. In particular, perceived partner support, a construct widely studied in social and interpersonal relationship psychology, is considered a potential explanatory pathway in the relationship between experiences of obstetric violence and symptoms of postpartum depression. This focus is especially relevant given the central role of close relationships in shaping women's emotional adjustment during the perinatal period.
Perceived Partner Support as a Link Between Obstetric Violence and Postpartum Depression
Perceived partner support represents a key social psychological variable in this context. A substantial body of research indicates that women reporting lower levels of social support during pregnancy and childbirth also tend to report higher levels of postpartum depressive symptoms (Cho et al., 2022; Nugrahaeni et al., 2022; Xie et al., 2009). In particular, partner support has consistently been identified as an important relational resource associated with maternal psychological well-being (Damsarsan & Ören, 2024; Gremigni et al., 2011; Kızılırmak et al., 2021; Misri et al., 2000). For example, Martinez-Vázquez et al. (2021) found that 67.4% of women in their sample reported experiencing some form of obstetric violence, and verbal and psychoemotional abuse were associated with a greater risk for postpartum PTSD. Their findings also highlighted social support as an important buffering context. Although prior studies have documented associations among obstetric violence, partner support, and maternal mental health, they have not directly examined whether perceived partner support may help explain the observed link between obstetric violence and postpartum depressive symptoms. The present study aims to address this gap by investigating perceived partner support as a potential mediating pathway while acknowledging that these relationships may be interrelated rather than strictly unidirectional.
Building on this, the present study examines perceived partner support as a potential mediator in the pathway from obstetric violence to postpartum depressive symptoms. Specifically, the study tests whether experiences of obstetric violence negatively affect perceived partner support, which in turn contributes to higher postpartum depression levels.
Disentangling Perceived Partner Support from Actual Partner Support
In social psychological research, a well-established distinction is made between actual and perceived social support. Actual support refers to tangible, observable forms of assistance that an individual receives from others, such as help with daily tasks, childcare, or financial aid (Cohen & Wills, 1985). In contrast, perceived support reflects an individual's subjective appraisal or belief that support is available if needed and that one is cared for, valued, and understood by significant others (Lakey & Cassady, 1990). This distinction is important because the psychological effects of support depend not only on what others objectively provide, but also on how such support is experienced and interpreted by the recipient.
A large body of research consistently shows that perceived support is a more robust predictor of psychological well-being than actual support (Uchino, 2009). One explanation for this pattern comes from the stress-buffering hypothesis, which posits that individuals who perceive higher levels of support tend to appraise stressful events as less threatening and more manageable, thereby reducing their emotional impact (Cohen & Wills, 1985; Szkody et al., 2020). Moreover, social cognitive perspectives suggest that perceptions of support are not solely determined by objective support behaviors but are also shaped by individuals’ psychological states and interpretive processes (Lakey & Orehek, 2011). For example, individuals exposed to stressful or traumatic experiences may develop a negativity bias—a tendency to interpret social cues more negatively—which can lead them to underestimate or misperceive available support, even when it is objectively present (Beck, 1976; Gotlib et al., 2004).
These conceptual and theoretical distinctions are particularly relevant in the context of childbirth experiences. In the present study, actual partner support refers to observable behaviors such as being present during labor and assisting with household and childcare responsibilities during the postpartum period. Perceived partner support, in contrast, reflects the woman's subjective sense of being emotionally and practically supported by her partner. This distinction may be especially important when considering experiences of obstetric violence. Women who feel mistreated, disrespected, or powerless during childbirth may have difficulty recognizing or internalizing supportive behaviors from others, even when such support is objectively available. In this sense, obstetric violence may contribute to feelings of emotional vulnerability or disconnection that shape how partner support is perceived, suggesting that perceived support may be influenced not only by partners’ actual behaviors but also by women's broader psychological and experiential context.
Given these dynamics, the present study focuses on perceived partner support as a psychologically salient construct that may help explain variation in postpartum depression. Specifically, obstetric violence may be associated with how women perceive support from their partners, which in turn may relate to their postpartum depressive symptoms. Although indicators of actual partner support (e.g., partner presence during labor, assistance with domestic work and childcare) are included in the analyses as control variables, the primary emphasis is placed on the subjective experience of support. This approach allows for a more nuanced understanding of how interpersonal perceptions may be linked to the psychological consequences of obstetric violence.
Present Research
The primary aim of the present research was to examine whether perceived partner support serves as a psychological mechanism linking experiences of obstetric violence to symptoms of postpartum depression. Drawing on the previous literature (O’Neill, 2023; Silva-Fernandez et al., 2023), it was first hypothesized that higher levels of obstetric violence would be associated with higher levels of postpartum depressive symptoms (Hypothesis 1).
Building on prior findings, we further hypothesized that greater exposure to obstetric violence would be associated with lower levels of perceived partner support (Hypothesis 2). In addition, the study aimed to distinguish perceived partner support from actual, observable forms of partner involvement. Accordingly, it was expected that indicators of actual partner support would not moderate the association between obstetric violence and perceived partner support, nor the association between obstetric violence and postpartum depression.
The central hypothesis of the study was that perceived partner support would mediate the positive association between obstetric violence and postpartum depression (Hypothesis 3). This hypothesis was designed to examine whether obstetric violence may be linked to postpartum depressive symptoms through its association with women's perceptions of support from their partners.
In addition to the hypothesis-driven analyses, exploratory analyses were conducted to examine whether birth-related characteristics—such as mode of delivery (vaginal vs. cesarean), pregnancy planning status (planned vs. unplanned), and frequency of prenatal visits—as well as demographic factors including age, education, and socioeconomic status, were associated with experiences of obstetric violence.
Method
Ethical approval for this study was obtained from the Scientific Research and Publication Ethics Committee of Anadolu University, Faculty of Social and Humanities Sciences (Project number: 748483). The questionnaire (in both Turkish and English), dataset, and analysis outputs are accessible via the link: https://osf.io/sqb9y/files/osfstorage?view_only=.
Design and Participants
This was a cross-sectional study.
The sample of the current study consisted of women, residing in Turkey, who had given birth within the past 18 months, as this period is known to have the highest prevalence of postpartum depression (Durukan et al., 2011; Monti et al., 2008). The model examining the mediating role of perceived partner support in the relationship between obstetric violence and postpartum depression had not been previously explored in the literature and was being investigated for the first time in this study. Therefore, there was a limited number of studies in the literature that could guide the sample size estimation based on effect size for the current study. A review of these few studies indicated that the effect size may range from small to medium (Cetin et al., 2023; Kömürcü-Akik, 2023; Martinez-Vazquez et al., 2021). For instance, in the study published by Martinez-Vazquez and colleagues (2021), the effect size of the relationship between obstetric violence and postpartum depression was found to be moderate (adjusted OR = 2.63). On the other hand, in another study conducted in Turkey examining the predictive relationship between obstetric violence and depression (Cetin et al., 2023), the effect size was relatively small (adjusted OR = 0.37). Taking into account the general tendency of low effect sizes in social psychology research (Götz et al., 2022; Lovakov & Agadullina, 2021; Richard et al., 2003), the effect size for the sample size estimation in the current study was set at a small level (f2 = 0.2). Using the small effect size (power = 0.80, alpha = .05), power analyses conducted in G*Power version 3.1 (Erdfelder et al., 1996) indicated a sample size of 485 was necessary to detect a comparable effect; ultimately, 535 participants were recruited online.
The age of participants ranged from 20 to 49 years, with a mean of 30.56 years (SD = 4.53). The duration of participants’ most recent pregnancies ranged from 27 to 42 weeks, with a mean of 38.54 weeks (SD = 1.79). Monthly household income, reported by participants, ranged from 0 to 500,000 Turkish Lira (TL), with a mean income of 44,314.69 TL (SD = 42,517.74). The age of participants’ babies ranged from newborn (0 months) to 18 months, with a mean of 9.51 months (SD = 5.13). Complete details regarding the participants are presented in Table 1.
Participants’ Characteristics.
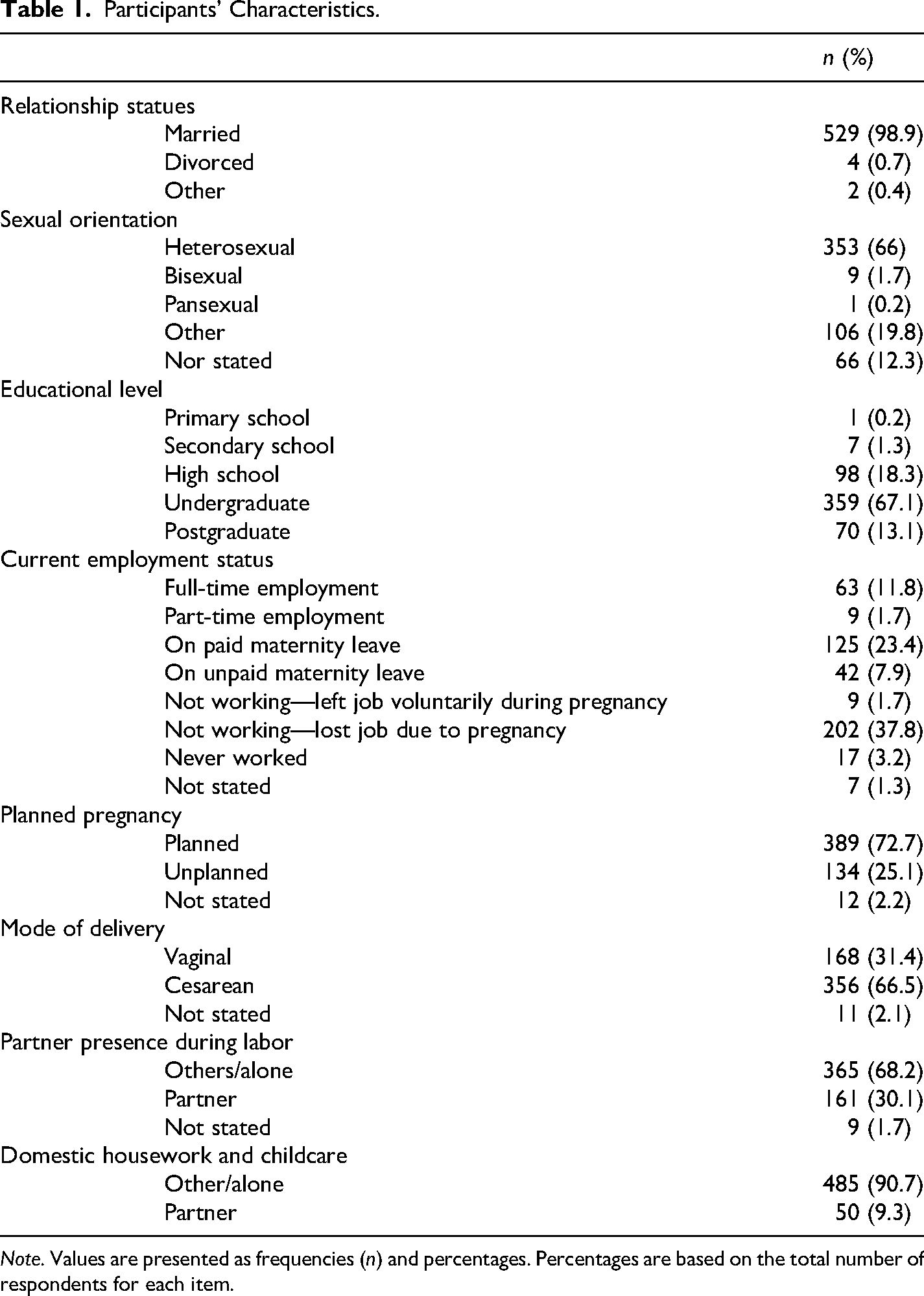
Note. Values are presented as frequencies (n) and percentages. Percentages are based on the total number of respondents for each item.
Materials
Obstetric Violence
Obstetric Abuse and Violence
The Obstetric Violence Scale, originally developed by Castro and Frías (2020) and adapted into Turkish by Kömürcü-Akik (2023), consists of two subscales. Participants responded to each of the 11 items using a binary response format (“Yes” or “No”). Responses were scored such that each “Yes” answer received 1 point and each “No” answer received 0 points. A total score was then calculated by summing the responses, with higher scores indicating greater exposure to obstetric violence.
The first subscale, Abuse and Violence, includes seven items that assess direct experiences of mistreatment, such as “Have you been yelled at or scolded?” The second subscale, Nonconsented Care, comprises four items addressing medical interventions performed without consent. A sample item from this dimension is: “During childbirth, were any birth control methods applied or were you operated on or sterilized to stop you from having children without your knowledge or consent? (e.g., tubal ligation).”
Exploratory factor analysis indicated that the scale was suitable for factorization, as evidenced by an adequate Kaiser–Meyer–Olkin value (KMO = 0.81) and a significant Bartlett's Test of Sphericity (χ2(55) = 938.64, p < .001). Principal component analysis revealed a two-factor structure with eigenvalues greater than 1. The first factor accounted for 28.16% of the variance, while the second factor explained 11.50%, with a total explained variance of 39.66%. Most items loaded strongly on the first factor, representing direct experiences of obstetric mistreatment, including verbal abuse, neglect, and coercive care, with generally acceptable communalities. In contrast, the second factor, reflecting nonconsented medical interventions, showed weaker loadings and notably low communalities for several items, including one item with near-zero shared variance. This pattern was consistent with reliability analyses, which indicated acceptable internal consistency for the Abuse and Violence subscale (α = .71) but very poor reliability for the Nonconsented Care subscale (α = .13). Taken together, these findings suggest that the second factor did not constitute a statistically stable or internally consistent dimension in this sample. Therefore, only the Abuse and Violence factor was retained and used in subsequent analyses.
Perceived Obstetric Violence
It was measured using two items developed by the researchers: “Was the attitude of the healthcare person(s) present during your labor and delivery negative?” and “Do you think the healthcare person(s) present during your labor and delivery acted violently toward you?” Participants responded to both items using a binary format (“Yes” or “No”), consistent with the Obstetric Violence Scale. The two items were correlated, r = .49, p < .001, and were therefore combined into a single variable for use in the analyses.
Perceived Partner Support
It was assessed using the Scale of Perceived Spousal Support During Early Postpartum Period, developed by Hotun-Şahin et al. (2014) based on a sample from Turkey. The scale includes 16 items rated on a 5-point Likert scale, ranging from strong disagreement to strong agreement. Participants respond to items reflecting their perceptions of support from their spouse during the prenatal and postpartum periods. An example item is: “My spouse showed me love and affection during my pregnancy and postpartum period.” Higher scores indicate greater perceived support from one's partner. In the current study, the scale demonstrated excellent internal consistency (α = .95).
Actual Partner Support
It was measured using two dichotomous indicators developed by the researchers. The first item assessed whether the partner was the primary source of domestic and childcare support (coded as: partner = 2, other or alone = 1). The second item asked whether the partner was present during labor (coded as: partner present = 2, someone else or no one present = 1). These two items reflect the observable and practical aspects of support provided by the partner during the perinatal and postpartum periods.
Postpartum Depression
The Edinburgh Postnatal Depression Scale, originally developed by Cox et al. (1987) and adapted into Turkish by Engindeniz et al. (1996), was used to measure postpartum depression. It was a 10-item self-report measure designed to assess the risk of postpartum depression. Each item is rated on a 4-point Likert scale ranging from 0 to 3, with total scores ranging from 0 to 30. Higher scores indicate a greater likelihood of experiencing postpartum depressive symptoms. Participants are asked to evaluate how they have felt during the past 7 days, responding to items such as “I have blamed myself unnecessarily when things went wrong.” In the current study, the scale demonstrated high internal consistency (α = .89), and thus, it was utilized as a single composite measure.
Demographic Information
A demographic information form was used to collect participants’ background characteristics as well as details regarding their pregnancy, childbirth, and infant. Participants were asked to provide information in the following order: age, relationship status, sexual orientation, education level, monthly income, current employment status, the age of their newborn, the duration of their most recent pregnancy, whether the pregnancy was planned, the mode of delivery, and the frequency of prenatal visits.
Statistical Analysis
All analyses were conducted using SPSS IBM version 24. Hypotheses 1 and 2 were tested with correlation analysis. Mediation (Hypothesis 3) was tested with PROCESS macro Model 4 using 5,000 bootstrapped samples to generate 95% bias-corrected confidence intervals (CIs). Moderation analyses were conducted with PROCESS macro Model 1 using 5,000 bootstrapped samples to generate 95% bias-corrected CIs to examine whether actual partner support—operationalized as partner-provided domestic and childcare support and presence during labor—moderated the effects of obstetric violence on perceived partner support and postpartum depression. Each moderator was tested in a separate model.
Results
Descriptive statistics and bivariate correlations were conducted among the primary study variables: obstetric abuse and violence, perceived obstetric violence, perceived partner support, and postpartum depression and participants’ demographic characteristics, including age, educational level, and socioeconomic status. A comprehensive summary of the results is provided in Table 2.
Correlation Matrix, Means, Range, and Standard Deviations for Age, Educational Level, Socioeconomic Status, Frequency of Prenatal Visits, Obstetric Abuse and Violence, Perceived Obstetric Violence, Perceived Partner Support, and Postpartum Depression.
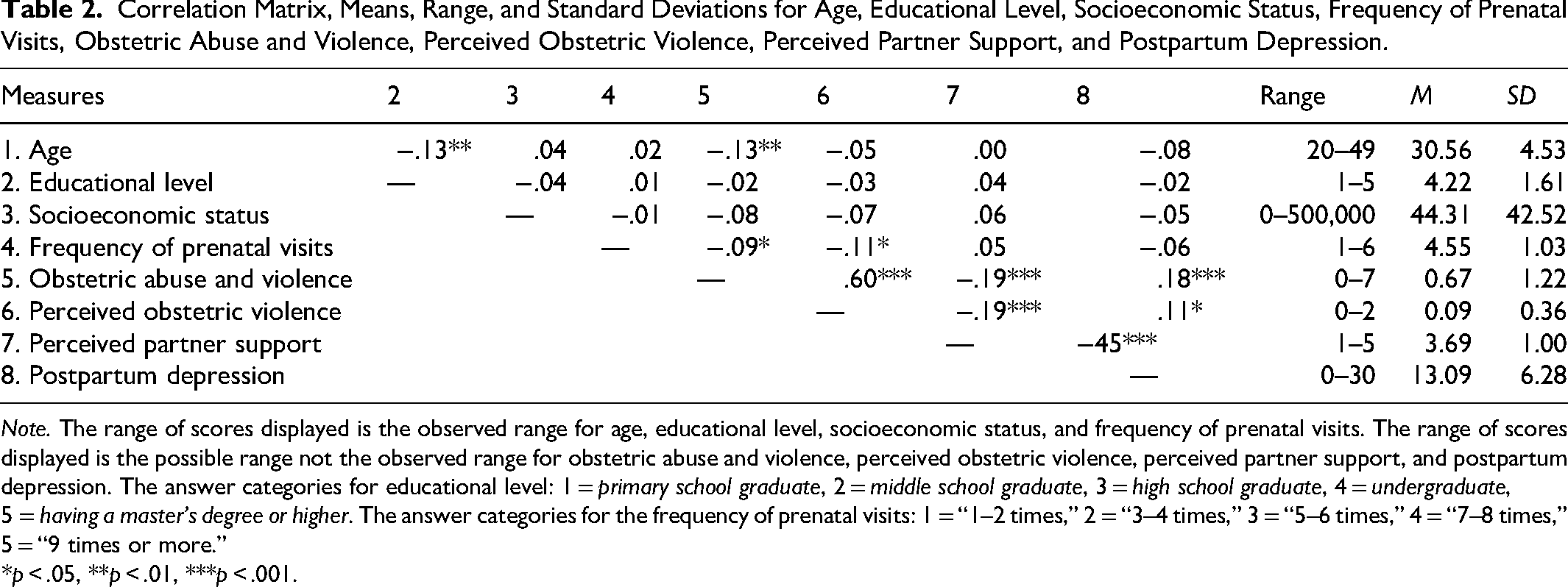
Note. The range of scores displayed is the observed range for age, educational level, socioeconomic status, and frequency of prenatal visits. The range of scores displayed is the possible range not the observed range for obstetric abuse and violence, perceived obstetric violence, perceived partner support, and postpartum depression. The answer categories for educational level: 1 = primary school graduate, 2 = middle school graduate, 3 = high school graduate, 4 = undergraduate, 5 = having a master's degree or higher. The answer categories for the frequency of prenatal visits: 1 = “1–2 times,” 2 = “3–4 times,” 3 = “5–6 times,” 4 = “7–8 times,” 5 = “9 times or more.”
*p < .05, **p < .01, ***p < .001.
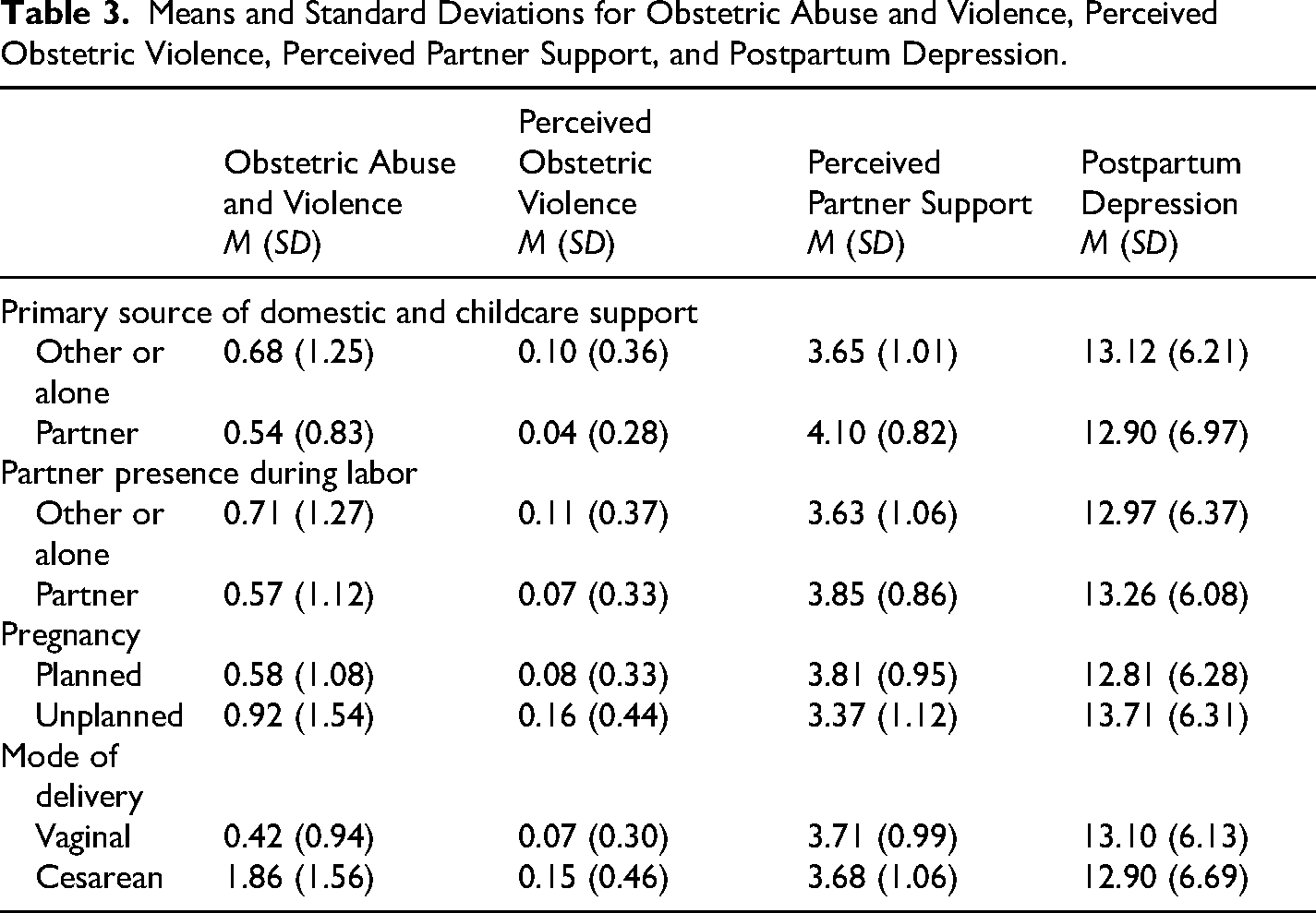
Means and SDs broken down by actual partner support (i.e., partner as main domestic and childcare supporter: yes vs. no and partner presence during labor: yes vs. no), planned pregnancy (planned vs. unplanned), mode of delivery (vaginal vs. cesarean), the presence of domestic support (yes vs. no), and breastfeeding status (yes vs. no) are presented in Table 3.
Means and Standard Deviations for Obstetric Abuse and Violence, Perceived Obstetric Violence, Perceived Partner Support, and Postpartum Depression.
Preliminary Analyses
Both obstetric abuse and violence and perceived obstetric violence were associated with higher postpartum depression, confirming Hypothesis 1. In addition, as hypothesized (Hypothesis 2), both were linked to lower perceived partner support, meaning that higher levels of mistreatment during childbirth were associated with reduced perceptions of support from partners. Also, a significant negative association was observed between perceived partner support and postpartum depression, suggesting that greater perceived support from a partner is linked to lower depressive symptomatology in the postpartum period.
To better understand the distinction between actual and perceived partner support, we examined whether women's reports of objective partner involvement were associated with their subjective perceptions of support. Actual partner support was assessed using two dichotomous indicators: whether the partner was the primary source of domestic and childcare support (partner vs. other/alone), and whether the partner was present during labor (partner present vs. someone else present/alone). As presented in Table 3, women who identified their partner as the main provider of domestic and childcare support reported significantly higher levels of perceived partner support compared to those who received support from someone else or managed alone, t(522) = −2.98, p < .01, 95% CI [−0.74, −0.15]. Similarly, women whose partners were present during labor reported greater perceived partner support than those who were accompanied by someone else or were alone during childbirth, t(513) = −2.25, p < .05, 95% CI [−0.40, −0.03].
Moderation analyses assessed whether actual partner support moderated the relationships between obstetric violence and perceived partner support (first model), and between obstetric violence and postpartum depression (second model).
In the first model, none of the interaction effects was statistically significant. The interaction between obstetric violence and abuse and having the partner as the primary source of domestic and childcare support did not predict perceived partner support, b = –0.09, SE = 0.17, p = .61, 95% CI [–0.43, 0.25]. Similarly, perceived obstetric violence did not interact significantly with this variable, b = –0.32, SE = 0.51, p = .53, 95% CI [–1.33, 0.69]. The interaction between obstetric violence and abuse and partner presence during labor was also nonsignificant, b = –0.05, SE = 0.08, p = .53, 95% CI [–0.21, 0.11], as was the interaction between perceived obstetric violence and partner presence, b = 0.13, SE = 0.27, p = .64, 95% CI [–0.42, 0.67].
In the second model, none of the interaction terms significantly predicted postpartum depression. Obstetric violence did not interact with either partner as the main domestic and childcare supporter, b = −0.07, SE = 1.08, p = .94, 95% CI [–2.20, 2.05], or partner presence during labor, b = 0.49, SE = 0.51, p = .39, 95% CI [–0.51, 1.49]. Similarly, perceived obstetric violence showed no significant interaction with domestic and childcare support, b = −2.57, SE = 3.25, p = .43, 95% CI [–8.96, 3.81], or partner presence, b = 0.28, SE = 1.76, p = .87, 95% CI [–3.18, 3.74].
These results suggest that although actual partner support is associated with perceived partner support, it does not alter the strength or direction of the relationship between obstetric violence and either perceived partner support or postpartum depression. Therefore, actual partner support variables were included as control variables (i.e., confounders) in subsequent mediation analyses to account for their influence on the perception of support.
The Mediating Role of Perceived Partner Support
Given their lack of moderating effect but significant associations with perceived support, actual partner support variables were included as control variables in the mediation model. The results of these analyses are illustrated in Figures 1 and 2, with obstetric abuse and violence, and perceived obstetric violence, examined as the respective primary predictors.
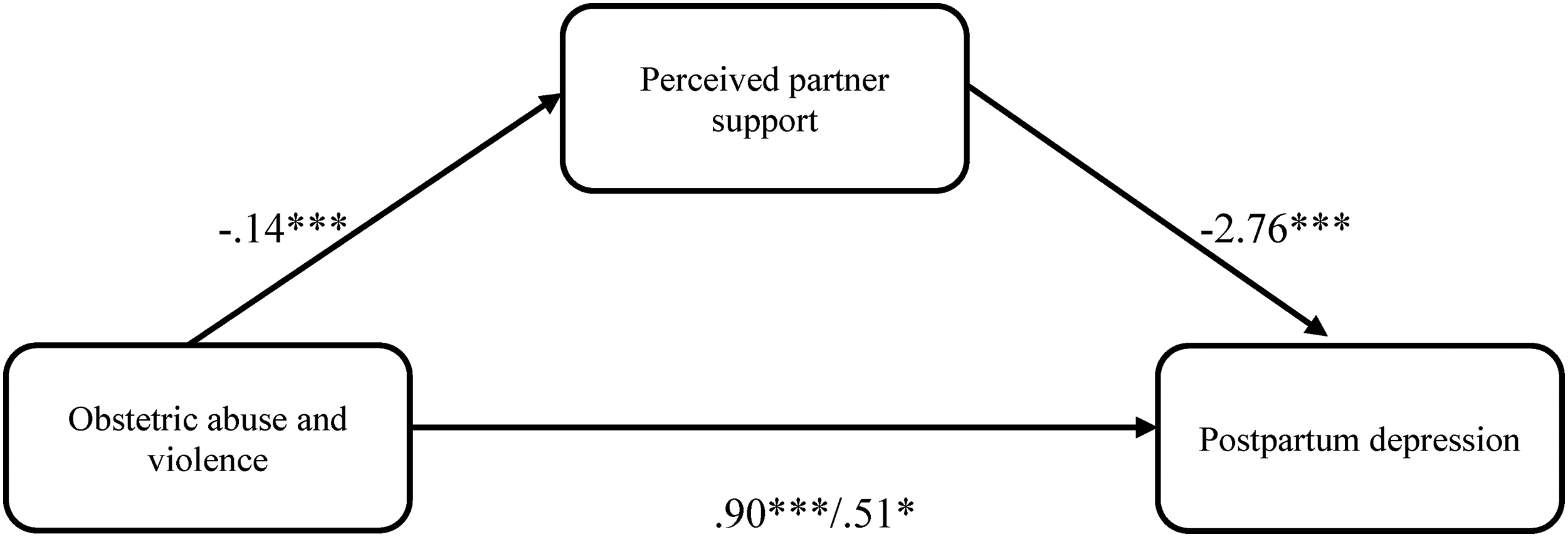
Mediational model with obstetric abuse and violence predicting postpartum depression through perceived partner support.
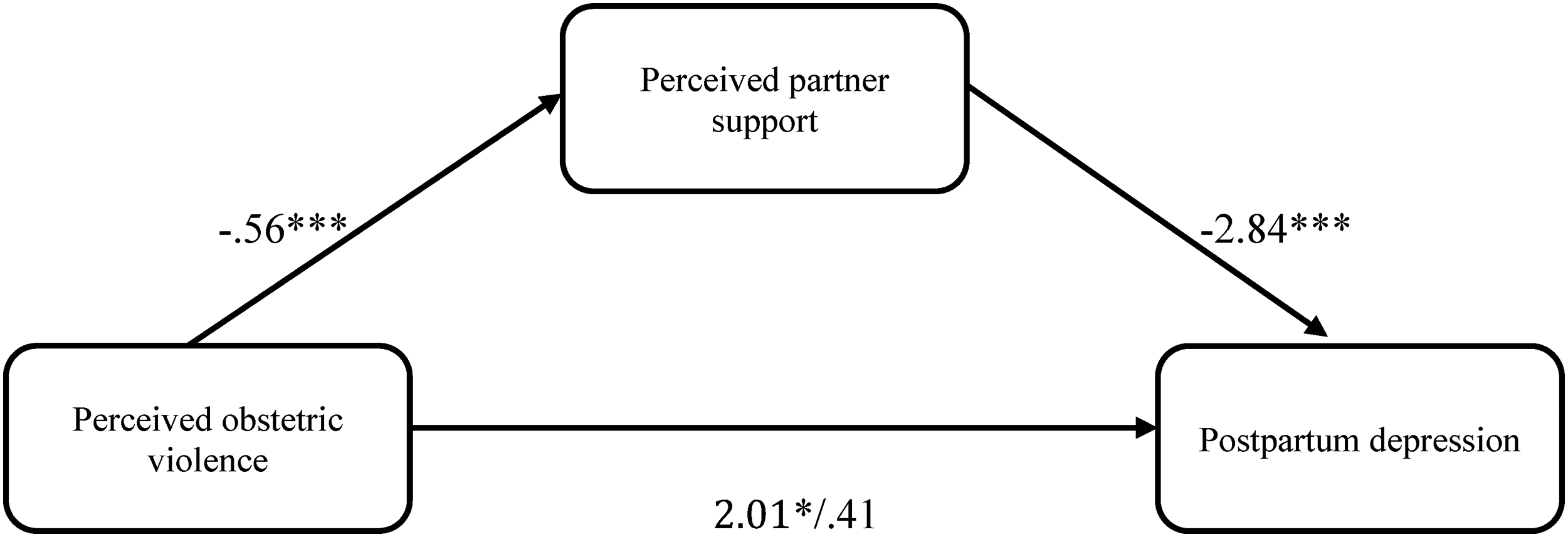
Mediational models with perceived obstetric violence predicting postpartum depression through perceived partner support.
In our first model with obstetric abuse and violence as the primary predictor (Figure 1), the positive association between obstetric abuse and violence and postpartum depression was found to be statistically significant as hypothesized, b = 0.90, SE = 0.22, p < .001, 95% CI [0.47, 1.35]. Furthermore, obstetric abuse and violence significantly predicted perceived partner support, b = −0.14, SE = 0.04, p < .001, 95% CI [−0.21, −0.07], with those reporting greater obstetric abuse and violence also reporting less perceived partner support. Finally, when including perceived partner support as a predictor along with obstetric abuse and violence, the effect of obstetric abuse and violence on postpartum depression became smaller in magnitude, b = 0.51, SE = 0.20, p < .05, 95% CI [0.10, 0.91], and the effect of perceived partner support on postpartum depression was significant, b = −2.76, SE = 0.25, p < .001, 95% CI [−3.25, −2.26]. These results indicated that the relationship between obstetric abuse and violence and postpartum depression was partially mediated by perceived partner support (indirect effect = 0.39, SE = 0.13, 95% CI [0.15, 0.64]). Overall, this model was significant and accounted for approximately 22% of the variance in postpartum depression, F(4, 497) = 35.13, p < .001, R2 = 0.22, supporting Hypothesis 3.
To further examine the robustness and potential directionality of the observed relationships, an alternative mediation model was tested in which postpartum depression was specified as the mediator between obstetric abuse and violence and perceived partner support. The results indicated that obstetric abuse and violence significantly predicted postpartum depression, b = 0.90, SE = 0.22, p < .001, 95% CI [0.46, 1.34]. In turn, postpartum depression was negatively associated with perceived partner support, b = −0.07, SE = 0.01, p < .001, 95% CI [−0.08, −0.06], indicating that higher depressive symptoms were related to lower perceived support. When postpartum depression was included in the model alongside obstetric abuse and violence, the direct effect of obstetric abuse and violence on perceived partner support decreased in magnitude but remained statistically significant, b = −0.09, SE = 0.03, p < .01, 95% CI [−0.16, −0.03]. Bootstrapped mediation analyses confirmed a significant indirect effect of obstetric abuse and violence on perceived partner support through postpartum depression, indirect effect = −0.06, SE = 0.02, 95% CI [−0.10, −0.03]. Overall, this alternative model was statistically significant and accounted for approximately 22% of the variance in perceived partner support, F(2, 508) = 70.31, p < .001, R2 = 0.22.
In a second step, the model was retested to examine whether perceived partner support mediated the association between perceived obstetric violence and postpartum depression (Figure 2). As observed in the prior analyses, the positive association between perceived obstetric violence and postpartum depression was found to be statistically significant, b = 2.01, SE = 0.78, p < .05, 95% CI [0.48, 3.54]. Furthermore, perceived obstetric violence significantly predicted perceived partner support, b = −0.56, SE = 0.12, p < .001, 95% CI [−0.80, −0.32], with those reporting greater perceived obstetric violence also reporting less perceived partner support. Finally, when perceived partner support was added as a predictor alongside perceived obstetric violence, the association between perceived obstetric violence and postpartum depression was no longer statistically significant, b = 0.41, SE = 0.71, p = .56, 95% CI [−0.98, 1.81], and perceived partner support had a significant effect on postpartum depression, b = −2.84, SE = 0.25, p < .001, 95% CI [−3.33, −2.34]. We found evidence for an indirect effect of perceived obstetric violence on postpartum depression through perceived partner support, indirect effect = 1.60, SE = 0.39, 95% CI [0.79, 2.35]. Overall, this model was significant and accounted for approximately 21% of the variance in postpartum depression, F(4, 502) = 33.51, p < .001, R2 = 0.21.
To further examine the potential directionality of these associations, an alternative mediation model was tested in which postpartum depression was specified as the mediator between perceived obstetric violence and perceived partner support. Results indicated that perceived obstetric violence significantly predicted postpartum depression, b = 1.96, SE = 0.77, p < .05, 95% CI [0.44, 3.48]. In turn, postpartum depression was negatively associated with perceived partner support, b = −0.07, SE = 0.01, p < .001, 95% CI [−0.08, −0.06], indicating that higher depressive symptoms were related to lower perceived support. When postpartum depression was included in the model alongside perceived obstetric violence, the direct effect of perceived obstetric violence on perceived partner support decreased in magnitude but remained statistically significant, b = −0.45, SE = 0.11, p < .001, 95% CI [−0.67, −0.23]. Bootstrapped mediation analyses confirmed a significant indirect effect of perceived obstetric violence on perceived partner support through postpartum depression, indirect effect = −0.14, SE = 0.06, 95% CI [−0.26, −0.02]. Overall, this alternative model was statistically significant and accounted for approximately 23% of the variance in perceived partner support, F(2, 513) = 76.10, p < .001, R2 = 0.23.
Exploratory Analyses
In addition to the primary analyses, several other variables measured in the study were examined for exploratory purposes. These included factors such as planned pregnancy and age, which have been suggested in the literature to relate to obstetric violence. The current section presents these exploratory findings to provide a broader context for understanding the indicators of obstetric violence beyond the core mediation models.
The analysis revealed a significant negative correlation between age and obstetric abuse and violence, indicating that as age increased, reports of such experiences decreased. Although there was a negative correlation between age and perceived obstetric violence, this association did not reach statistical significance. Additionally, educational level and socioeconomic status did not significantly predict experiences of obstetric abuse and violence or perceived obstetric violence. However, a higher frequency of prenatal visits was significantly linked to lower levels of both obstetric abuse and violence and perceived obstetric violence (shown in Table 2).
Planned pregnancy (planned vs. unplanned), mode of delivery (vaginal vs. cesarean), and partner presence during labor (partner present vs. someone else present/alone) were included in the analyses for descriptive purposes to explore the indicators of obstetric violence. As shown in Table 3, the findings of the t test indicated that compared to women with planned pregnancies, women who had unplanned pregnancies reported significantly higher levels of both obstetric abuse and violence, t(515) = −2.82, p < .01, 95% CI [−0.59, −0.10], and perceived obstetric violence, t(520) = −2.20, p < .05, 95% CI [−0.15, −0.01]. Regarding mode of delivery, women who underwent vaginal birth reported greater experiences of obstetric abuse, t(516) = −6.91, p < .001, 95% CI [−0.98, −0.55], and violence and higher perceived obstetric violence, t(521) = −2.24, p < .05, 95% CI [−0.14, −0.01], compared to those who had cesarean deliveries. The results showed that women who were with someone other than their partner or alone during delivery reported higher levels of obstetric abuse and violence compared to those accompanied by their partner; however, this difference did not reach statistical significance, t(527) = 0.780, p = .43, 95% CI [−0.21, 0.50]. Similarly, there was no significant difference between these two groups in terms of perceiving obstetric violence, t(532) = 1.1534, p = .25, 95% CI [−0.04, 0.16].
Discussion
The present study investigated the psychological mechanisms linking obstetric violence and postpartum depression, with a particular focus on the mediating role of perceived partner support. Consistent with expectations, both obstetric abuse and perceived obstetric violence were positively associated with postpartum depression and negatively associated with perceived partner support. In turn, perceived partner support was significantly associated with lower levels of postpartum depression. Mediation analyses further indicated that perceived partner support accounted for the relationship between obstetric violence and postpartum depression, even after controlling for actual partner support indicators such as partner presence during labor and domestic support. These findings highlight the importance of perceived partner support as a psychologically meaningful variable in the context of birth-related mistreatment and maternal mental health.
First, consistent with the study's hypothesis and prior findings (Kohan et al., 2025; O’Neill, 2023; Silva-Fernandez et al., 2023), obstetric violence was positively associated with postpartum depression. This relationship was examined using two indicators: one capturing direct experience of obstetric abuse and violence, and the other assessing women's subjective perception of having experienced obstetric violence. Both measures yielded converging results, reinforcing the robustness of the association. This replication is particularly noteworthy for two reasons. First, the empirical investigation of obstetric violence remains a relatively new and evolving area of study (Fraser et al., 2025; Hakimi et al., 2025), making the replication of initial findings such as the link between obstetric violence and postpartum depression especially critical for establishing a reliable evidence base. Second, given the broader replication crisis in psychological science (Bogdan, 2025; Malich & Munafò, 2022), finding the same link between obstetric violence and postpartum depression across different measures adds strength and reliability to the field of psychology.
Second, as anticipated, the negative impact of obstetric violence on perceived partner support was statistically significant. To our knowledge, this is a novel finding in the literature. While one prior study (Vega-Sanz et al., 2025) examined the role of perceived social support in the context of obstetric violence and postpartum depression, that study focused on the general protective function of social support in relation to depression, rather than investigating how obstetric violence may specifically diminish perceived support. Moreover, the support in that study was measured broadly, encompassing family and friends rather than focusing on support from a partner. In this regard, the present study offers a unique contribution by identifying perceived partner support as a mechanism through which obstetric violence may undermine maternal well-being.
Another key contribution of this study lies in its examination of how exposure to obstetric violence may be associated with women's perceptions of partner support and postpartum depressive symptoms. The findings suggest a potential pathway in which experiences of obstetric violence are linked to lower perceived partner support, which is in turn related to higher levels of postpartum depression. This relational pattern has received limited attention in previous research and therefore represents an important addition to the literature. Rather than reflecting only a direct association with postpartum depression, obstetric violence may also be linked to women's access to psychological resources that typically help buffer distress.
A related line of research has also highlighted the role of relationship factors in linking childbirth experiences to parental mental health outcomes (Seefeld et al., 2024). This recent study using dyadic models has shown that more positive birth experiences are associated with higher relationship satisfaction and lower levels of depression and anxiety among both mothers and their partners, with relationship satisfaction partially mediating these associations. While these findings converge with the present results in emphasizing the importance of relational processes in understanding psychological adjustment following childbirth, the current study extends this literature in several important ways. First, prior research has primarily focused on overall birth experience quality, whereas the present study specifically examines obstetric violence as a distinct and adverse form of childbirth experience. Second, existing studies typically assess general relationship satisfaction, whereas this study focuses on perceived partner support as a more proximal, social–psychological construct. Together, these distinctions suggest that beyond general relationship dynamics, women's subjective perceptions of support may represent a particularly relevant pathway through which negative childbirth experiences are linked to postpartum mental health.
At the same time, it is also possible that depressive symptoms themselves influence how partner support is perceived, suggesting that these relationships may be reciprocal rather than strictly unidirectional. Accordingly, the present findings are best understood as reflecting interconnected psychological and interpersonal processes rather than definitive causal effects. This perspective underscores the broader psychological significance of the results while acknowledging the limitations inherent in cross-sectional data.
To examine potential directionality, two alternative mediation models were tested in which postpartum depression was specified as the mediator and perceived partner support as the outcome. In both models, obstetric abuse and violence and perceived obstetric violence were positively associated with postpartum depression, which in turn was linked to lower perceived partner support. Bootstrapping analyses confirmed significant indirect effects, although the direct effects of obstetric violence on perceived partner support remained significant, indicating partial mediation. These findings suggest that the associations among obstetric violence, depressive symptoms, and perceived support may be interconnected and potentially bidirectional.
Despite the statistical significance of these alternative pathways, the proposed model in which perceived partner support mediated the relationship between obstetric violence and postpartum depression appears to be theoretically and empirically more robust. From a theoretical perspective, this specification aligns more closely with the established stress and coping frameworks, which conceptualize social support as a key psychosocial resource through which stressors influence mental health outcomes. Obstetric violence represents an external adverse event, whereas perceived support and depressive symptoms reflect psychological responses that unfold subsequently. Empirically, the proposed model demonstrated stronger explanatory power for postpartum depression and yielded larger indirect effects, whereas the alternative models showed comparatively smaller indirect effects and primarily explained variance in perceived support rather than in mental health outcomes. Taken together, these considerations suggest that the findings are best interpreted as supporting a process-oriented pathway in which obstetric violence may contribute to postpartum depressive symptoms partly through its impact on women's perceptions of partner support, while still acknowledging the possibility of bidirectional influences among these variables.
Next, to clarify the distinction between actual and perceived support, women's reports of objective partner involvement, such as presence during labor and contributions to domestic and childcare tasks, were examined. While actual partner support was positively associated with perceived support, moderation analyses showed that it did not significantly influence the relationship between obstetric violence and either perceived support or postpartum depression. These results indicate that, although actual support may shape perceptions, it does not buffer the psychological consequences of obstetric violence. As a result, actual support variables were treated as covariates in the mediation models. Indeed, findings from social psychology suggest that perceived social support plays a more crucial role than actual support in managing stress, as stress may impair individuals’ capacity to recognize, interpret, or utilize the support available to them (Cohen & Wills, 1985; Lakey & Cassady, 1990; Uchino, 2009).
These findings highlight the critical need to address the attitudes and behaviors of healthcare professionals. The existing interventions aimed at reducing obstetric violence have largely focused on training and educating medical staff (for a review, see Yalley et al., 2024), a strategy that this study supports as effective in mitigating the adverse consequences of mistreatment during childbirth. While postpartum interventions that involve the partner remain important, the current results suggest that partner-focused approaches alone may not be sufficient to prevent postpartum depression. As such, prioritizing interventions directed at healthcare providers or healthcare systems, particularly through training programs designed to prevent obstetric violence, should remain a central focus in efforts to improve maternal mental health outcomes.
Furthermore, in exploratory analyses, several demographic and birth-related variables were examined to better understand potential indicators of obstetric violence. For example, a higher frequency of prenatal visits was associated with lower reports of obstetric abuse and violence, suggesting that regular engagement with healthcare services may offer some protective value. This pattern may be partly explained by psychological theories emphasizing the role of exposure and interpersonal contact in reducing harmful behavior. A growing body of research suggests that increased familiarity through repeated interaction enhances empathy, reduces prejudice, and promotes prosocial conduct. For instance, Zajonc's (1968) mere exposure effect highlights how repeated contact fosters positive feelings, while Allport's (1954) contact hypothesis emphasizes the prejudice-reducing effects of meaningful social interaction. Similarly, theories of deindividuation (Zimbardo, 1969) and empathy (Batson et al., 1991) underscore the importance of recognizing others as individuals in fostering compassion and accountability. In this context, regular prenatal care may reduce the risk of obstetric mistreatment by increasing face-to-face interactions between women and healthcare providers, thereby humanizing the clinical relationship and discouraging dehumanizing treatment.
In addition, women who gave birth vaginally reported significantly higher levels of both experienced and perceived obstetric violence. This finding may reflect broader systemic dynamics in Turkey, where the c-section rate is among the highest globally, approximately 61% (Ulgu et al., 2023). Vaginal births are often discouraged by healthcare providers, as cesarean delivery is typically preferred due to its perceived efficiency, medicolegal safety, and lower physical demands on staff (Birinci & Parpucu, 2023). In this context, vaginal birth may be devalued, leading to neglectful or coercive treatment during labor. Thus, the elevated violence reports among vaginal births may stem not from the mode of delivery itself, but from institutional attitudes and practices surrounding it.
Lastly, consistent with previous research (Gökçe İşbir et al., 2023; Hakimi et al., 2025), older women reported fewer instances of obstetric abuse and violence, while those with unplanned pregnancies experienced and perceived higher levels of mistreatment. One possible explanation for this pattern is that older women may possess greater familiarity with healthcare systems, stronger communication skills, or higher confidence in interacting with medical professionals, which may reduce their vulnerability to mistreatment. In addition, research on age and gender suggests that women's experiences within institutional settings are shaped by the intersection of ageism and sexism, which can influence how authority, credibility, and respect are attributed to them (Chrisler et al., 2016). Younger women, particularly in highly medicalized contexts such as childbirth, may therefore occupy a more vulnerable social position, making them more susceptible to dismissive or controlling treatment. From this perspective, obstetric violence may reflect broader power dynamics within healthcare interactions, where women's perceived social status, including age, shapes their experiences of care. In contrast, unplanned pregnancies may be associated with greater psychosocial stress, reduced preparedness (Carlander et al., 2023; Sah et al., 2026), and potentially less access to resources, factors that could increase women's susceptibility to negative treatment experiences during childbirth. These interpretations align with broader literature suggesting that social and psychological vulnerabilities can shape women's interactions with healthcare providers and influence their perceptions of care.
In contrast, no significant associations were found between perceived obstetric violence and factors such as education, socioeconomic status, or partner presence during labor, despite earlier studies suggesting otherwise (Hakimi et al., 2025). This discrepancy may reflect contextual differences across healthcare settings, cultural variations in expectations of care, or the possibility that obstetric violence operates through interpersonal and institutional dynamics that are not fully captured by sociodemographic indicators alone (Dasgupta et al., 2025; Preziosi et al., 2025; Silva-Fernandez et al., 2025). Taken together, these findings suggest that while certain demographic and situational factors may be associated with vulnerability to mistreatment, obstetric violence may also represent a broader systemic issue that transcends traditional sociodemographic factors.
Although this study contributes novel insights to the literature, it is not without limitations. Most notably, it is a cross-sectional study. Investigating a process such as depression ideally requires measurements taken both before and after childbirth. In the current study, participants’ levels of depression prior to childbirth were unknown, making it difficult to determine whether the postpartum depression measured here developed as a result of exposure to obstetric violence. Therefore, although the observed association between obstetric violence and postpartum depression aligns with findings repeatedly reported in the literature, longitudinal studies are still needed to more robustly confirm this relationship.
Another potential limitation of the present study concerns the measurement of the actual partner support variable. In this study, actual support was assessed using two binary items: whether the partner was present during labor and whether they provided help with household tasks and childcare during the postpartum period. The use of dichotomous items rather than scaled questions, such as “To what extent does your partner help with domestic and childcare responsibilities?” could be seen as a strength, as it minimized the influence of the participant's subjective interpretation or perception. However, these items may not have been sufficient in number or depth to comprehensively capture the construct of actual support. Specifically, both items primarily assess physical presence or assistance and may overlook other important dimensions of support. Future research should consider using more detailed measures that include various forms of actual support—such as emotional, financial, and practical support—to provide a more nuanced understanding of actual partner involvement.
In conclusion, this study highlights the crucial role of perceived partner support in explaining how obstetric violence contributes to postpartum depression. Findings show that birth-related mistreatment not only affects maternal mental health directly but also disrupts access to key psychological resources, particularly women's perception of partner support.
Footnotes
Ethical Considerations
This study was approved by the Scientific Research and Publication Ethics Committee of Anadolu University (approval no. 748483) on July 2, 2024. All participants provided informed consent prior to enrolment in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.