
Abstract
This study examines associations between male- and female-perpetrated psychological, physical, and sexual intimate partner violence and child protective services involvement among Black women under community supervision in New York City (N = 247). Up to 72.1% of women experienced lifetime intimate partner violence (IPV) and 55.9% child protective services (CPS) involvement as parents. Women had significantly higher odds of CPS involvement if they experienced sexual IPV by male partners, multiple forms of IPV by male partners, or multiple forms of IPV by any partner (ORs: 1.8; 95% CIs: 1.1, 3.0; p < .05). Adjusted models lacked significance, suggesting further research and service needs.
Introduction
Community Supervision Programs and Black Women with Children in the US
Community supervision programs (CSPs), the largest segment of the corrections system in the US, include individuals living in their community while on probation or parole or in alternative-to-incarceration programs (Minton et al., 2021). Of those on probation, which constitutes the majority of people in CSPs, 19% identified as female and 21% as Black (Minton et al., 2021). Of those on parole, 11% identified as female and 32% as Black (Minton et al., 2021). Black individuals are 3.5 times more likely than non-Hispanic Whites to be under community supervision (PEW, 2018). The structural racism undergirding the criminal legal system has been traced to the history of slavery in the US followed by the era of Jim Crow, leading to a new system of social control, in which Black and Brown individuals are systematically stripped of legal and civic rights and their corresponding social and economic privileges (Alexander, 2010).
The intersection of race and sex identities further nuance individuals’ experiences in CSPs. Though men make up the majority of people in community supervision, the number of women in CSPs has been increasing in recent decades (PEW, 2018). The vast majority of women involved in the criminal legal system are raising children as single parents, are living in poverty, and face additional challenges caring for their children while being punished for offenses related to economic and social inequalities (Cowan, 2019). Challenges may be compounded by heightened surveillance of their activities, restrictions on movement, and fears of violating the CSP's terms, which could yield added penalties, including incarceration (Schlafer et al., 2023). These penalties can stress the parent–child relationship and lead to physical separation. Further, many women in the criminal legal system have histories of trauma (including from intimate partner violence, or IPV) and struggle with mental illness and/or substance use (Vera Institute of Justice, 2016). Despite these needs and inequalities, women in the criminal legal system face barriers to essential health and psychosocial services. Wu et al. (2012) reported an average of three barriers to services among individuals in CSPs, highlighting a need for concurrent services to address areas such as mental health, food insecurity, and limited social support.
Intimate Partner Violence and Its Impacts
IPV is a pattern of coercive, controlling behaviors by an intimate partner and can include physical, sexual, psychological or emotional, economic, and other forms of abuse (NYC, 2021). According to 2015 data from the National Intimate Partner and Sexual Violence Survey (NISVS), 1 in 4 women and 1 in 10 men reported experiencing sexual violence, physical violence, and/or stalking by an intimate partner (Smith et al., 2018). Black women experience particularly high rates of IPV, with over half of Black women in the US reporting physical, sexual, and/or stalking violence by an intimate partner (Leemis et al., 2022). Furthermore, Black women are less likely to access services voluntarily due to cultural insensitivity of existing services, greater likelihood of losing custody of their children to child protective services (CPS), and greater likelihood of being arrested or charged with crimes (Bent-Goodley, 2005, 2009). Extant research primarily focuses on IPV perpetrated by male partners or does not specify the sex of the perpetrating partner.
Intersections of Child Protective Services, Criminal Legal Systems, and Intimate Partner Violence
In 2019, CPS agencies throughout the US received approximately 4.4 million referrals, mostly from law enforcement, education, and medical personnel, of alleged child maltreatment for roughly 7.9 million children (U.S. DHHS, 2021). Research has shown a roughly 40% (or more) overlap between exposure to IPV and direct child maltreatment, suggesting that a large percentage of CPS cases involve IPV (Appel & Holden, 1998; Herrenkohl et al., 2008). Existing literature commonly treats children's exposure to IPV as a unitary construct without differentiating by number of exposures and type of IPV, despite evidence that physical, sexual, psychological, and other forms of IPV may impact children differently and warrant different interventions (Gonzalez et al., 2020). Furthermore, CPS has a documented history of punishing mothers for IPV perpetrated against them by male partners through “failure to protect” policies, rather than partnering with mothers to promote the safety and well-being of them and their children (Victor et al., 2019). A woman experiencing IPV may be deemed un-protective of her children for not leaving a partner perpetrating violence, reflecting a CPS belief that the woman's only safe choice is to leave. If the woman does not leave the relationship, CPS may deem her to be making an unsafe parenting choice and may increase its interventions with the family, even removing children from her custody (Cannon et al., 2020; Hughes & Chau, 2012).
CPS systems (e.g., Administration for Children Services [ACS] in New York City) are more likely to engage and intervene in families involved in the criminal legal system (Fedock et al., 2018; Phillips & Dettlaff, 2009). Women who have children and who are in the criminal legal system are more likely to experience violence such as IPV, which further increases their likelihood of CPS involvement as parents, compared to women who have children and are not in the criminal legal system (Alaggia et al., 2012; Fedock et al., 2018; Fong, 2017; Mirick, 2014). Evidence suggests that criminalization has failed to decrease IPV, while having had severe consequences, especially among Black women (Goodmark, 2021; Kajeepeta et al., 2024). Criminal legal systems punish women for physically defending themselves and their children from the violence, labeling them as “bad victims” (i.e., undeserving of systems’ protection and support in ways the women themselves define as supportive), and even remove children from their custody as a result (Goodmark, 2021; Kajeepeta et al., 2024). This relationship may be greater among parents living in poverty, who often have to rely on more volatile interpersonal relationships for support and on service systems more likely to report them to CPS (Fong, 2017). Again, these associations primarily focus on physical IPV, as perpetrated by male partners, and do not center the unique risks and experiences of women under community supervision (Casanueva et al., 2014; Gurusami, 2019; Macy et al., 2012).
Studies have repeatedly confirmed the disproportionate representation of Black women in both CPS and criminal legal systems, rooted in the separation of Black families under legalized slavery, vagrancy laws, racialized drug laws and policing, and mass incarceration of Black and Brown people (Alexander, 2010; American Bar Association, 2022; Dettlaff & Boyd, 2020; Harp & Bunting, 2020; Mirick, 2014). In the state of New York, African-American children were identified as victims of maltreatment at a rate of 31.7 per 1,000 African-American children in the population, which is nearly three times higher than the rate of 11.6 per 1,000 found among non-Hispanic White children in the population (U.S. DHHS, 2021). Harp and Bunting (2020) argue that multiple racist structures lead to the overrepresentation of Black mothers and families involved with CPS, such as through the so-called “crack babies” epidemic in the 1980s, in which Black parents were vilified as unfit parents due to specific drug use and inadequate healthcare access; meanwhile, White mothers using alcohol or opioids during and after pregnancy were less frequently reported to CPS, less vilified in the media, and less likely to lose custody of their children. Over-surveillance by CPS and criminal legal systems has been identified as a form of poverty and reproductive governance over Black families in poverty and neighborhoods in poverty (Fong, 2019, 2020; Harp & Bunting, 2020; Merritt, 2020). That the majority of CPS cases are classified as “neglect” reinforces the conflation of child maltreatment and the real effects of poverty on families, also contributing to the racialization of the family policing system (Merritt, 2020; Roberts, 2001).
Ideally, CPS and other systems would respond with services and interventions to help address families’ specific needs in ways that are protective and empowering; however, services and interventions often are imposed upon women and children, are unavailable or inaccessible (especially to families in which one or more parents are involved in the criminal legal system), or present additional risks to women and children (Amiri et al., 2020; Fong, 2019; Liang et al., 2005; Wu et al., 2012). Black women, in particular, may choose not to seek formal help to avoid racial discrimination from service providers and systems (Waller et al., 2022). Mirick (2014) found that identifying as Black, Latinx, or biracial, using (unspecified) substances, and having experienced IPV each increased levels of mistrust on the part of parents involved with CPS, which affected their ability to engage with CPS officials. Further, Kajeepeta et al. (2024) found that Black families in predominantly White counties may have an even higher risk of family surveillance due to the interactive nature of IPV policing and family surveillance systems, which would further erodes trust in these systems. As such, many women who have experienced IPV as victims have reported greater satisfaction with informal support (e.g., family, friends, and neighbors) than with formal service systems (Tan et al., 1995). Still, Panchanadeswaran et al. (2008) found that women in methadone maintenance treatment who were experiencing IPV perceived themselves to have low levels of social support, thus suggesting a useful point of intervention.
Aims and Conceptual Framework
This paper examines the relationship between IPV and CPS involvement as parents among Black women who have used drugs and are in CSPs in New York City.
Aim 1 is to estimate the prevalence of IPV and CPS experiences among Black women who have used drugs and who ever had children and who are in CSPs. Aim 2 is to test hypothesized associations between IPV (psychological, physical, and/or sexual) and lifetime CPS involvement among Black women who have used drugs and who ever had children and who are in CSPs.
We hypothesize that Black women in the study who ever experienced psychological, physical, and/or sexual IPV by any partner (male and/or female) would have higher odds of being involved with CPS than Black women in the study who never experienced IPV. This paper relies on ecological theory to frame the relationship between Black women's experiences with IPV and CPS in the context of CSPs (Bronfenbrenner, 1977; Few, 2007).
Through the lens of ecological theory, IPV is an interpersonal risk factor at the microsystemic level for exosystemic CPS engagement in this specific population of Black women who have used drugs, have children, and are in CSPs (see Figure 1). Individual women's experiences across multiple systems can be contextualized at each ecological level (e.g., as uniquely embodying the needs of women with children in CSPs in a society in which Black women are disproportionately represented in these systems). Drawing from the literature presented above, potential (not definitive or causal) pathways for the hypothesized relationship are presented below.
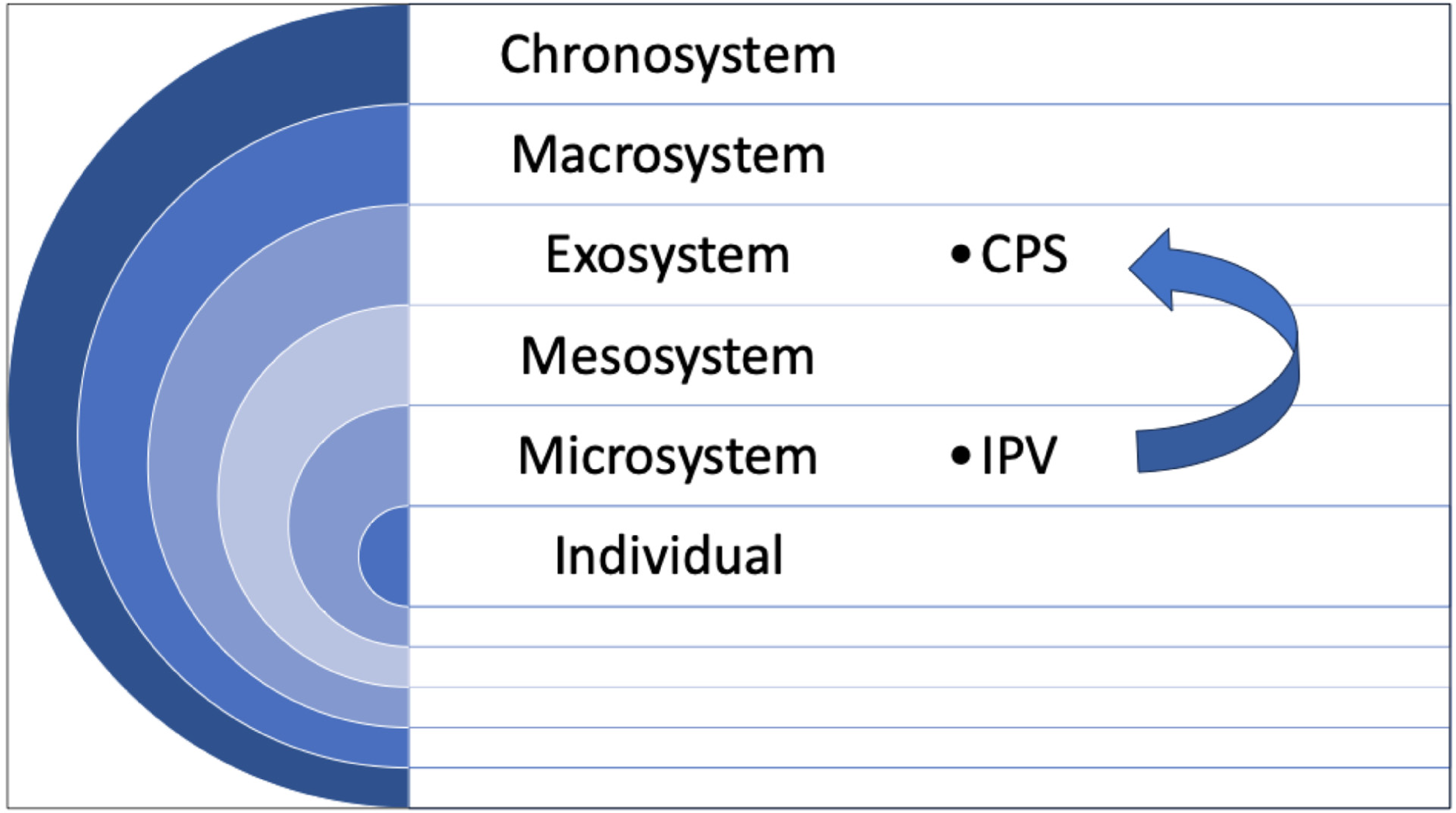
Conceptual framework.
Individual
Women involved in the criminal legal system are more likely to experience violence (Fedock et al., 2018). That violence may exhaust their internal resources and overwhelm their capacity to manage child safety and/or system involvement (Thompson & Whimper, 2010).
Microsystem
Intimate partners and children exist at the level of the microsystem. Intimate partners perpetrating IPV may directly maltreat children (Appel & Holden, 1998; Herrenkohl et al., 2008). Indirectly, IPV may decrease the time and attention that women experiencing IPV are able to devote to caring for their children (Thompson & Whimper, 2010).
Mesosystem
The mesosystem acts as a conduit for the relationship between individual women's experiences of IPV at the microsystemic level and involvement with CPS at the exosystemic level. Direct maltreatment of children and/or the interference of the violence in women's ability to care for their children can increase risk to children, leading to CPS involvement (Thompson & Whimper, 2010).
Exosystem
CPS and CSPs are both formal service systems that increase the likelihood of engagement with other formal service systems, such as when a CSP/probation/parole officer visits the home and makes a report to CPS. In how they respond, CPS systems may flag IPV as a case of “failure to protect” or neglect by women experiencing IPV (Victor et al., 2019). CPS may also flag IPV as direct child maltreatment by individuals perpetrating IPV.
Macrosystem
Beliefs about “fit” versus “unfit” parenting tie into “failure-to-protect” decisions in the context of IPV (Cannon et al., 2020; Harp & Bunting, 2020; Hughes & Chau, 2012). CSPs and CPS systems act as forms of poverty governance and family surveillance, especially over Black and Brown families (Fong, 2019, 2020; Harp & Bunting, 2020; Merritt, 2020).
Chronosystem
Sociohistorical conditions link CSPs and CPS systems through policing of Black and Brown bodies/families by formal systems, including through the criminalization of family violence (Goodmark, 2021; Harp & Bunting, 2020).
Thus, ecological theory is a dynamic framework underscoring not only human experiences at each level of ecology, but also the dynamics across levels—in this case, individual Black women's experiences with IPV (at the microsystemic level) and systemic racism (at the exosystemic and macrosystemic levels), as connected through the mesosystem.
Methods
Design, Sampling, and Participants
This is a secondary analysis using baseline (pre-intervention) data from the E-WORTH (Empowering African-American Women on the Road to Health) randomized clinical trial that tested the effectiveness of a multimedia HIV/STI and IPV prevention intervention among Black women in CSPs in New York City who have used drugs (N = 352). (See previous publications for greater detail about E-WORTH [e.g., Johnson et al., 2018], clinical trials number NCT02391233. See also Johnson et al., 2023, for a syndemic and holistic perspective from the WORTH intervention study.) Between 2015 and 2018, researchers used convenience and voluntary response sampling to recruit women from community-based and corrections organizations by directly speaking to clients, posting flyers, distributing referral vouchers, and conducting group presentations at recruitment sites in Manhattan and Queens (Johnson et al., 2018). Research assistants conducted screening and informed consent procedures, and women were compensated for participation. Women were included in the study if they met the following inclusion criteria: were assigned female sex at birth; were at least 18 years of age; identified as African-American or Black; were English-speaking; if pregnant, were less than 7 months along; have had any biological or adopted children (for this paper's analyses); had an address to receive mail; and were living in any of NYC's five boroughs (N = 247). The women had to have been under community supervision (e.g., probation, parole) in the past 90 days and had to have reported illicit drug use, binge drinking, and/or alcohol or drug treatment in the past 6 months. Women also had to have engaged in risky sexual behavior (e.g., engaging in unprotected sex with a male partner in the past 90 days). For more expansive details about the parent study's inclusion criteria, see Johnson et al. (2018).
Measurement
Baseline assessment data were collected via audio computer-assisted self-interviews.
Dependent Variable: Child Protective Services Involvement as Parents
The dependent variable was measured by the question, “Have you ever had an open or active case with the Administration for Children Services (ACS)?” (i.e., the name of the CPS system in New York City). Responses were dichotomized as yes or no.
Independent Variables: Ever Experienced Intimate Partner Violence
We used shortened forms of two scales to measure any lifetime experiences of psychological, physical, sexual, and all IPV victimization (i.e., psychological, physical, and sexual) by male and/or female partners. The Revised Conflict Tactics Scale (CTS2) has demonstrated reliability and internal consistency (alpha = 0.86 for physical violence, alpha = 0.87 for sexual coercion) in its use with multiple populations over decades of research (Straus et al., 1996). The Psychological Maltreatment of Women Inventory, with internal consistency previously found to be alpha = 0.88, was combined with questions on the short-form CTS2 to measure psychological abuse (Tolman, 1999). For more details about the use of these tools in the E-WORTH parent study, see Gilbert et al. (2022).
Sociodemographic Characteristics and Covariates
Dichotomous and continuous descriptive variables represented the presence and number of children of each woman included in the analysis. Women with CPS involvement as parents were asked to answer yes or no to indicate if they had ever been treated unfairly by CPS officials. Women were also asked to indicate if, at the time of survey, they had any children in the foster care system and, if so, how many. Women's Hispanic/Latina ethnicity was represented as a binary yes/no descriptive variable.
A dichotomous question about food (in)security served as a proxy for families’ economic hardship, as in previous studies (Maguire-Jack et al., 2022; Rodriguez-Jenkins & Marcenko, 2014), as follows: “In the past 3 months, have you always had enough money to buy food?” “Ever had mental health diagnoses/suicidal ideation” was dichotomized as yes/no, with yes indicating a yes response to ever having experienced depression, anxiety, PTSD, bipolar disorder, schizophrenia, or suicidal ideation.
The following questions from the ENRICHD Social Support Instrument (Mitchell et al., 2003) were used, continuously scored from 3 to 15: (1) Is there someone who you can talk with if you are experiencing conflict or relationship problems with your partner? (2) Is there someone who you can stay with overnight if you need a place in an emergency? (3) Is there someone who you can talk to if you are concerned that you are having challenges negotiating safe sex with your partner? Responses ranged from none of the time (1) to all of the time (5).
Data Analysis
We used SPSS version 28 to conduct analyses. We used univariate statistics (i.e., frequency distributions, measures of central tendency, and standard deviations) to present the prevalence of IPV and CPS involvement in the sample (Aim 1) and for all variables. We relied on bivariate statistical tests (t-tests and chi-square tests) to explore basic associations between the dependent variable and independent variables and covariates.
To test the study hypothesis, related to associations between IPV and CPS involvement in the sample (Aim 2), we used logistic regression models, reporting on unadjusted and adjusted odds ratios with confidence intervals at 95%. Covariate adjustments included age, food insecurity (as a proxy for low economic resources), history of mental health diagnoses and/or suicide attempt, and social support. Extant literature has found these variables to be associated with involvement in both CPS and criminal legal systems and may, therefore, act as confounders in our models (Gurusami, 2019; Harp & Bunting, 2020; Herrenkohl et al., 2008). We further ran modified Poisson regression models (see Zou, 2004), calculating risk ratios as sensitivity analyses.
Human Subjects
The parent study, Project E-WORTH, received approval from the Columbia University IRB (protocol number AAAN8409).
Results
Sample Characteristics
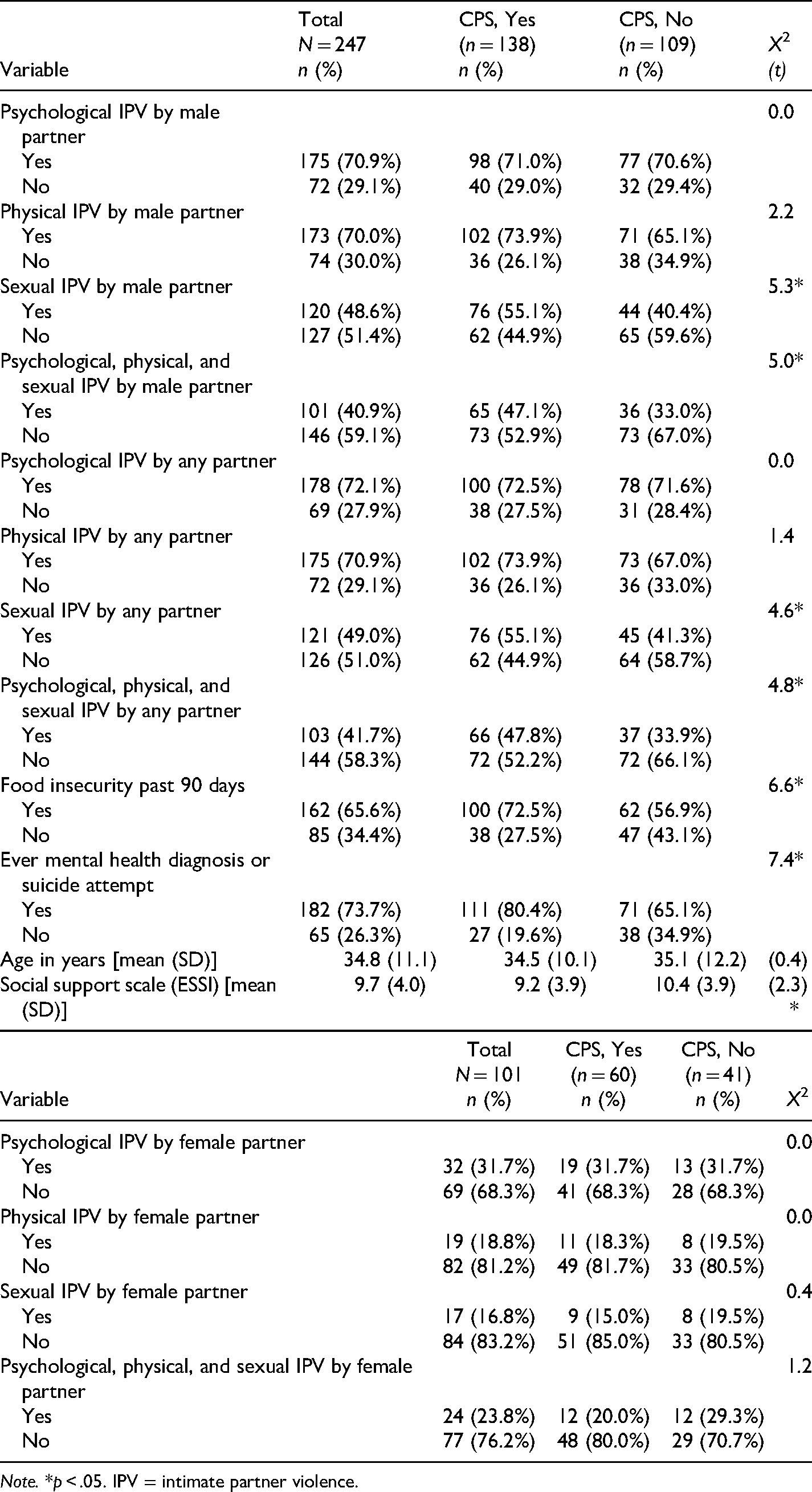
Male-perpetrated and male-or-female-perpetrated IPV questions yielded a sample size of 247 (in this paper's analyses), whereas female-perpetrated IPV questions yielded a sample size of 101. Table 1 presents characteristics of women in the sample. The sample included 247 Black-identifying women with a mean age of 34.8 years (SD: 11.1, range: 19–68). Almost two-thirds of women (n = 162, 65.6%) reported experiencing food insecurity. Nearly three-quarters (n = 182, 73.7%) reported ever having received a mental health diagnosis and/or ever having made a suicide attempt. On a three-item version of the ESSI, with a range of 3 to 15, in which higher scores reflect higher levels of social support, the mean score was 9.7 (4.0, 3–15). All women in the study had histories of using drugs or engaging in binge drinking. Around two-thirds (n = 167, 67.6%) had ever engaged in binge drinking and/or marijuana/hashish (n = 171, 69.2%). About one-third of women had used crack, cocaine, or heroin (n = 86, 34.8%) and/or other drugs (n = 74, 30.0%).
Sample Characteristics (N = 247).
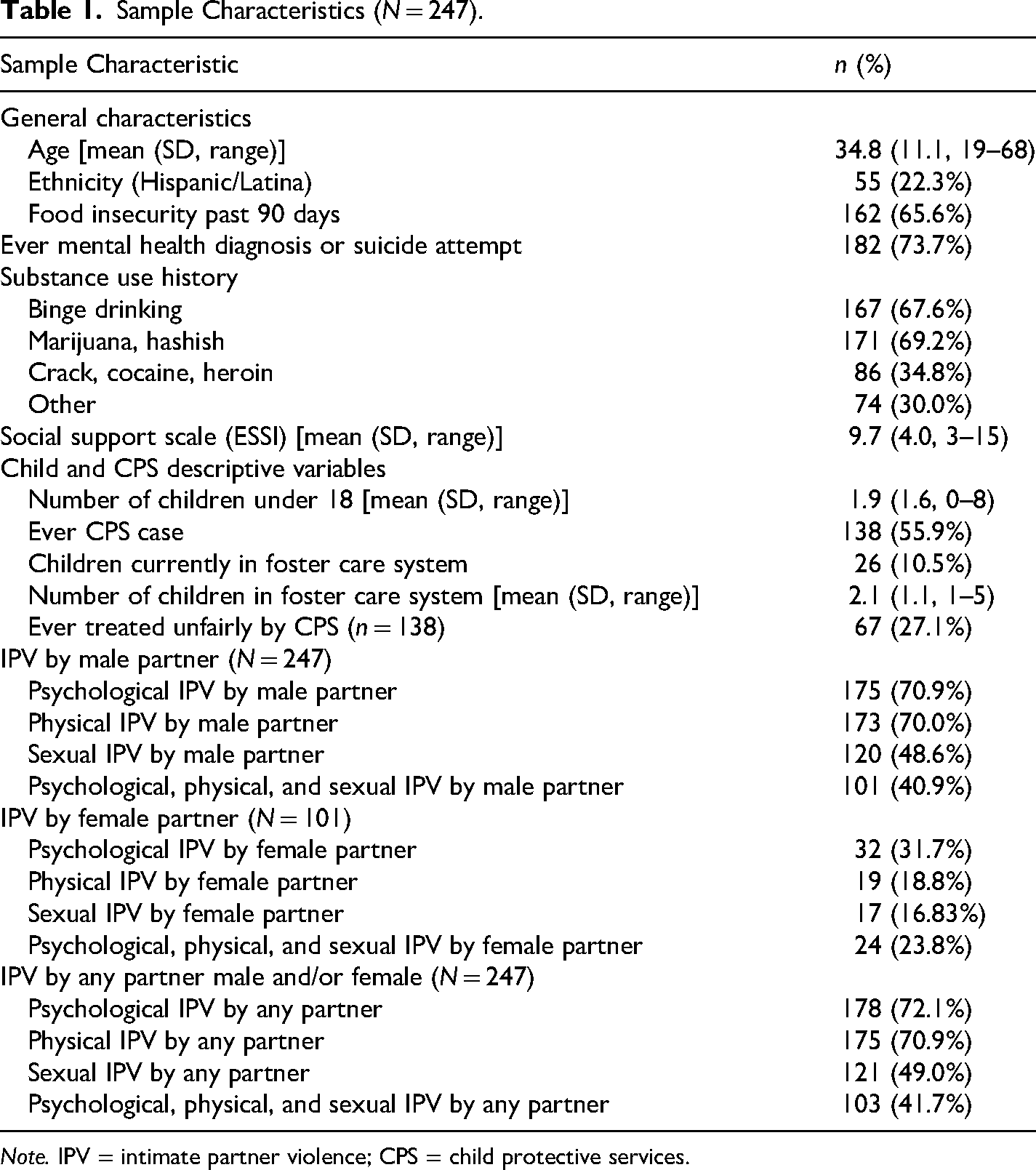
Note. IPV = intimate partner violence; CPS = child protective services.
Child Protective Services Involvement
Women reported having a mean of 1.9 (1.6) children under the age of 18 years old, with a range of 0 to 8 children under 18. Of women with children of any age, over half (n = 138, 55.9%) reported ever, as parents, having had an open or active case with CPS. The large majority of women (n = 221, 89.5%) did not currently have children in the foster care system. The mean number of children in foster care was 2.1 (1.1, 1–5). Of women with CPS cases, nearly one-third (n = 67, 27.1%) reported having been treated unfairly by CPS.
Intimate Partner Violence
A substantial percent of women reported ever experiencing psychological IPV (n = 175, 70.9%) or physical IPV (n = 173, 70.0%) by a male partner. Nearly half of women (n = 120, 48.6%) reported experiencing sexual IPV by a male partner. Psychological, physical, and sexual IPV by male partners were reported by 40.9% of women (n = 101).
Of the 101 women who reported having had female partners, approximately one-third reported psychological IPV (n = 32, 31.7%) and nearly one-fifth reported physical IPV (n = 19, 18.8%). Only 17 women (16.83%) reported sexual IPV by a female partner, and nearly one-quarter of women (n = 24, 23.8%) reported all three forms of IPV—psychological, physical, and sexual—by female partners.
Nearly three-quarters of women reported psychological IPV (n = 178, 72.1%) and/or physical IPV (n = 175, 70.9%), respectively, by any partner regardless of the partner's sex. Almost half of women (n = 121, 49.0%) reported sexual IPV by any partner, and 41.7% of women (n = 103) reported psychological, physical, and sexual IPV by any partner.
Associations with Child Protective Services Involvement
Table 2 displays model variables and their associations with CPS involvement. (See Appendix Table A for all associations, including covariates.) Results from Pearson's chi-square of the independent variables (i.e., types of IPV) and the outcome variable (i.e., CPS involvement) revealed that women who had experienced sexual IPV were significantly more likely than women who had not experienced sexual IPV to be involved with CPS as parents, X2 = 4.6, p < .05. Women who experienced all three forms of IPV (i.e., psychological, physical, and sexual) were also significantly more likely than women who had not experienced all three forms of IPV to be involved with CPS, X2 = 4.8, p < .05. Similar results were found for women who had experienced male-perpetrated sexual IPV (X2 = 5.3, p < .05) and multiple forms of male-perpetrated IPV (X2 = 5.0, p < .05), respectively. Pearson's chi-square results were not significant for psychological IPV, physical IPV, or any IPV perpetrated by female partners and CPS involvement.
Associations with Child Protective Services (CPS) Involvement (N = 247).
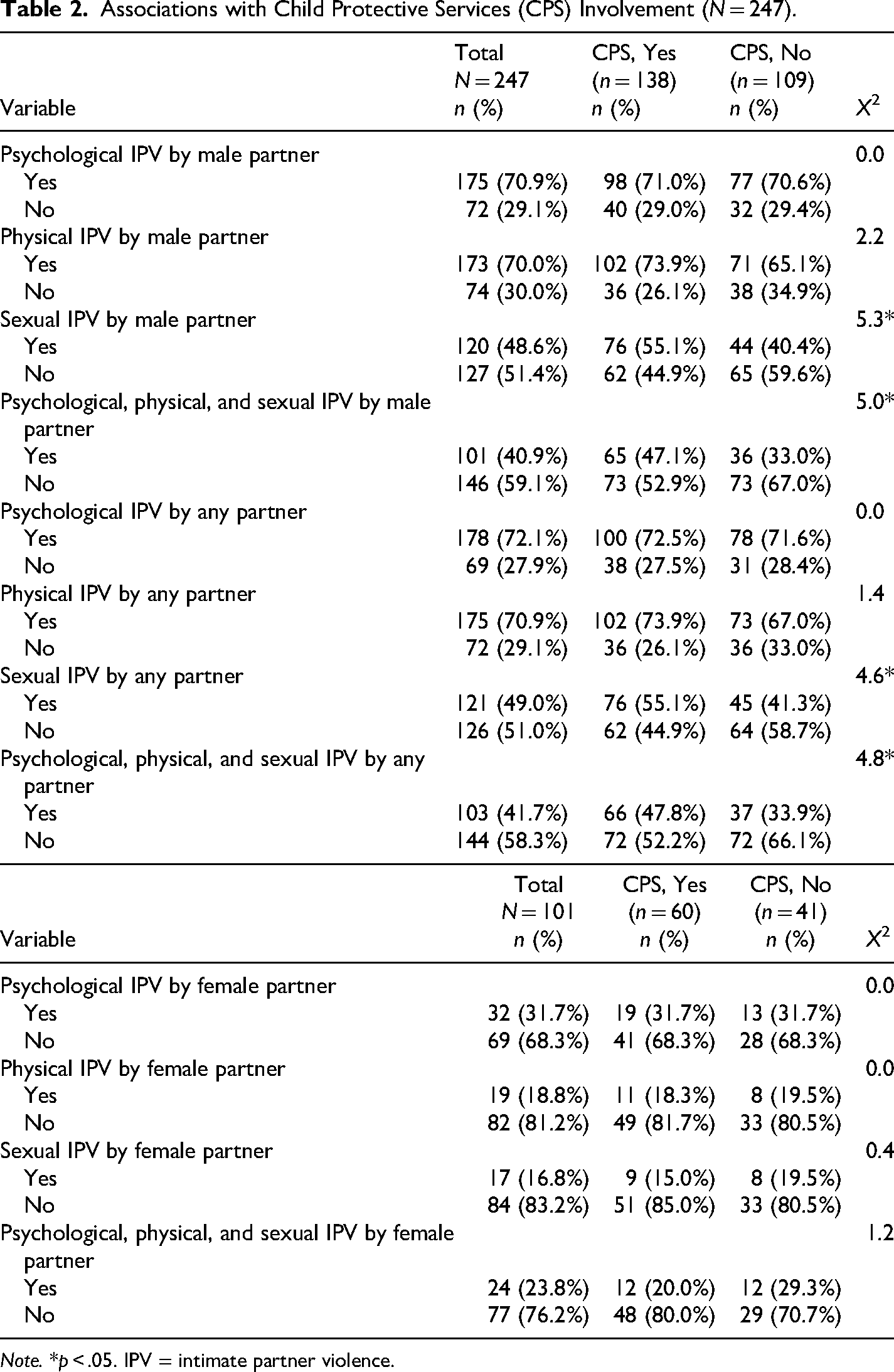
Note. *p < .05. IPV = intimate partner violence.
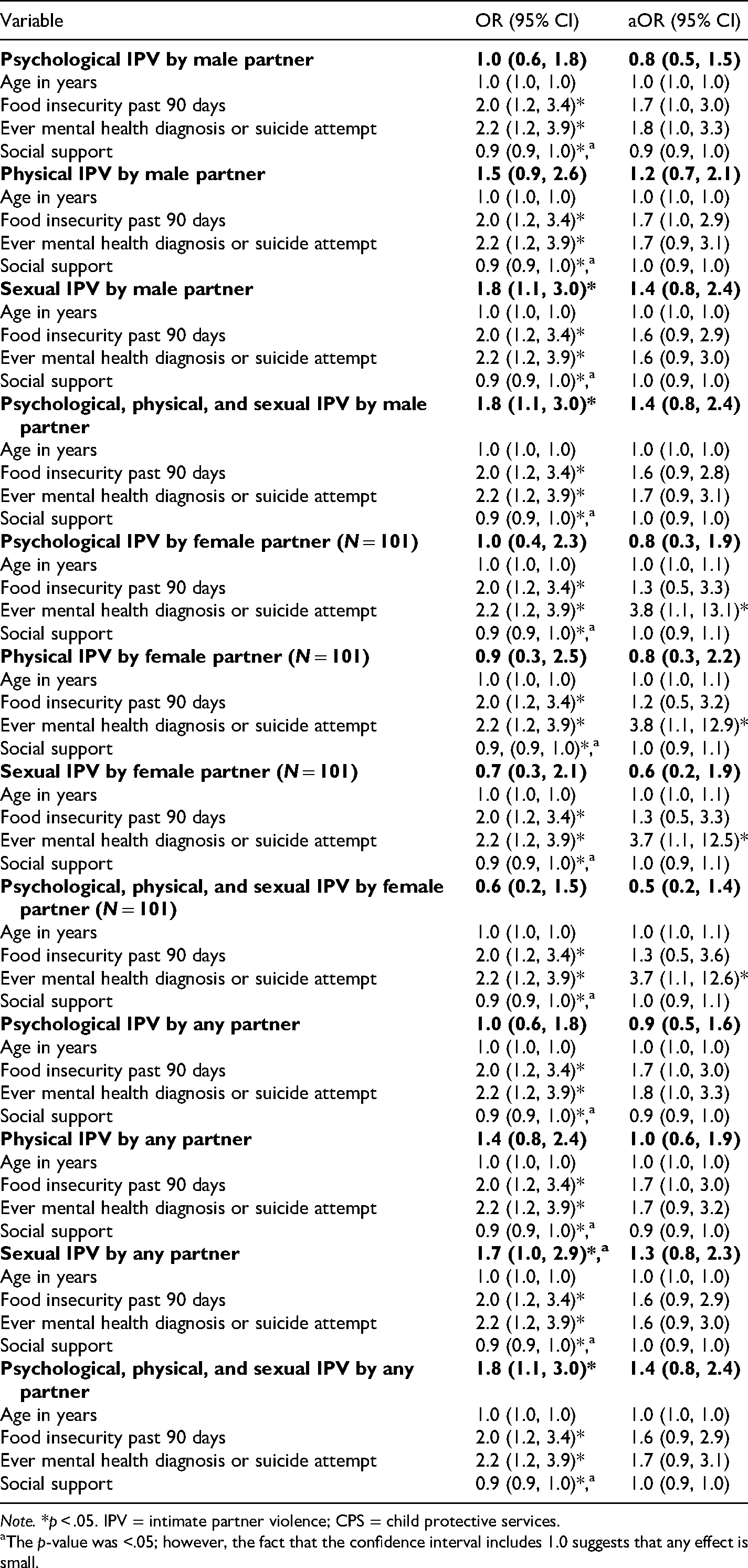
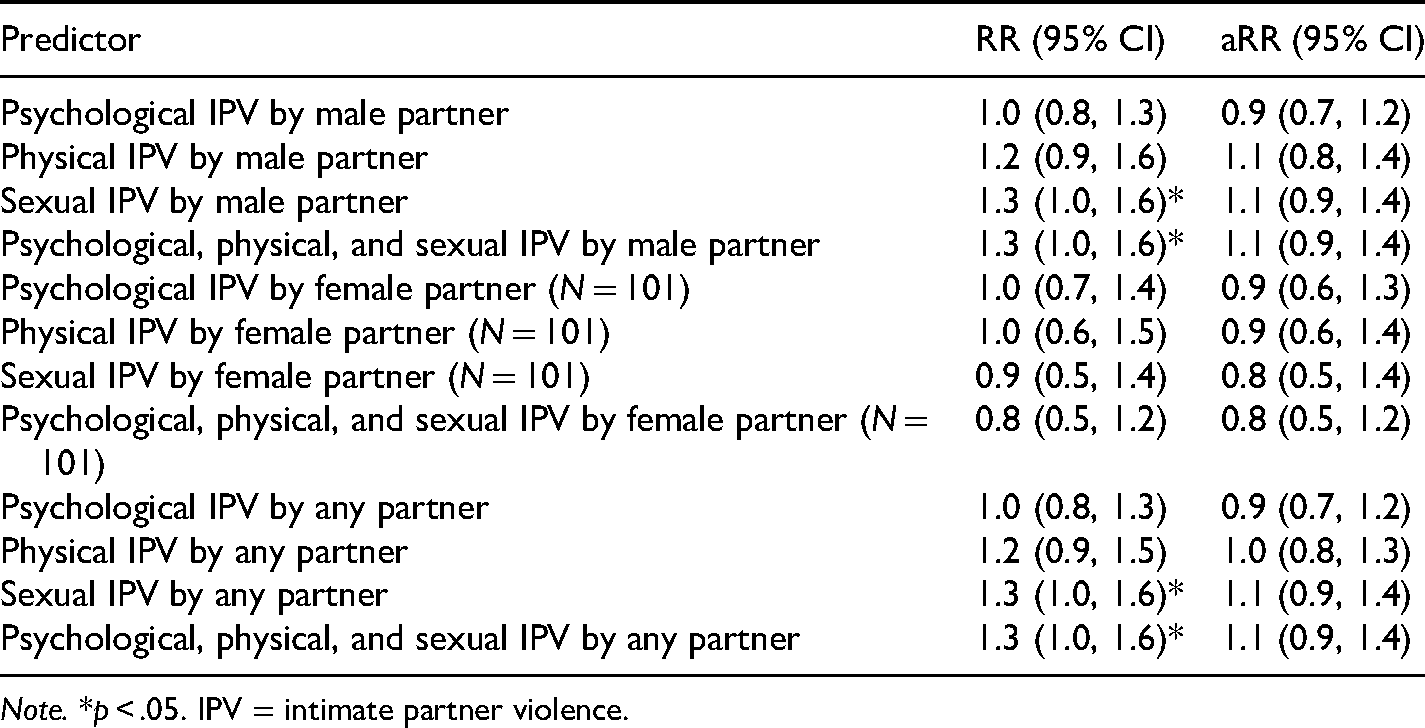
Table 3 presents results from logistic regression models, which further tested the hypothesis that experiences of psychological, physical, and/or sexual IPV would be significantly associated with CPS involvement. (See Appendix Table B for complete regression results that include unadjusted odds ratios for covariates.) In the unadjusted regression models, experiencing all forms of IPV by any partner was significantly associated with CPS involvement (OR: 1.8; 95% CI: 1.1, 3.0, p < .05). Results were similar for sexual IPV and multiple forms of IPV perpetrated by males only (OR: 1.8; 95% CI: 1.1, 3.0 and OR: 1.8; 95% CI: 1.1, 3.0, p < .05, respectively). These associations did not persist in female-perpetrated-only IPV models or in adjusted models, which controlled for age, food insecurity in the past 90 days, mental health history (ever received a diagnosis of depression, anxiety, PTSD, bipolar disorder, schizophrenia, or suicidal ideation), and social support. We were unable to reject the null hypothesis for the association between IPV and CPS in any of the adjusted models, regardless of the sex of the partner who perpetrated the violence. However, odds ratios for mental health history remained significant in adjusted models for female-perpetrated psychological IPV (aOR: 3.8; 95% CI: 1.1, 13.1; p < .05), female-perpetrated physical IPV (aOR: 3.8; 95% CI: 1.1, 12.9; p < .05), female-perpetrated sexual IPV (aOR: 3.7; 95% CI: 1.1, 12.5; p < .05), and female-perpetrated psychological, physical, and sexual IPV (aOR: 3.7; 95% CI: 1.1, 12.6; p < .05). See Appendix Table C for risk ratios resulting from modified Poisson regression models as sensitivity analyses.
Odds Ratios and Risk Ratios from Logistic Regression Analyses Estimating the Associations Between IPV and CPS Involvement (N = 247).
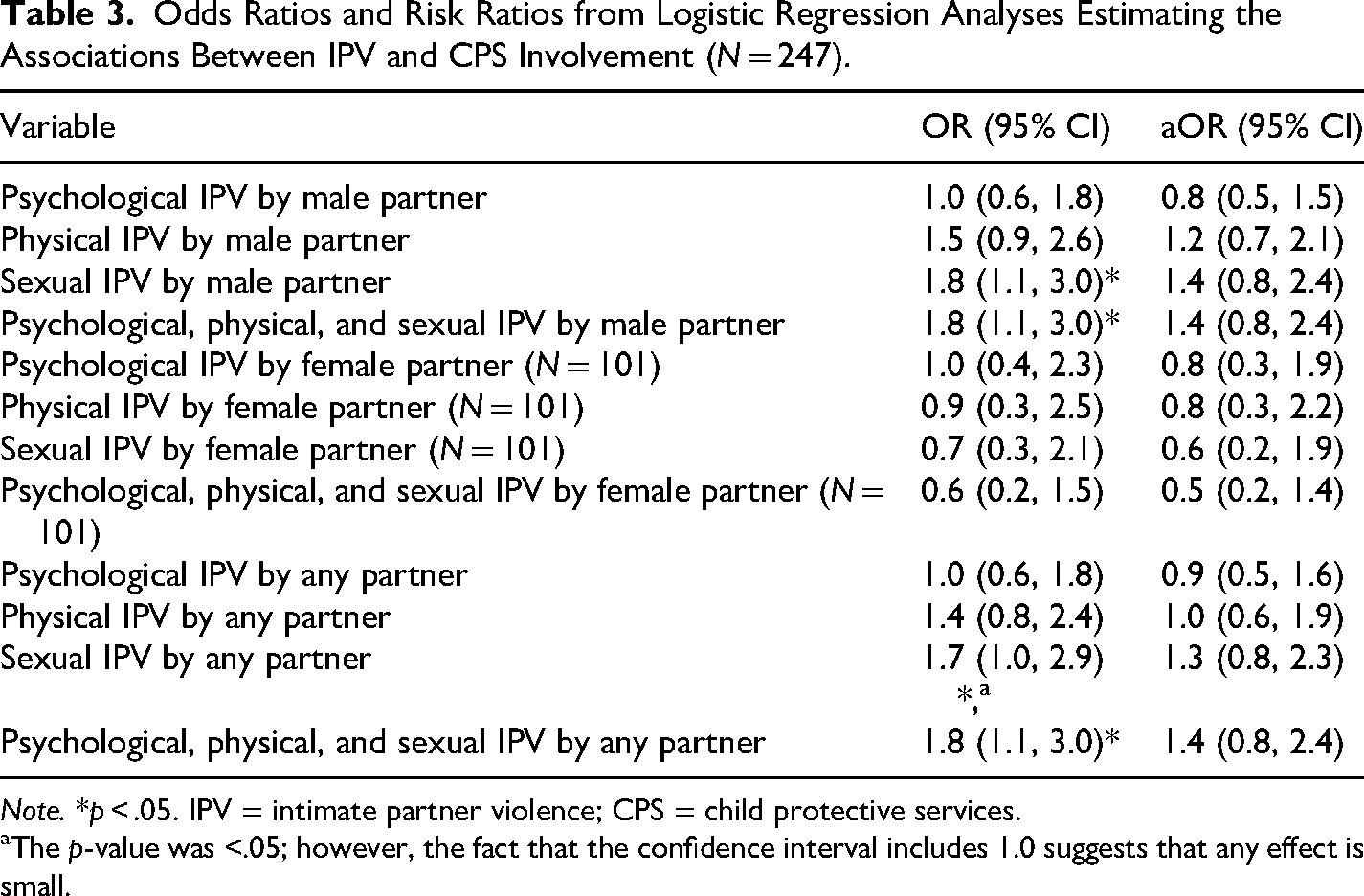
Note. *p < .05. IPV = intimate partner violence; CPS = child protective services.
The p-value was <.05; however, the fact that the confidence interval includes 1.0 suggests that any effect is small.
Discussion
This study found high rates of IPV and CPS involvement as parents among this sample of Black women in CSPs in NYC. We also found bivariate associations between experiencing different types of IPV, as perpetrated by male partners and by any partner regardless of sex, and CPS involvement. However, the significance of these associations attenuated with covariate adjustment in the multiple logistic regression models. Further, we did not find any associations between female-only perpetrated IPV and CPS involvement.
In this sample of Black women who have used drugs, who have or had children, and who are in CSPs in NYC, we observed high rates of IPV compared to the general population: Lifetime psychological and physical IPV rates were around 70%, respectively, as compared to nearly 54% for psychological aggression and 41% for physical IPV among non-Hispanic Black women in the general population (Breiding et al., 2015). These rates are higher still when compared to non-Hispanic White women in the general population who have reported psychological aggression (47.2%) and physical violence (30.5%) by intimate partners (Breiding et al., 2015).
Roughly half of the women in the study experienced sexual IPV, as compared to one in five women in the general population who experienced sexual violence by an intimate partner (CDC, 2022). This compares to the 8.8% and 17.4% of non-Hispanic Black women in the general population who have reported rape or other sexual violence by an intimate partner, respectively (Breiding et al., 2015). Roughly two-fifths of the women experienced all three forms of IPV, a notable finding given that few if any studies measure all three forms of IPV together, especially among Black women with children, who have used drugs, and who are involved in the criminal legal system.
Over half of the women (n = 138, 55.9%) had ever had an open or active case with CPS as parents. Surveillance data on parents’ prevalence of CPS involvement in New York or the US is sparse. However, Kim et al. (2017) found that children's lifetime prevalence of CPS involvement in the US to be 37.4%, rising to 53.0% for African-American children. It follows that national rates for parents would be lower given that the average parent has one or more children, all with variability by state. This paper's findings of higher rates of CPS involvement are important yet unsurprising for the following reason: the women in the study were already at heightened risk due to legal system involvement and substance use (all women in the study), high levels of economic instability, as evidenced through food insecurity (n = 162, 65.6%), and mental health history (n = 182, 73.7%).
Interestingly, mental health history was the only significant covariate in adjusted models, showing that women with mental health histories and female-perpetrated IPV had significantly higher odds of CPS involvement as parents than women without these experiences (see Appendix Table B). One possible explanation for this is the extremely inadequate and unavailable support for survivors of same-sex perpetrated IPV and/or the possibility that same-sex IPV is less likely to be reported, or acknowledged by systems; however, additional research is desperately needed in this area (Kar et al., 2023). Social support slightly decreased women's odds of CPS involvement; however, the significance of this relationship was lost when adjusting for risk factors, suggesting that social support may be insufficient to prevent CPS involvement when weighted against multiple, intersecting risk factors. These findings quantify the extent of this risk and reinforce that risk exists at multiple ecological levels of human experience (e.g., individual mental health and macro-related economic conditions or exosystemic disproportionate involvement with Black families), as understood through ecological theory and in the background literature. Similarly, the findings also highlight a point of resilience among women with children in their outreach to informal support systems.
Consistent with the study hypothesis, but only in models without controlling for covariates, sexual IPV and ever experiencing each type of IPV (i.e., psychological, physical, and sexual IPV) by male partners or by any partner regardless of sex were significantly associated with CPS involvement as parents. Women who experienced sexual IPV by any partner had 1.7 higher odds of CPS involvement, and women who experienced all three forms of IPV by any partner also had 1.8 higher odds of CPS involvement. These findings are consistent with Fedock et al. (2018) who found that multiple forms of stressful life experiences, including sexual IPV and other types of adult victimization along with CPS involvement, were interrelated forms of stressors contributing to adverse mental health experiences among women in the criminal legal system. Similarly, using child welfare reports in Canada, Gonzalez et al. (2020) found that children's exposure to multiple sub-types of IPV was more likely to warrant CPS responses like substantiation, court involvement, and ongoing case management.
We were unable to reject the null hypothesis in any models for psychological and physical IPV alone with CPS involvement. Regarding psychological IPV, Gonzalez et al. (2020) found that children's exposure to emotional or psychological IPV was least likely to warrant CPS interventions, particularly referrals for services, despite the impacts of this type of IPV exposure on children. Despite the fact that CPS caseworkers are trained to screen for IPV, these trainings may not be mandatory, and screening practices often focus on physical IPV alone, resulting in significant under-identification of active IPV by caseworkers as compared to mothers’ reports (Casanueva et al., 2014). Further, screening and increased CPS involvement do not necessarily yield helpful or appropriate interventions.
Our findings related to physical IPV are inconsistent with Gonzalez et al. (2020), who found that direct exposure to physical IPV was more likely to bring CPS intervention. This discrepancy may be explained by differences in study populations: Gonzalez et al. (2020) limited risk factors in their Canadian sample (e.g., only using data from cases in which IPV was the primary concern), whereas the women in the E-WORTH study faced a multitude of intersecting risk factors. It is also possible that protective factors and various forms of resilience balanced risk factors, which is a worthy topic of continued exploration in future studies.
We failed to reject the null hypothesis regarding IPV and CPS involvement in any of the adjusted regression models that included covariance adjustment for additional variables associated with CPS involvement. These findings suggest that mental health in particular confounds the relationship between IPV and CPS involvement. Future analyses could examine the moderating role of mental health in this population.
Limitations and Implications
Research Limitations
The findings reveal important descriptive experiences of IPV and CPS involvement among Black women who have used drugs, who have children, and who are in CSPs. Unadjusted models confirm that sexual and multiple forms of IPV and CPS involvement co-occur, for potential reasons explicated in our conceptual framework. As with any null findings in a study of associations, the adjusted findings do not prove there is no relationship between IPV and CPS involvement among Black women who have used drugs, who are involved in the criminal legal system, and who have children. Rather, the findings may highlight limitations of the study and/or indicate the need for more sophisticated measurement and/or modeling. Findings should be interpreted carefully given the lack of significance in adjusted models.
Practices and policies locally (e.g., New York City) and across states vary considerably. Therefore, the generalizability of these findings is limited to women involved in CSPs and CPS in New York City. Generalizability is also limited by the paper's use of a non-random intervention sample at baseline. This paper's use of IPV is restricted to psychological, physical, and sexual violence against women by male and/or female partners and, consequently, does not include perpetration of IPV against male or gender non-binary partners. These exclusions may bias results and represent an ongoing gap in existing literature. Though we chose covariates based on existing literature in conjunction with preliminary analytic results, failing to control for Latinx ethnicity, education, and other variables may have confounded results. The IPV measure also does not include economic or other forms of violence like reproductive health coercion, substance use coercion, or technology-facilitated IPV. Not all variables are time-matched (e.g., CPS involvement ever as parents versus food insecurity over the past 90 days). The study does not suggest causality or confirm directionality.
Finally, women may be hesitant to report IPV experiences, in addition to substance use, impacts on children, and help-seeking behaviors, in order to protect their and their children's safety (Follingstad & Rogers, 2013). Casanueva et al. (2014) found that increased IPV screening competence among CPS workers can improve detection of violence at the system level, which could help researchers triangulate data from multiple sources. Women may feel more comfortable reporting IPV experiences to researchers outside CPS and other reporting systems, especially if protective protocols are in place (Rizo et al., 2019). Again, however, improved screening practices do not equate to useful, safe, or appropriate interventions once CPS detects violence.
Future studies need to use larger sample sizes to increase the study's power and to expand the focus to include women as perpetrators of violence in same-sex and opposite-sex relationships. Future studies should also gather, compare, and contrast experiences by race and ethnicity both among and apart from Black-identifying women. Questions about CPS involvement should include different time periods (e.g., ever versus past year versus past 6 months). Longitudinal designs are also needed to improve causal inferences and linkages between different types of IPV and CPS involvement over time. Researchers could triangulate time-matched data on IPV experiences using women's reports, CPS reports, and at least one other source (e.g., children's reports, medical records, police reports), understanding their individual limitations but relative collective strength.
Implications for Practice, Policy, and Research
Given the high rates of IPV and CPS involvement as parents among the sample of women in the study population, practitioners and policy-makers should engage women in CSPs to improve understanding of how IPV, especially in the context of substance use, may manifest (Mirick, 2014). They can then tailor their recruitment, engagement efforts, interventions, services, and policies to help prevent and address IPV in the population, to the benefit of Black women, children, and communities. Our findings suggest that attention to the effects of poverty, mental health diagnoses, and social support can mitigate risk and potentially prevent unnecessary CPS intrusion into family life. Particular attention to preventing sexual IPV in this population also serves to protect women and their children. As Black women are disproportionately represented in CPS systems, practitioners and policy-makers working in or adjacent to these systems must challenge systemic practices and policies that portray Black women as deviant, unfit parents and instead focus on their strengths and protective capacities (Gurusami, 2019). Dettlaff and Boyd (2020) argue that such shifts in practice and policy must occur at more macro levels, such as through CPS agency leader's explicit commitment to addressing systemic racism, agency-community partnerships, and increased use of kinship care and other (subsidized) alternatives to foster care, especially in Black families. Though this study did not measure racism or its impact, their influence makes up part of the ecological theoretical perspective that contextualizes women's experiences of IPV and systems involvement, making them important to mention here.
Lastly, researchers can use the descriptive and correlative knowledge generated from this paper to inform future studies on CPS- and IPV-related interventions among women in CSPs, which remain limited among women involved in the criminal legal system and experiencing IPV (Macy et al., 2012; Proctor et al., 2011). Systems-involved individuals should be part of formulating research questions, programs, and policies locally, nationally, and globally to promote the safety and well-being of them and their children.
Footnotes
Acknowledgements
The authors are deeply grateful to the women who participated in the E-WORTH study, the Center for Court Innovation, the New York City Department of Probation, all partners at CSP sites, and the entire E-WORTH research team. The E-WORTH study was funded by the National Institute on Drug Abuse (NIDA) [grant number R01DA038122].
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse (grant number R01DA038122).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Biographies
Appendix Table A: Associations with Child Protective Services (CPS) Involvement ( N = 247).
| Variable | Total |
CPS, Yes |
CPS, No |
X 2 (t) |
|---|---|---|---|---|
| Psychological IPV by male partner | 0.0 | |||
| Yes | 175 (70.9%) | 98 (71.0%) | 77 (70.6%) | |
| No | 72 (29.1%) | 40 (29.0%) | 32 (29.4%) | |
| Physical IPV by male partner | 2.2 | |||
| Yes | 173 (70.0%) | 102 (73.9%) | 71 (65.1%) | |
| No | 74 (30.0%) | 36 (26.1%) | 38 (34.9%) | |
| Sexual IPV by male partner | 5.3* | |||
| Yes | 120 (48.6%) | 76 (55.1%) | 44 (40.4%) | |
| No | 127 (51.4%) | 62 (44.9%) | 65 (59.6%) | |
| Psychological, physical, and sexual IPV by male partner | 5.0* | |||
| Yes | 101 (40.9%) | 65 (47.1%) | 36 (33.0%) | |
| No | 146 (59.1%) | 73 (52.9%) | 73 (67.0%) | |
| Psychological IPV by any partner | 0.0 | |||
| Yes | 178 (72.1%) | 100 (72.5%) | 78 (71.6%) | |
| No | 69 (27.9%) | 38 (27.5%) | 31 (28.4%) | |
| Physical IPV by any partner | 1.4 | |||
| Yes | 175 (70.9%) | 102 (73.9%) | 73 (67.0%) | |
| No | 72 (29.1%) | 36 (26.1%) | 36 (33.0%) | |
| Sexual IPV by any partner | 4.6* | |||
| Yes | 121 (49.0%) | 76 (55.1%) | 45 (41.3%) | |
| No | 126 (51.0%) | 62 (44.9%) | 64 (58.7%) | |
| Psychological, physical, and sexual IPV by any partner | 4.8* | |||
| Yes | 103 (41.7%) | 66 (47.8%) | 37 (33.9%) | |
| No | 144 (58.3%) | 72 (52.2%) | 72 (66.1%) | |
| Food insecurity past 90 days | 6.6* | |||
| Yes | 162 (65.6%) | 100 (72.5%) | 62 (56.9%) | |
| No | 85 (34.4%) | 38 (27.5%) | 47 (43.1%) | |
| Ever mental health diagnosis or suicide attempt | 7.4* | |||
| Yes | 182 (73.7%) | 111 (80.4%) | 71 (65.1%) | |
| No | 65 (26.3%) | 27 (19.6%) | 38 (34.9%) | |
| Age in years [mean (SD)] | 34.8 (11.1) | 34.5 (10.1) | 35.1 (12.2) | (0.4) |
| Social support scale (ESSI) [mean (SD)] | 9.7 (4.0) | 9.2 (3.9) | 10.4 (3.9) | (2.3)* |
| Variable | Total |
CPS, Yes |
CPS, No |
X 2 |
|---|---|---|---|---|
| Psychological IPV by female partner | 0.0 | |||
| Yes | 32 (31.7%) | 19 (31.7%) | 13 (31.7%) | |
| No | 69 (68.3%) | 41 (68.3%) | 28 (68.3%) | |
| Physical IPV by female partner | 0.0 | |||
| Yes | 19 (18.8%) | 11 (18.3%) | 8 (19.5%) | |
| No | 82 (81.2%) | 49 (81.7%) | 33 (80.5%) | |
| Sexual IPV by female partner | 0.4 | |||
| Yes | 17 (16.8%) | 9 (15.0%) | 8 (19.5%) | |
| No | 84 (83.2%) | 51 (85.0%) | 33 (80.5%) | |
| Psychological, physical, and sexual IPV by female partner | 1.2 | |||
| Yes | 24 (23.8%) | 12 (20.0%) | 12 (29.3%) | |
| No | 77 (76.2%) | 48 (80.0%) | 29 (70.7%) |
Note. *p < .05. IPV = intimate partner violence.
Appendix Table B: Unadjusted and Adjusted Odds Ratios from Regression Analyses Estimating the Associations Between IPV and CPS Involvement ( N = 247).
| Variable | OR (95% CI) | aOR (95% CI) |
|---|---|---|
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.0) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.7 (1.0, 3.0) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 1.8 (1.0, 3.3) |
| Social support | 0.9 (0.9, 1.0)*,a | 0.9 (0.9, 1.0) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.0) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.7 (1.0, 2.9) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 1.7 (0.9, 3.1) |
| Social support | 0.9 (0.9, 1.0)*,a | 1.0 (0.9, 1.0) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.0) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.6 (0.9, 2.9) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 1.6 (0.9, 3.0) |
| Social support | 0.9 (0.9, 1.0)*,a | 1.0 (0.9, 1.0) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.0) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.6 (0.9, 2.8) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 1.7 (0.9, 3.1) |
| Social support | 0.9 (0.9, 1.0)*,a | 1.0 (0.9, 1.0) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.1) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.3 (0.5, 3.3) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 3.8 (1.1, 13.1)* |
| Social support | 0.9 (0.9, 1.0)*,a | 1.0 (0.9, 1.1) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.1) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.2 (0.5, 3.2) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 3.8 (1.1, 12.9)* |
| Social support | 0.9, (0.9, 1.0)*,a | 1.0 (0.9, 1.1) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.1) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.3 (0.5, 3.3) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 3.7 (1.1, 12.5)* |
| Social support | 0.9 (0.9, 1.0)*,a | 1.0 (0.9, 1.1) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.1) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.3 (0.5, 3.6) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 3.7 (1.1, 12.6)* |
| Social support | 0.9 (0.9, 1.0)*,a | 1.0 (0.9, 1.1) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.0) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.7 (1.0, 3.0) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 1.8 (1.0, 3.3) |
| Social support | 0.9 (0.9, 1.0)*,a | 0.9 (0.9, 1.0) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.0) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.7 (1.0, 3.0) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 1.7 (0.9, 3.2) |
| Social support | 0.9 (0.9, 1.0)*,a | 0.9 (0.9, 1.0) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.0) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.6 (0.9, 2.9) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 1.6 (0.9, 3.0) |
| Social support | 0.9 (0.9, 1.0)*,a | 1.0 (0.9, 1.0) |
|
|
|
|
| Age in years | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.0) |
| Food insecurity past 90 days | 2.0 (1.2, 3.4)* | 1.6 (0.9, 2.9) |
| Ever mental health diagnosis or suicide attempt | 2.2 (1.2, 3.9)* | 1.7 (0.9, 3.1) |
| Social support | 0.9 (0.9, 1.0)*,a | 1.0 (0.9, 1.0) |
Note. *p < .05. IPV = intimate partner violence; CPS = child protective services.
The p-value was <.05; however, the fact that the confidence interval includes 1.0 suggests that any effect is small.
Appendix Table C: Crude and Adjusted Risk Ratios from Sensitivity Analyses ( N = 247).
| Predictor | RR (95% CI) | aRR (95% CI) |
|---|---|---|
| Psychological IPV by male partner | 1.0 (0.8, 1.3) | 0.9 (0.7, 1.2) |
| Physical IPV by male partner | 1.2 (0.9, 1.6) | 1.1 (0.8, 1.4) |
| Sexual IPV by male partner | 1.3 (1.0, 1.6)* | 1.1 (0.9, 1.4) |
| Psychological, physical, and sexual IPV by male partner | 1.3 (1.0, 1.6)* | 1.1 (0.9, 1.4) |
| Psychological IPV by female partner (N = 101) | 1.0 (0.7, 1.4) | 0.9 (0.6, 1.3) |
| Physical IPV by female partner (N = 101) | 1.0 (0.6, 1.5) | 0.9 (0.6, 1.4) |
| Sexual IPV by female partner (N = 101) | 0.9 (0.5, 1.4) | 0.8 (0.5, 1.4) |
| Psychological, physical, and sexual IPV by female partner (N = 101) | 0.8 (0.5, 1.2) | 0.8 (0.5, 1.2) |
| Psychological IPV by any partner | 1.0 (0.8, 1.3) | 0.9 (0.7, 1.2) |
| Physical IPV by any partner | 1.2 (0.9, 1.5) | 1.0 (0.8, 1.3) |
| Sexual IPV by any partner | 1.3 (1.0, 1.6)* | 1.1 (0.9, 1.4) |
| Psychological, physical, and sexual IPV by any partner | 1.3 (1.0, 1.6)* | 1.1 (0.9, 1.4) |
Note. *p < .05. IPV = intimate partner violence.