
Abstract
The association between intimate partner violence (IPV) and poor physical and mental health outcomes for women is well documented. Few studies examined factors that strengthen resilience of women exposed to IPV. A telephone survey was administered to 242 Lebanese and Syrian IPV-exposed women. Resilience was positively associated with age, personal income and negatively associated with household crowding index, depression, anxiety, somatic symptoms, PTSD, food and clothing insecurity, feeling safe, and community support. Resilience significantly mediated the relation between IPV exposure and physical health. Developing programs to strengthen IPV survivors’ resilience may lessen the impact of IPV experiences on their physical health.
Introduction
Intimate partner violence (IPV) is an abuse of power committed by a romantic partner while in a relationship or after separation and includes emotional abuse, physical and/or sexual violence, intimidation and threats, and social or economic deprivation (Miller & McCaw, 2019). IPV is a major public health problem worldwide where one in three women have reported physical and/or sexual partner violence, or sexual violence by a non-partner (WHO, 2021). IPV varies geographically due to differences in cultural norms, economic levels, social systems, and religion mores; with the highest prevalence rates reported in Africa, the Eastern Mediterranean, and South–East Asia regions, followed by the Americas. The high-income areas of Europe and the Western Pacific generally report lower prevalence rates (WHO, 2013).
A meta-analysis of 55 studies encompassing 138,692 participants from 11 Middle Eastern countries reported a 26% prevalence rate for overall abuse, 48.6% for psychological abuse, 28.4% for physical, 19% for economical, 18% for sexual, and 18% for injury (Moshtagh et al., 2023). Studies in Lebanon (Awwad et al., 2014; Rahme et al., 2021; Usta et al., 2007) reported similar prevalence rates of 35% for domestic violence (Usta et al., 2007), 37% for physical violence (Awwad et al., 2014), and 49% for non-physical violence (Rahme et al., 2021). As for Syrian refugees, a study published in Lebanon found that around 20% of participants were victims of gender-based violence (Roupetz et al., 2020), and another in Egypt showed that more than 90% of participants were exposed to psychological control and emotional abuse by their partners, with around 30% sexual violence by their partner (Elbarazi, 2024).
The private nature of family settings contributes to the significant underreporting of IPV, as victims are often reluctant to disclose abuse due to shame and stigma (Dim & Elabor-Idemudia, 2018). Factors associated with IPV include low educational status, high levels of anxiety, and pre-existing psychiatric conditions (Rahme et al., 2021). Despite the prevalence of IPV in Lebanon and some meaningful operational efforts within the health system in Lebanon, violence against women remains underprioritized as a core health system objective as seen in the current Vision 2030 (El Kak et al., 2025). The health care system has failed to identify and refer abused women to care, mostly because the recognition of an abusive pattern in women is blurred by cultural and societal taboos (Usta et al., 2007).
IPV has significant negative psychological and physical consequences for the victims (Howell et al., 2017; Smith et al., 2018). IPV is associated with an increased risk of multiple psychiatric problems that include post-traumatic stress symptoms (PTSD), depression, and anxiety (Bonomi et al., 2009; Howell et al., 2017; Smith et al., 2018); all of which compromise women's functioning in daily life, access to social support, personal safety, and increase their financial hardships (Clark & Jordan, 2021; El-Nimr et al., 2021). A recent literature review showed that the physical effects of IPV often result in worsening menopause symptoms; increasing risks associated with the onset of diabetes and other chronic diseases; contracting sexually transmitted infections; and abusing drugs and alcohol (Stubbs & Szoeke, 2022). IPV survivors are frequent users of the health care system, seeking care from emergency departments or clinics three times more often than baseline, and generating 92% more in healthcare costs (Campbell, 2002).
Although IPV seriously impacts women's lives, how they navigate the experience and respond may depend in large part, on their capacity to remain resilient. Resilience is the ability to overcome adversity, resulting from the interplay between risk and protective factors, rooted in interconnected systems, such as the individual, family, community, and culture (Southwick et al., 2014). Studies show resilience is related to better physical and mental health outcomes (Sánchez & Lopez-Zafra, 2019). The onset of mental health disorders, such as PTSD is inversely related to the individual's resilience (Babić et al., 2020). A high level of resilience also impedes the onset of illness and promotes good health (Babić et al., 2020).
To date, few studies have examined links between IPV exposure, physical and mental health, and resilience, particularly among Middle Eastern populations. Studies conducted with IPV-exposed women in the United States showed resilience was negatively associated with levels of physical (i.e., somatic) and psychological distress (Humphreys, 2003), such as depression, anxiety, anger, and stress (Jose & Novaco, 2016). A study in Iran reported that among victims of IPV resilience was an important determinant in reducing the likelihood of suicide (Hajian et al., 2018).
Given reports of the positive direct effects of individuals’ resilience on their health, the current research aims to study the mediating effect of resilience on the relationship between IPV and the physical and mental health of Lebanese women. Specifically, the study explores how resilience may impact health outcomes among women exposed to IPV with a focus on their health care utilization, perception of their health status, and reproductive health. The study hypothesis is that there is a significant relationship between IPV and physical health, and psychological outcomes, and that resilience would act as a mediator of these relations.
Method
This is a cross-sectional study conducted between November 2022 and January 2023.
Participants
Several non-governmental organizations (NGOs) known to be involved in domestic violence response were contacted and asked to seek the approval of women who used their services in the past 2 years to participate in the research. Women considered eligible were married and currently living in Lebanon, aged 18 to 45 years. We excluded pregnant and postpartum women (within 6 months of delivery) as frequent pregnancy-related healthcare utilization and postpartum mood changes could influence the study outcomes. The NGOs provided the research team with a list of potential participants that included the age, preferred name to be used during data collection, place of residence, phone number to be contacted and the best time to make the call. Trained data collectors contacted participants by phone to obtain oral consent and to schedule a suitable time to administer the survey when participants could ensure privacy. The consented women were then contacted via direct phone calls at the agreed time by trained data collectors. The research protocol and tools were reviewed by the UNFPA and the involved NGOs research board and provided ethical approval.
Measures
Demographics
Participants provided basic demographic information (e.g., age, education, work status, income, number of children, living conditions, nationality, smoking status, exercise, alcohol intake, age at marriage and duration), and their spouses’ information (e.g., age, education, work, smoking status, exercise, alcohol use, and health status). To estimate the household size, the crowding index was calculated from the number of residents and rooms in the home.
Health Status
Participants rated perceptions of their health status using a 4-point scale (1 = poor; 4 = excellent), and the frequency of their use of health care services over the past 6 months and for what reason. The items were summed and averaged to form an index of their reported health status.
Somatic Symptoms
Participants completed the Patient Health Questionnaire (PHQ-15; Kroenke et al., 2002) to measure the severity of somatic symptoms. The 15 items are rated 0 = not bothered at all; to 2 = bothered a lot. This questionnaire was used with Syrian Refugees (Schlechter et al., 2023) and in a Mainland Chinese tertiary hospital (Zhang et al., 2016) with adequate validity. The reliability for the 15 items in current study was α = .81. The 15 items were summed to form a composite variable.
Depression
Participants completed the Patient Health Questionnaire (Kroenke et al., 1999; Spitzer et al., 1999) to measure depressive symptoms occurring in the prior 2weeks. The nine items are rated 0 = never, 1 = some days, 2 = more than half the days, and 3 = nearly every day. The scale was validated to screen for depression in primary care settings (Bruce Arroll et al., 2010), and was translated into Arabic and used with a Saudi Arabian population (AlHadi et al., 2017). The reliability for the nine items in current study was α = .85. The 9 items were summed to form a composite variable.
Anxiety
Participants completed the General Anxiety Disorder (GAD) Scale (Spitzer et al., 2006) to measure anxiety. The seven items are rated 0 = not at all, 1 = several days, 2 = more than half of the days, and 3 = almost every day. The GAD-7 was used with healthcare workers in Lebanon (Sakr et al., 2022) and was validated in Arabic with a Saudi Arabian population (AlHadi et al., 2017). The reliability for the seven items in current study was α = .88. The 7 items were summed to form a composite variable.
Post-Traumatic Stress Disorder (PTSD)
Participants completed the Trauma Symptom Checklist-40 (Briere & Runtz, 1987) to measure symptomatic distress for the past 2 months. The items are rated from 0 (never) to 3 (often). This scale has reliability and validity when screening children for abuse and PTSD (Wherry & Herrington, 2018), and was used with Lebanese medical students (Usta et al., 2014). The reliability for the 40 items in current study was α = .93. The 40 items were summed and averaged to form a composite variable.
Resilience
Participants completed the Conor–Davidson Resilience Scale (CD-RISC) which has 25 questions rated as 0 = never to 4 = all the time. The CD-RISC was translated into Arabic and tested for validity with Lebanese women (Bizri et al., 2022). It was used in a study of Lebanese health care workers (Sakr et al., 2022), and critical care nurses (Mealer et al., 2016). Reliability for the 25 items in current study was α = .90. The 25 items were summed and averaged to form a composite variable.
Intimate Partner Violence
Participants completed the Composite Abuse Scale (CAS; Ford-Gilboe et al., 2016) to measure experiences with IPV over the previous 12 months. The 25 items are first scored as yes = 1; no = 0 indicating an experience with IPV, then if yes, the frequency of IPV was rated as 1 = once, 2 = sometimes, 3 = monthly, 4 = weekly, and 5 = almost daily. The CAS was translated to Arabic using a multi-method approach (Alhabib et al., 2013). Reliability and validity were assessed with a Saudi Arabian population (Alhalal et al., 2019). Reliability in current study was α = .81. The frequency ratings of the 25 items were summed to form a composite variable.
Life Stress
Participants rated seven sources of daily stress using a 3-point scale (0 = not a problem, 2 = major problem), for example, concerns about access to food, medication, clothing, health care services, medications, community support and feeling safe. The seven were summed and averaged to form a composite variable. In this research, feeling safe was defined as the individual's perception of personal security and protection from harm. Environmental factors such as wars, weapons, theft, crime and other form of violence from their surroundings could affect their feeling of being safe, and community support referred to the availability, accessibility and perceived effectiveness of resources within the community that provide protection in situations of harm and how to seek help in cases of IPV.
Statistical Analysis
Descriptive data of the demographics and health related variables was performed using mean and standard deviation for normally distributed variables and proportion for categorical variables. Median was used for the income variables as the data was not normally distributed. Health status was operationalized by the question related to the perception of health with a 4-Likert scale. Simple linear regressions were performed to assess the association between pairs of violence, resilience, and health. Then, Sobel test was used to measure whether resilience is mediator in the relationship between violence and health. Regarding the associated factors of resilience, one-way ANOVA was used for categorical variables and Pearson correlation for continuous variables. IBM SPSS Statistical Software 24 was used for data analysis. P-value was set at 0.05. A power analysis was conducted using G*Power version 3.1.9.7 (Faul et al., 2007) to determine the minimum sample size required to test the study hypotheses. Results indicated the required sample size to achieve 80% power for detecting a medium effect size at a significance criterion of α = .05, was N = 194 for linear regression analyses. We increased the sample size to cover for missing data.
Missing Data Handling
For PHQ15, PHQ9 and GAD and IPV CAS and resilience scores, there were very few participants (a maximum of 8 participants) with one or two missing items, so the partial raw score was used, which is the sum of the score of items that were answered. This is following the APA recommended procedure.
Results
Sample Characteristics
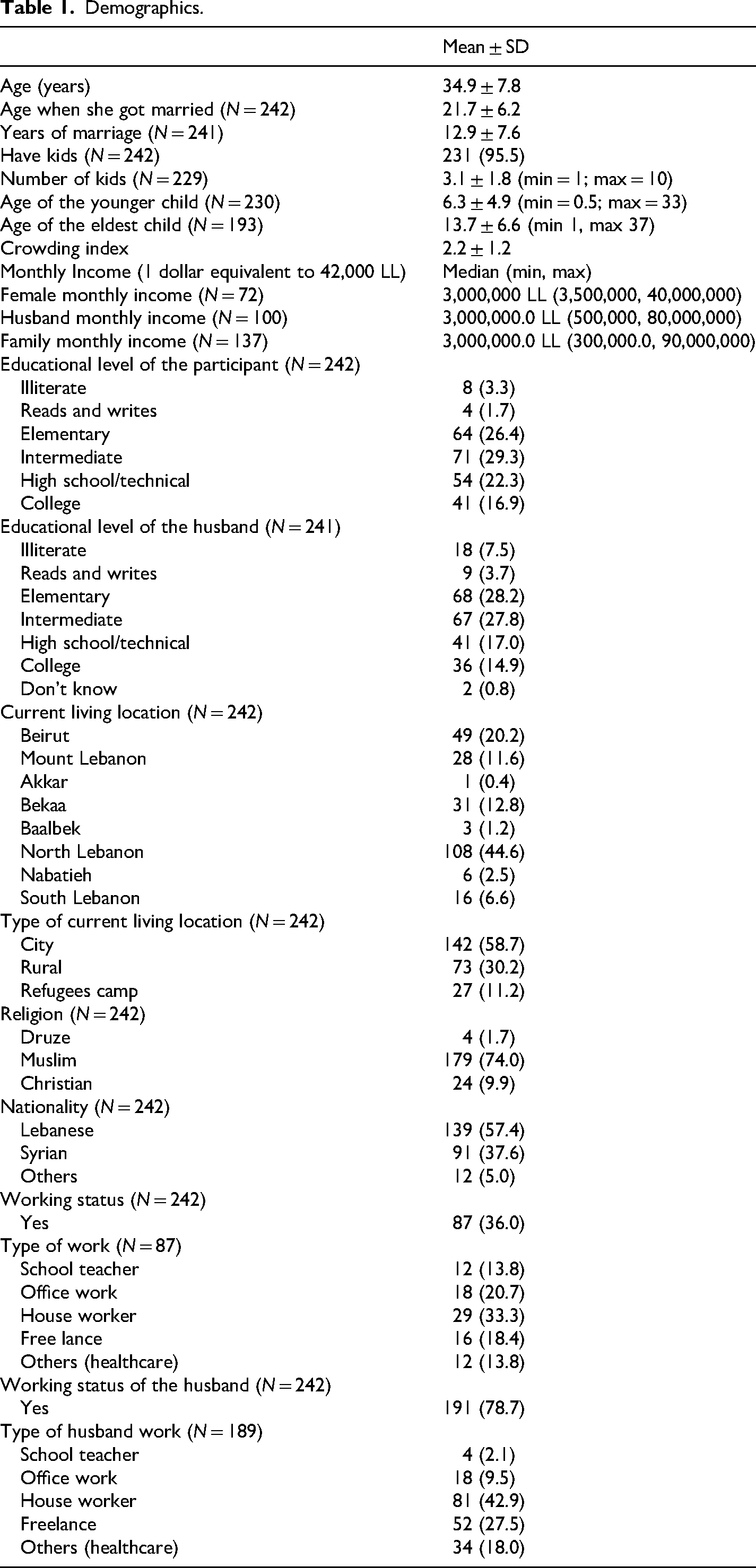
A total of 242 participants completed the survey. Table 1 shows the demographics. Participants were on average 34.9 ± 7.8 years old, had been married for 12.9 ± 7.6 years, and almost all had children (231, 95.5%). The family's median monthly income is 3,000,000 LL (72 USD); the minimum wage is 675,000 LL (17 USD). Most of the sample were Lebanese (139, 57.4%) or Syrian (91, 37.6%). Most husbands work (191. 78.7%), while only 36% (n = 87) of the participants work. More husbands reported smoking, alcohol consumption, and the presence of chronic disease), while more participants reported exercising (Table 2).
Demographics.
Health Status and Social Habits of the Participants and Their Husbands.
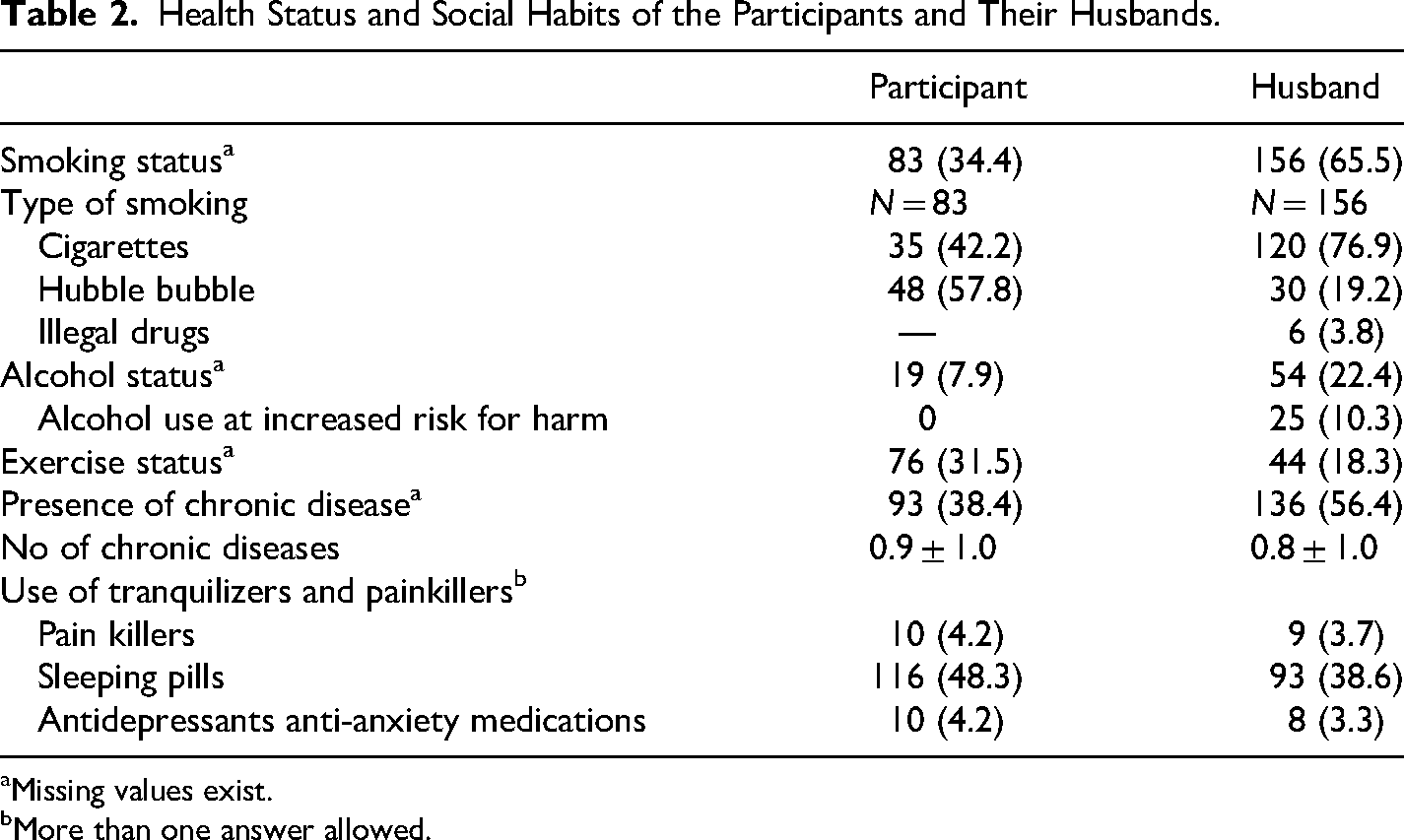
Missing values exist.
More than one answer allowed.
Health Status
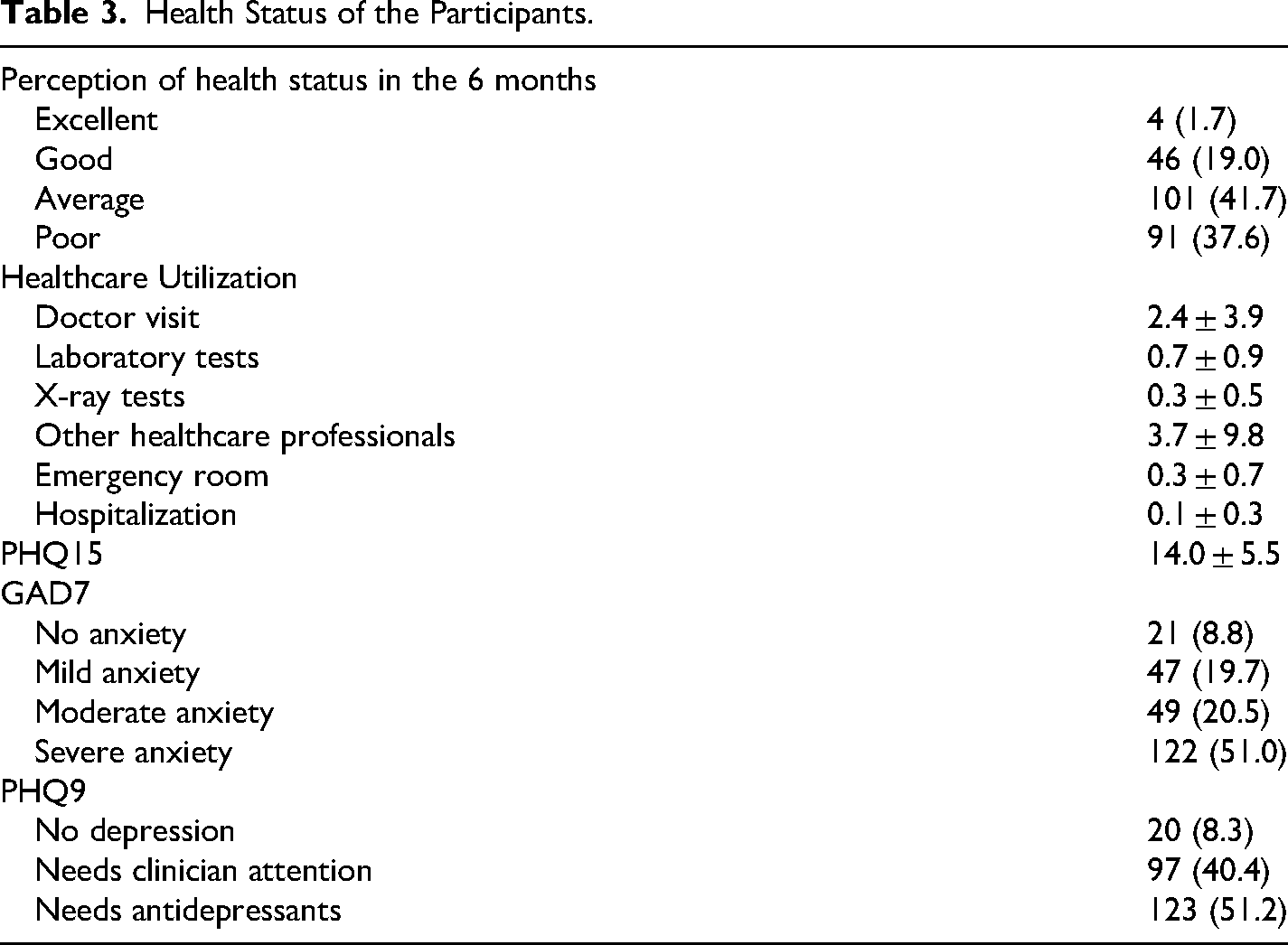
Most participants rated their health status as average to poor over the past 6 months (Table 3). On average, they have visited the doctor 2.4 ± 3.9 times and other health professionals such as the pharmacist or the nurse on average 3.7 ± 9.8 times. Nearly half of the participants reported suffering from severe anxiety or depression (Table 3). However, only 10 participants (4.2%) reported taking antidepressants or anti-anxiety medication, while 116 (48.3%) reported taking sleeping pills (Table 2).
Health Status of the Participants.
Social and Living Conditions of the Participants
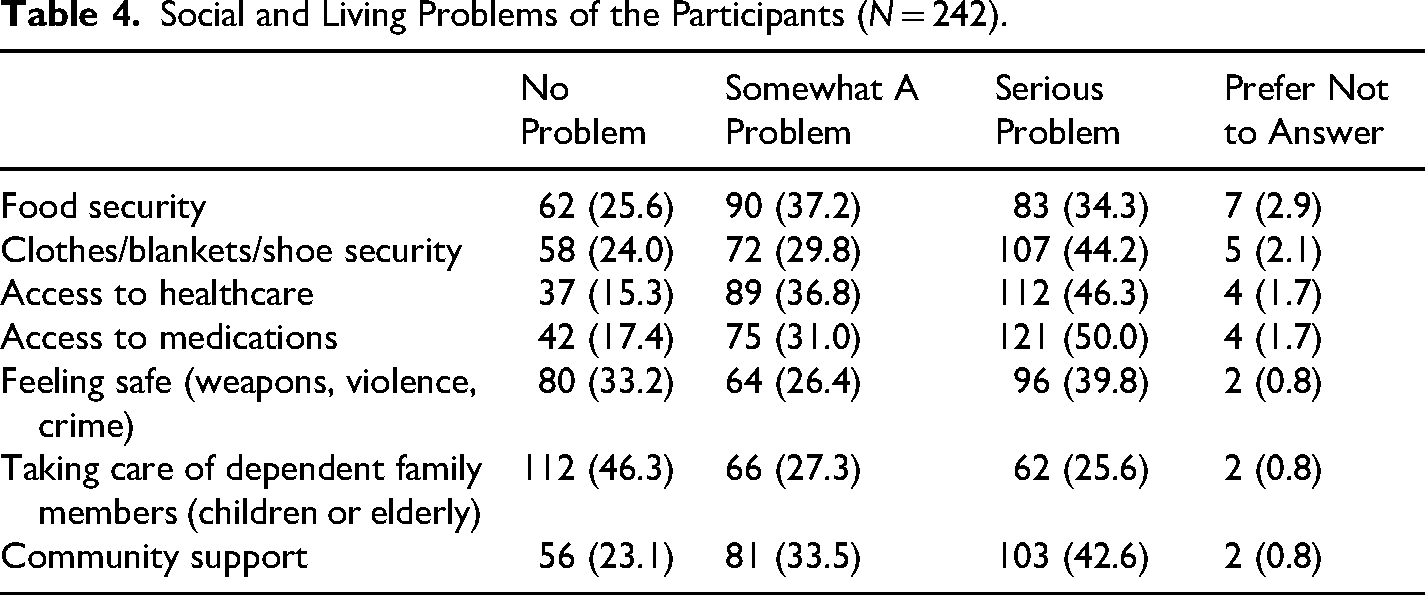
Thirty-four percent of the participants had serious problems with food security, 44% with clothes security, 46% had inaccessibility to health care, and 42% lack of community support (Table 4).
Social and Living Problems of the Participants (N = 242).
IPV, physical and mental health status, and resilience
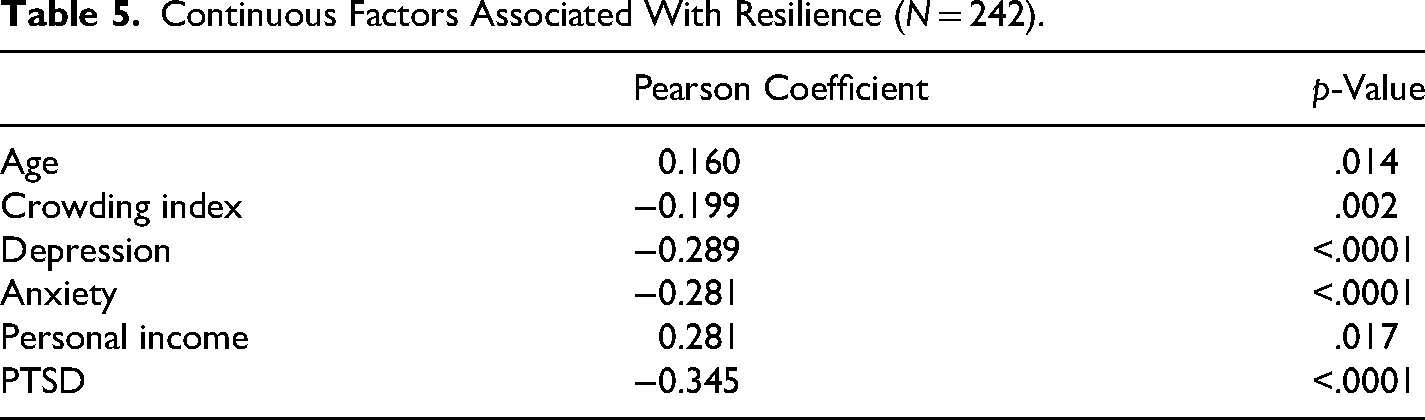
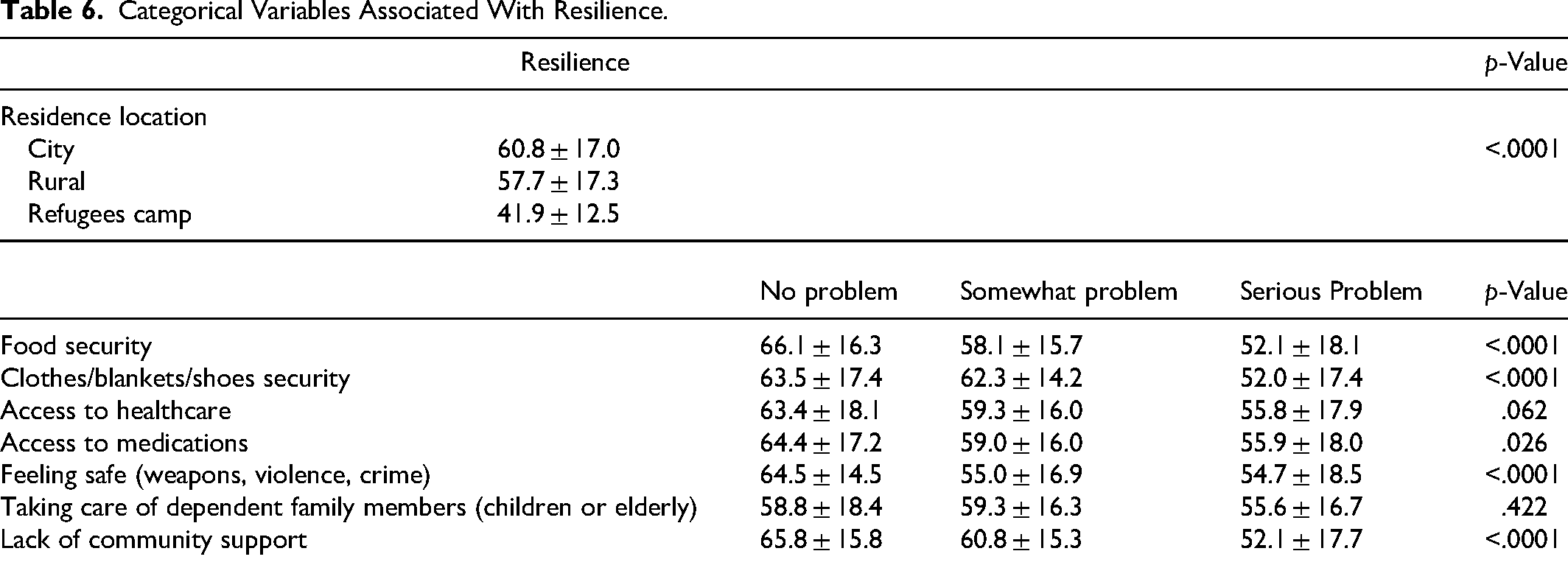
The participants scored 16.9 ± 3.8 on violence as measured by the CAS and 58.0 ± 17.5 on the CD-RISC 25 resilience scale. A bivariate analysis was conducted to determine the factors associated with resilience. There was a positive association between resilience and age, personal income, and place of residence (Tables 5 and 6). Resilience was negatively associated with crowding index, depression, anxiety, PHQ15, food and clothes insecurity, feeling safe, and community support.
Continuous Factors Associated With Resilience (N = 242).
Categorical Variables Associated With Resilience.
Mediator Effect of Resilience
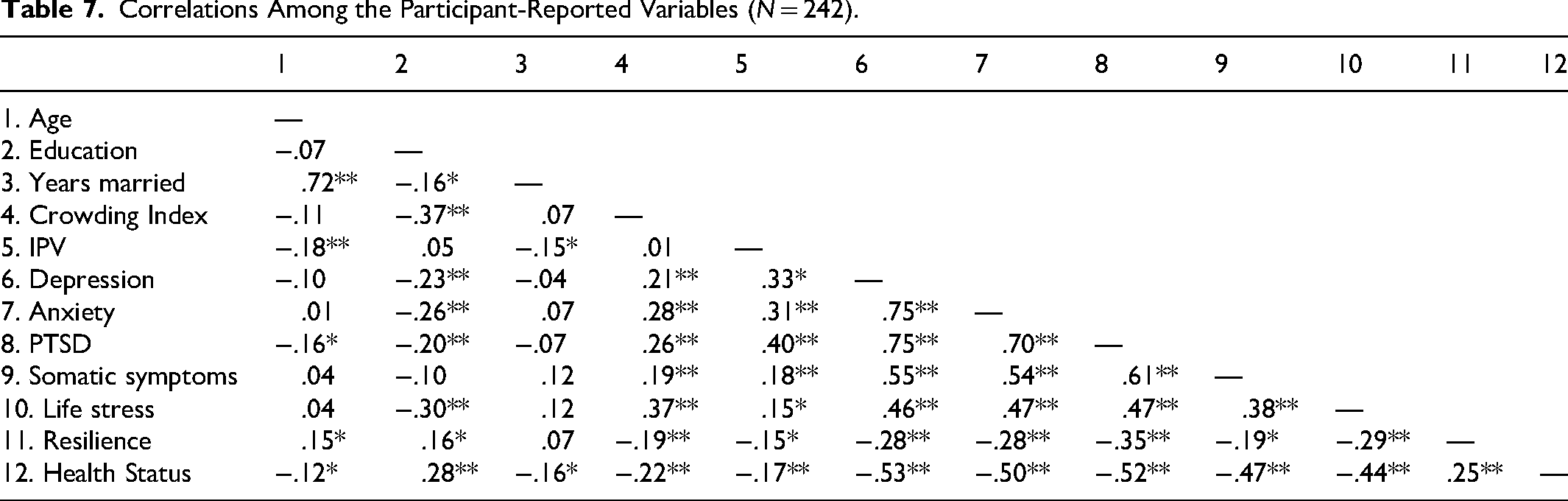
Regarding the mediator effect of resilience on the relationship between IPV (CAS) and physical health symptoms (PHQ15), a simple linear regression showed that IPV was a statistically significant predictor of health (B = −0.009, t = −2.632, p = .009). IPV was also statistically significant predictor of resilience (B = −.121, t = −2.391, p = .018). The mediator, resilience, emerged as a predictor of health (B = 0.011, t = 3.768, p < .0001). To examine whether resilience mediated the relationship between physical health symptoms (PHQ15) and IPV (CAS), a mediation analysis was performed using the traditional SOBEL and PROCESS macro for SPSS (Model 4; Hayes, 2022) with 5,000 bootstrap samples. Age, crowding, and current residence were included as covariates in the model. The direct effect of physical health symptoms on IPV remained significant (B = 0.36, p = .037). Regarding the indirect effect, the normal theory-based Sobel test indicated a statistically significant mediation relationship (Z = 2.14, p = .032). To examine whether resilience mediated the relation between IPV and mental health status, a linear regression was conducted with measures of PTSD, anxiety (GAD7), and depression (PHQ9). The results were not significant (Table 7).
Correlations Among the Participant-Reported Variables (N = 242).
Discussion
The current study explored the effect of resilience on the negative health outcomes of IPV exposure. It was hypothesized that resilience would mediate the effect of IPV on the mental wellbeing, health care utilization and physical outcomes of IPV survivors. The findings could pave the way for interventions to support women survivors of IPV in countries where IPV is not adequately addressed. In Lebanon, IPV remains an underestimated problem and has been largely ignored by the local authorities (Awwad et al., 2014). Despite the efforts taken by the Lebanese health care system to address the topic of IPV, it remains underprioritized (El Kak et al., 2025). There remains significant gaps in identifying and referring abused women, mostly because the recognition of an abusive pattern in women is often blurred by cultural and societal taboos (Usta et al., 2007), leaving survivors suffer in silence and use negative coping strategies to get them through their experiences with IPV (Usta et al., 2019).
A key strength of the present study lies in its identification of resilience as a statistical mediator between IPV and physical symptoms. While previous studies have explored the relationship between these variables, the present findings offer a more nuanced understanding that previous correlational approaches. This understanding can inform the development of more effective, resilience focused interventions. Previous research indicated a positive association between resilience and improved physical and mental health outcomes (Sánchez & Lopez-Zafra, 2019), hindering illness onset and promoting wellbeing (Babić et al., 2020). Given that resilience is a prevalent human response to trauma (Fenton, 2017), a “salutogenic” framework focusing on health-promoting factors rather than solely on disease-causing agents, may be particularly beneficial (Antonovsky, 1996). Promoting resilience may reduce feelings of helplessness, foster awareness of available resources and build new opportunities for growth, and thriving despite adversity (Gonzalez-Mendez & Hamby, 2020). Interventions designed to bolster resilience have been shown to decrease healthcare utilization (e.g., imaging, lab encounters, emergency department visits) (Stahl et al., 2015) and improve mental health symptoms, pain frequency, and physical symptoms such as headache and musculoskeletal pain (Gonzalez et al., 2019). Clinical interventions targeting prenatal mental health and relational resilience improved labor outcomes for IPV-exposed mothers (Scrafford et al., 2019). Understanding the complex interplay of factors associated with resilience is crucial for developing effective programs that can foster this protective capacity in IPV survivors.
The present study reveals a concerning pattern of compromised mental health among IPV survivors. A substantial proportion of the sample experienced significant challenges with anxiety, depression, and insomnia, evidenced by the prevalent use of sleep medication. Furthermore, the low rate of help-seeking behavior (4%) likely reflects both financial barriers to accessing mental health services, and the enduring stigma associated with mental illness. While resilience demonstrated a negative association with both depression and anxiety, its mediating role was not observed. This finding suggests that resilience may operate prophylactically, mitigating the impact of IPV (or other stressors) on psychological well-being prior to the development of clinically significant psychiatric disorders. This interpretation is consistent with Babic's findings regarding the inverse relationship between resilience and the incidence of mental health disorders such as PTSD (Babić et al., 2020). The advanced psychological symptomology observed in the current sample may have masked the identification of resilience as a mediator. Future research should investigate the specific mechanisms through which resilience confers its protective effects on survivor mental health. Such investigations might explore the interplay between resilience and factors such as specific coping mechanisms, social support structures, or underlying neurobiological processes.
A gap remains in the literature regarding factors that buffer the impact of IPV and strengthen resilience in IPV survivors (McNaughton Reyes et al., 2020). Our findings indicate a positive association between resilience and age, personal income, and a negative association with feeling safe, and community support. The negative association between conditions affecting their feeling of being safe, such as war or high crime, and an individual's resilience agree with the literature that found higher levels of trauma are linked to lower resilience capacity (Camargo et al., 2025; Danga et al., 2022). However, the negative association with community support was surprising. While prior research suggests that social support, life perspective shifts, and motivation to break the cycle of violence contribute to resilience and post-traumatic growth (Brosi et al., 2020) and that social support and other tertiary preventive interventions can mitigate long-term health and mental health consequences of IPV (Carlson et al., 2002), our findings present a more nuanced picture. The negative association with community support may be because women perceive IPV as lower level of trauma compared to the wars they were living through and hence manageable. It can also be explained by the stigmatizing response that IPV survivors often encounter in Lebanon when seeking help, including blame and pressure to remain in abusive relationship. Hence, older survivors with a lower personal income lacking community support may have developed self-reliance as a coping mechanism.
Resilience interventions should therefore incorporate strategies that foster self-reliance, such as self-affirmation techniques, which can reduce stress and rumination (Pandey et al., 2020). Self-care strategies, like breathing exercises and meditation, have been effective in promoting resilience across various conditions like HIV, headache and mental health, and cutaneous neural conditions (Gonzalez et al., 2019; Psaros et al., 2023; Vranceanu et al., 2014). While the results of this exploratory study showed that resilience statistically mediated the relation between IPV and health outcomes in a Middle Eastern population; yet it is limited by its small geographically restricted sample from organizations serving IPV survivors, limiting its generalizability. A wider, community-based sample would likely explore the prevalence of unreported IPV and further elucidate the mediating effect of resilience.
Conclusion
IPV is a major public health challenge in Lebanon where sociocultural norms often discourage disclosure and perpetuate a cycle of silent suffering. While previous research has established the importance of resilience, this study extends these findings by demonstrating its function as a mediator, thereby offering a more refined understanding of its impact on the health of IPV survivors. In communities where survivors are encouraged to remain silent, helping women develop or strengthen their resilience may protect their psychological and mental wellbeing and stay healthy till they decide to disclose the violence and seek help. Consequently, resilience focused interventions within these communities should prioritize the cultivation of self-reliance among women. These results are noteworthy and require additional exploration with larger community samples to explore those dynamics more comprehensively.
Footnotes
Ethical Considerations
Recruitment of participants from non-governmental organizations for participation in the study was approved by the UNFPA and the organizations.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The UNFPA has provided funds for the recruitment of participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.