
Abstract
This study examined moral injury (MI) among women survivors (N = 142) of intimate partner sexual violence (IPSV). IPSV was significantly associated with shame-related moral injury, trust-violation-related moral injury, and posttraumatic stress disorder (PTSD). Results revealed significant indirect effects of IPSV on PTSD via shame-related moral injury and trust-violation-related moral injury. Reflexive thematic analysis of open-ended responses identified three key themes: (a) Self-Betrayal, (b) Self-Blame, and (c) Other-Betrayal. Our findings indicate that moral injury may serve as an important mechanism linking IPSV to PTSD among IPSV survivors.
Keywords
Intimate partner sexual violence (IPSV) encompasses any forced or coerced sexual act perpetrated within the context of an intimate relationship, including rape, sexual abuse, or sexual coercion (Bagwell-Gray et al., 2015). According to recent nationally representative data, intimate partners are responsible for more than one-third of all rapes and over half of all acts of sexual coercion committed against women (Basile et al., 2022). Despite this, IPSV has not been widely studied (Bagwell-Gray et al., 2015; Tarzia, 2021). Bagwell-Gray et al. (2015) suggest that one reason for this dearth of research may be due to public perceptions that IPSV is not as harmful as sexual assault perpetrated by strangers or acquaintances. For example, assaults perpetrated by strangers are more likely to be investigated and deemed credible by law enforcement than assaults perpetrated by an intimate partner (Tellis & Spohn, 2008). Additionally, in Ferro et al. (2008), participants were less likely to believe that rape would cause the victim psychological damage when the perpetrator was their husband.
However, despite public perceptions, empirical research consistently demonstrates that IPSV survivors can and do experience significant adverse outcomes, including depression and posttraumatic stress disorder (PTSD; Barker et al., 2019; Tarzia et al., 2018), suicide attempts (Barker et al., 2019), and death by homicide (Barker et al., 2019). IPSV survivors are at a greater risk of adverse mental health outcomes relative to survivors of IPV where sexual assault has not taken place (Honda et al., 2018; McFarlane et al., 2005). In qualitative research, IPSV survivors report that sexual violence perpetrated by their partner constituted a unique form of trauma, and some wished that they had “only” experienced physical violence (Tarzia, 2020). Further, and in contradiction of public perceptions, research finds that IPSV survivors report significantly higher PTSD and depression relative to women who were assaulted by nonpartners (Tarzia et al., 2018).
One reason that IPSV survivors may experience particularly deleterious outcomes is because these experiences constitute a high betrayal trauma (Freyd, 1996). According to Betrayal Trauma Theory (BTT; Freyd, 1996), posttraumatic responses are shaped not merely by the circumstances of the traumatic event, but also by the relational context between the victim and the perpetrator, such that experiencing interpersonal trauma is more injurious when perpetrated by someone close to the victim (Freyd, 1996). According to Freyd (1996), traumas fall into three categories: low betrayal (e.g., car accidents), medium betrayal (e.g., assault by a stranger), and high betrayal (e.g., abuse by a romantic partner). Research finds that high betrayal trauma is associated with significantly worse health outcomes (Martin et al., 2013; Platt & Freyd, 2015). For example, survivors of high betrayal trauma are at an increased risk of shame (Platt & Freyd, 2015) relative to survivors of low betrayal trauma.
The consequences of high betrayal trauma are particularly well-illustrated in qualitative accounts from IPSV survivors (Tarzia, 2020; Sanchez et al., 2024). In Tarzia's (2020) qualitative study, survivors reported feeling that their trust in their partner had been shattered, with one woman stating of her partner: “That is one person in your life that you should be able to trust beyond anybody else and to have that trust broken, I think is worse than if it was a stranger” (Tarzia, 2020, p. 291). Moreover, many IPSV survivors report feelings of negative moral emotions (e.g., guilt, shame; Beck et al., 2011), and prior research finds that survivors who engage in self-blame experience elevated psychological distress (Peter-Hagene & Ullman, 2016). Notably, both betrayal and negative moral emotions (e.g., shame) have emerged as core facets of moral injury, a potential clinical problem (Litz & Walker, 2025) that can develop following experiences that transgress an individual's moral beliefs (Litz et al., 2022), that may be particularly relevant to IPSV (Kanter et al., 2025).
Moral Injury
Psychiatrist Jonathan Shay (1994) is credited with introducing the term “moral injury.” Shay initially conceptualized moral injury as a betrayal of moral expectations by authority figures in high-stakes contexts (1994), while Litz et al. (2009) emphasized the role of acts of commission and omission (i.e., perpetrating or failing to prevent morally transgressive acts) as potential precursors to moral injury. The field has since expanded since these two early definitions (Litz et al., 2022; Litz & Walker, 2025; VanderWeele et al., 2025). Importantly, in newer conceptualizations and definitions, moral injury can develop from a wide range of potentially morally injurious experiences (PMIEs), including exposure to interpersonal victimization (Litz & Walker, 2025; VanderWeele et al., 2025). According to Litz & Walker (2025), MI is a “potential clinical problem” comprising functional impairments in perceptions of oneself or others, moral thinking, social behavior, moral emotions and moods, self-harming/sabotaging, and changes in beliefs about the meaning and purpose of life that is indexed to a “worst and most currently distressing experience” (p. 259). Thus, moral injury itself is not considered a mental illness; however, it is consistently and strongly related to adverse mental health outcomes (see Hall et al., 2021 for a systematic review).
Prior research has delineated between two distinct dimensions of moral injury: Shame-related (SR), which encompasses internalizing outcomes such as shame, self-blame, self-dehumanization, avoidance, isolation, and a loss of trust in oneself (Currier et al., 2018; Litz et al., 2022; Litz & Walker, 2025) and trust-violation-related (TVR), which encompasses externalizing outcomes such as anger, broken-heartedness, disillusionment, distrust, and a loss of faith in humanity (Currier et al., 2018; Litz et al., 2022; Litz & Walker, 2025), associated with a PMIE. Importantly, survivors of IPSV may experience both dimensions of moral injury, given that research consistently finds outcomes related to both SR moral injury (e.g., shame, self-blame; Lindgren & Renck, 2008; Platt & Freyd, 2015) and TVR moral injury (e.g., betrayal; Tarzia, 2020) among IPV survivors.
While originally studied in military contexts, researchers have recently begun to expand the concept of moral injury to civilian traumas (Kanter & Hassija, 2025, 2026; Kanter et al., 2025a; Kanter et al., 2025b; Lathan et al., 2022), and some research has proposed that moral injury may act as a key mechanism through which traumatic experiences lead to adverse mental health (Kanter & Hassija, 2026; Kanter et al., 2025a; Kanter et al., 2025b; Roth et al., 2023). Empirical research on moral injury in civilian sexual violence contexts is limited, but some initial findings suggest its relevance. For example, Lathan et al. (2022) examined moral injury among trauma-exposed civilians and found that experiencing sexual assault remained a significant predictor of moral injury-related distress (i.e., both SR and TVR moral injury) after accounting for other potentially traumatic events (Lathan et al., 2022).
In addition, Kanter and Hassija (2026) found that greater IPV (i.e., a PMIE) was positively associated with both dimensions of moral injury outcomes among a sample of U.S. college students. To these authors’ knowledge, only one prior study has examined moral injury in relation to IPSV, specifically (Kanter et al., 2025a), which demonstrated significant relationships between IPSV and both forms of moral injury (i.e., SR and TVR moral injury) in a sample of U.S. women. While empirical research is limited, there is a broader field of literature, particularly among qualitative research, that helps demonstrate why IPSV survivors may experience moral injury. For example, research among survivors of IPV found an emergent theme of moral disgust, such that survivors felt disgusted not only with their partners, but with themselves as well (Akça & Gençöz, 2021). Although the literature remains limited, current findings point toward a potentially meaningful relationship between IPSV and moral injury.
However, given the relative lack of research between moral injury and interpersonal victimization among civilians, little is known about how both dimensions of moral injury (i.e., SR and TVR) may present in these populations. According to a recent review, half of the extant research on moral injury has been conducted among military populations, with the remaining half conducted predominantly among healthcare and public safety personnel (Beech et al., 2024). Yet the way moral injury presents among military, healthcare, and public safety personnel may be meaningfully different from how it presents in interpersonal violence contexts. This may be particularly the case for SR moral injury.
For example, SR moral injury has often been framed as developing following an experience in which an individual perpetrates or fails to prevent an act that transgresses their moral code (Litz et al., 2009; Litz et al., 2022; Litz & Walker, 2025). In military contexts, such potentially morally transgressive acts may include killing others or failing to prevent someone else's death (Litz et al., 2009). The reasons underlying why IPSV survivors might experience SR moral injury may be altogether very different. According to BTT (Freyd, 1996), when individuals are victimized by someone who they trust, they often suppress awareness of the abuse, blaming themselves in the process in order to maintain the relationship. Thus, rather than arising from perpetrating harm against others, elevated SR moral injury among IPSV survivors may reflect self-blame (e.g., for not leaving, for “causing” the abuse) such that survivors may perceive themselves, rather than the perpetrator (i.e., their intimate partner), as having acted in a way that transgressed their moral values.
The Current Study
Empirical research on the relationship between IPSV and moral injury remains limited (Kanter et al., 2025a). The vast majority of studies on moral injury have focused on military and healthcare populations (Beech et al., 2024), thereby leaving significant gaps in understanding how moral injury manifests among civilians—particularly survivors of interpersonal traumas (Kanter & Hassija, 2026; Kanter et al., 2025a; Kanter et al., 2025b; Lathan et al., 2022). Given that IPSV often involves severe betrayal, coercion, and violations of bodily autonomy by an intimate partner (Bagwell-Gray et al., 2015), it is important to examine whether moral injury plays a role in shaping outcomes for these survivors. Thus, this study is one of the first to examine IPSV as a PMIE (Kanter et al., 2025a). Further, although Kanter et al. (2025a) found elevated levels of both dimensions of moral injury in relation to IPSV among a sample of Christian women, by incorporating a convergent mixed-methods design, this study also seeks to provide insights from open-ended responses to help explain why IPSV survivors have reported both dimensions of moral injury in prior research.
First, we hypothesized that IPSV would be positively associated with SR moral injury, TVR moral injury, and PTSD symptoms (H1). Second, we predicted that PTSD symptoms would be positively associated with both SR and TVR moral injury (H2). Third, we hypothesized that there would be indirect effects of IPSV on PTSD through both dimensions of moral injury (H3). To complement these quantitative aims, we also aimed to collect data from open-ended responses to explore how IPSV survivors describe (a) negative moral emotions, such as guilt and shame, (b) betrayal by others, and (c) internal moral conflict, stemming from their experiences.
Method
Participants and Procedure
The present study was approved by the University Institutional Review Board (#IRB-FY2025-171). We recruited a convenience sample through the online sampling pool, Prolific. Previous research finds that participants on Prolific provide higher quality data relative to participants on other platforms, including higher quality responses to open-ended questions in surveys (e.g., Amazon Mechanical Turk, SONA; Douglas et al., 2023). We used Prolific's prescreening measures to limit participation to individuals who were located in the United States, fluent in English, and identified as women. Participants who self-selected into the study completed a two-item IPSV prescreening measure (Tarzia, 2020; Tarzia, 2021). Participants were asked to indicate (a) whether “things happened in the bedroom” that they did not want and (b) whether they “…felt pressured, unsafe, or afraid during sex with a boyfriend, girlfriend, husband, or partner?” in the past 12 months (yes/no). Respondents who replied “no” to either question (n = 204) were thanked for their time, redirected back to the Prolific platform, and paid a small amount commensurate with the time they spent on the study ($0.20). Those who responded “yes” to both items (n = 169) were invited to participate in the present study.
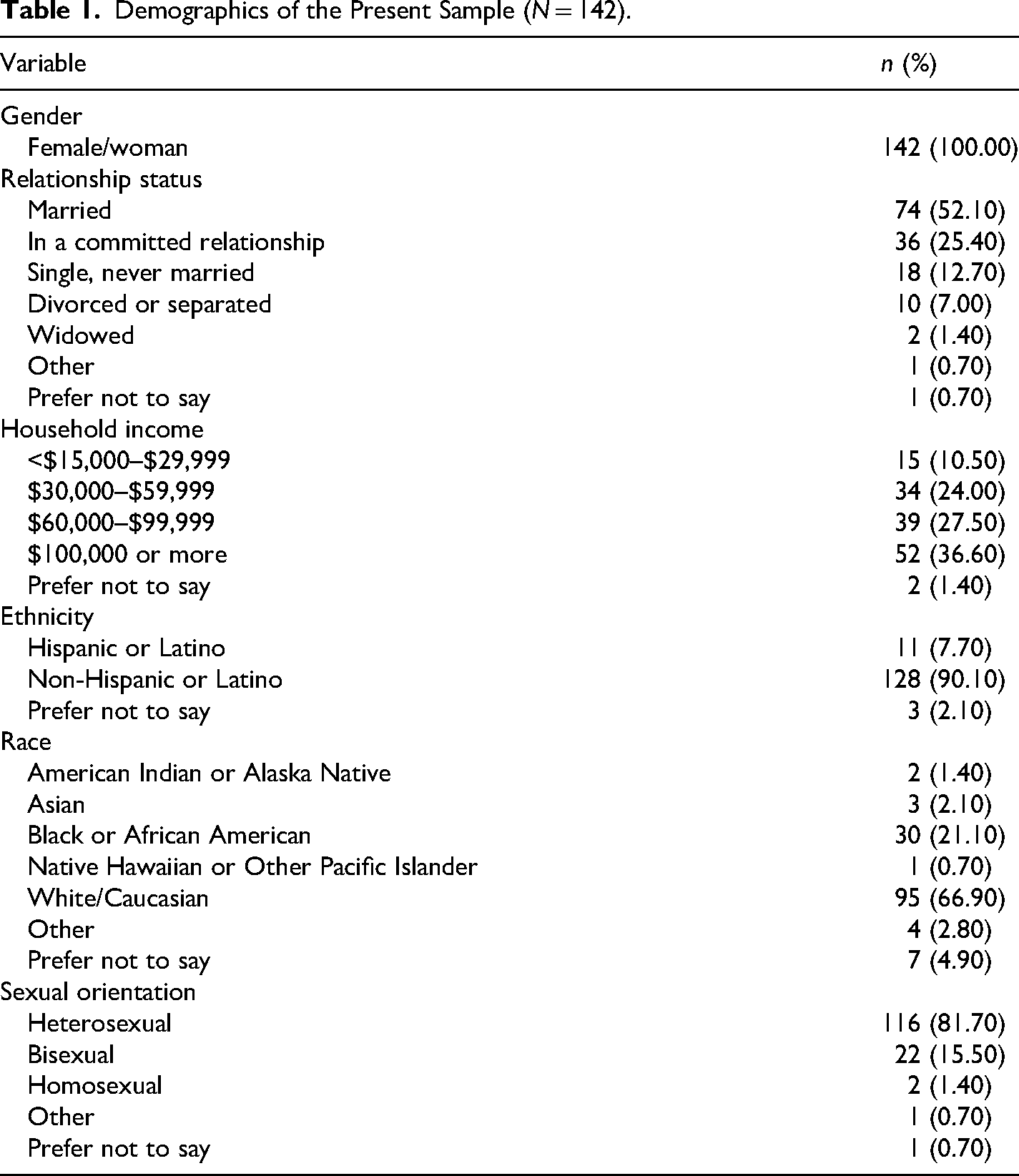
Upon accessing the survey, participants were provided an informed consent form, which informed them of the study topic (i.e., how difficult or distressing experiences in romantic relationships may influence well-being). Each participant indicated their consent to participate in the study. After providing informed consent, participants completed the IPSVS, MIOS, PCL-5, and open-ended responses in randomized order to control for order effects, followed by demographics. Lastly, participants were debriefed and provided resources for support (i.e., mental health hotlines). The survey took approximately 20 min to complete, and participants were paid $3.00 for their time. Participants who failed at least on attention check (n = 7) and/or scored ≥ 30 on Qualtrics’ fraud detection system (n = 20) were excluded from analysis. Excluding participants who score ≥ 30 is consistent with Qualtrics’ recommended threshold for identifying responses that are likely fraudulent or completed by bots (Bonett et al., 2024; Qualtrics, 2022). The final sample consisted of 142 women who ranged in age from 18 to 77 (M = 38.43) and largely identified as heterosexual (n = 116, 81.70%) and White (n = 92, 69.00%). In terms of relationship status, most participants reported that they were married (n = 74, 52.10%). See Table 1 for additional demographic information.
Demographics of the Present Sample (N = 142).
Measures
Demographics. A demographics questionnaire was created for the present study. Participants were asked to indicate their age, gender, sexual orientation, ethnicity, race, relationship status, and annual household income.
IPSV. The Intimate Partner Sexual Violence Scale (IPSVS; Tarzia et al., 2024) is a 20-item self-report measure designed to assess sexual violence in intimate relationships. Participants were requested to indicate whether a romantic partner or ex-partner (of a relationship lasting longer than 1 month) had engaged in each of the listed behaviors (yes/no) within the prior 12 months. The IPSVS consists of three factors: Dominance and humiliation (e.g., “Made me have sex in front of my child/ren or other people”), Emotional coercion (e.g., “Accused me of cheating or not loving them when I said ‘No’ to sex”), and Aggressive indifference (e.g., “Made me participate in sex acts or sexual positions that they knew I did not like”). The IPSVS has strong content validity, having been developed based on extensive qualitative research with IPSV survivors (Tarzia et al., 2024) and has demonstrated good psychometric properties (α = .89). For the purposes of the present study, a sum IPSVS score was calculated, with possible scores ranging from 0 to 20. Higher scores indicated a greater prevalence of IPSV experiences. Internal consistency in the present sample was good (α = .85).
Moral Injury. The Moral Injury Outcome Scale (MIOS; Litz et al., 2022) is a 14-item self-report measure assessing the impact of PMIEs. For this study, we modified the instructions to assess PMIEs within current or former intimate relationships, asking whether participants have had at least one experience related to unwanted sexual experiences in their current or former intimate relationship that violated moral codes or values within the prior 12 months (yes/no). Participants who responded “yes” completed the remainder of the questionnaire. Participants first reported which aspect of the experience was most distressing: (a) acting (or failing to act), (b) witnessing another's act (or failure to act), or (c) being directly affected by an act, that went against their moral code or values. Participants could select all that applied.
Following this, participants answered the 14 main MIOS items, which measure two dimensions: SR moral injury (seven items; e.g., “I blame myself,” “I am not the good person I thought I was”) and TVR moral injury (seven items; e.g., “I have lost faith in humanity,” “I lost trust in others”). Participants rate their agreement with each item on a 5-point Likert scale from 0 (strongly disagree) to 4 (strongly agree), with possible scores ranging from 0 to 28 for both subscales. Both subscales have demonstrated strong internal consistency (α = .83−.95 across samples) and convergent validity with measures of psychological distress (Litz et al., 2022). In the present sample, internal consistency was good for SR moral injury (α = .85) and TVR moral injury (α = .84).
Moral Injury Functional Outcomes. Following the MIOS, participants complete an adapted version of the Brief Inventory of Psychosocial Functioning (B-IPF; Kleiman et al., 2020), assessing functional impairment related to moral injury symptoms across various domains (e.g., “Work,” “Friendships or socializing”). Items are rated on a 7-point Likert scale from 0 (not at all) to 6 (extremely) or “n/a,” if the domain does not apply. The B-IPF total score is calculated by summing completed items, dividing by the maximum possible score based on applicable items, and multiplying by 100, with possible scores ranging from 0 to 100. The B-IPF demonstrates strong psychometric properties, with high internal consistency (α = .84) and adequate test–retest reliability (r = .65, p < .001). Internal consistency in the present sample was good (α = .88).
Posttraumatic Stress Disorder. PTSD symptoms were assessed using the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013). The PCL-5 is a 20-item self-report measure that assesses the severity of DSM-5 PTSD symptoms over the past month. For this study, we contextualized the instructions to focus on participants’ worst experience related to unwanted sexual experiences within a current or former romantic relationship that occurred in the previous 12 months. Participants were first asked to briefly describe this experience in a text entry field, if comfortable. The PCL-5 measures symptoms across four PTSD symptom clusters: intrusion symptoms, avoidance symptoms, negative alterations in cognitions and mood, and alterations in arousal and reactivity. Items are rated on a 5-point scale ranging from 0 (not at all) to 4 (extremely), with possible scores ranging from 0 to 80. Higher scores indicate greater PTSD symptom severity. The PCL-5 has demonstrated strong psychometric properties, including excellent internal consistency (α = .94) and convergent and discriminant validity (Blevins et al., 2015). In the present sample, internal consistency was excellent (α = .95).
Open-Ended Survey Responses. Participants responded to the following three open-ended prompts that were incorporated within the survey. Respondents were instructed that they could provide as much or as little detail as they felt comfortable sharing and could skip any questions they preferred not to answer. The prompts are included below:
Sometimes when people experience unwanted or harmful sexual experiences in relationships, they can experience negative emotions—like guilt and shame. Have you ever experienced these emotions in relation to your experiences in a relationship? If so, can you describe how? For some people, unwanted or harmful sexual experiences can lead to feelings of betrayal or disappointment in their partner or others. Have you experienced a sense of betrayal due to your experiences? If so, can you describe how? Some individuals experience distress when their actions conflict with their personal values. Have you ever felt distress or moral conflict regarding how you responded to certain situations in your relationship? If so, can you describe how?
Data Analysis
Quantitative data were cleaned and analyzed using packages from the tidyverse (Wickham et al., 2019) in RStudio (Posit Software, PBC, 2025), an integrated development environment for R (R Core Team, 2025). Prior to hypothesis testing, descriptive statistics were examined, and all variables were screened for normality, which uncovered that several study variables were positively skewed. As a result, Spearman's rank-order correlations were conducted using the Hmisc package (Harrell, 2025), with bootstrapped confidence intervals calculated via the boot package (Canty & Ripley, 2024). Demographic variables (i.e., race, income, and sexual orientation) were dichotomized for analytic purposes (Race: 1 = White, 0 = Non-White; Income: 1 ≥ $59,999, 0 ≥ $59,999; Sexual orientation: 1 = Sexual minority, 0 = Heterosexual). These variables, as well as age (continuous), were included as covariates in all models. SR and TVR moral injury were entered as predictors in separate models to (a) avoid potential multicollinearity (given the high intercorrelation between SR and TVR moral injury; see Table 3) and (b) to better understand the potential unique effects of IPSV on both dimensions of moral injury. To assess indirect effects, bias-corrected bootstrapped confidence intervals (5,000 resamples) were generated using lavaan (Rosseel, 2012), as this approach is robust to non-normality and is considered appropriate for mediation models involving variables with skewed distributions (Rosseel, 2012). Assumption checks were conducted for each regression model, with residuals indicating reasonably normal distributions. Furthermore, VIF values for all predictors were below accepted thresholds (i.e., <5).
To analyze the open-ended responses, we utilized reflexive thematic analysis to examine the textual data, as this approach is particularly valuable for investigating sensitive topics where existing research is limited (Braun & Clarke, 2006; Campbell et al., 2019). Codes were generated by the first author (Rachel L. Kanter) and refined through discussions with the second author (Christina M. Hassija). Our data analysis process involved several systematic stages. First, all narrative responses were transcribed and imported into MAXQDA (Verbi Software, 2023) for organization and coding. We followed the process for thematic analyses outlined by Braun and Clarke (2006). First, the first author familiarized themselves with the dataset through multiple readings of all responses. Next, Rachel L. Kanter generated preliminary codes that identified meaningful elements within the responses. This coding process remained primarily inductive, thus allowing patterns to emerge from the data. Following the initial coding, the first author identified potential thematic patterns across participant narratives. All themes reflected patterns found in multiple participants’ accounts. It should be noted that coding did not involve independent, blind double-coding; instead, both authors (Rachel L. Kanter and Christina M. Hassija) were involved in developing the final themes to ensure that they accurately represented the data and answered the research questions, following which the themes were finalized and structured into a coherent narrative.
Results
Quantitative Results
Of the 142 participants, 119 (83.80%) reported experiencing a morally injurious event (see Table 2 for PMIE characteristics and moral injury functional outcomes). Among those individuals (n = 119), the most distressing aspects of the event were categorized as follows: 92 (28.70%) reported personal transgressions, 80 (24.90%) reported witnessing a transgression, and 81 (25.20%) reported being directly affected by a transgression. The mean scores for the study variables were as follows: IPSV (M = 7.27, SD = 4.46), SR moral injury (M = 8.27, SD = 6.34, TVR moral injury (M = 12.35, SD = 7.87), and PTSD (M = 40.74, SD = 17.16). See Table 3 for descriptives (Table 2).
Characteristics of Morally Injurious Events and Functional Outcomes (N = 142).
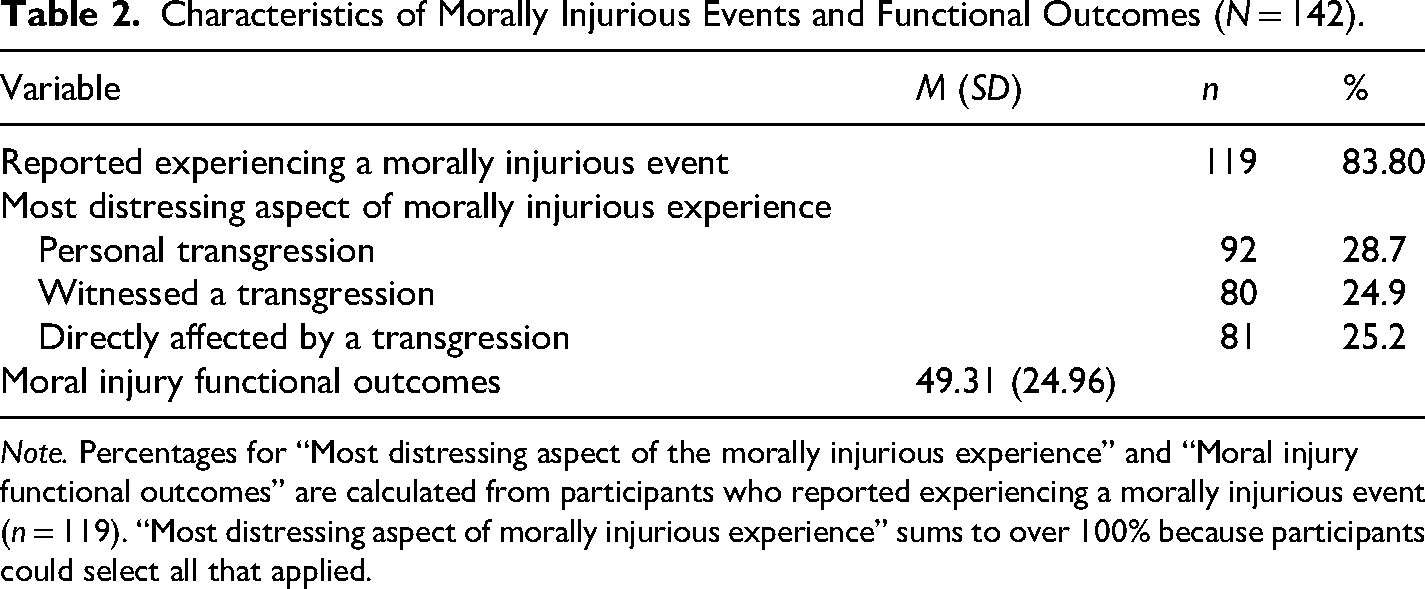
Note. Percentages for “Most distressing aspect of the morally injurious experience” and “Moral injury functional outcomes” are calculated from participants who reported experiencing a morally injurious event (n = 119). “Most distressing aspect of morally injurious experience” sums to over 100% because participants could select all that applied.
Correlations Among Study Variables (N = 142).
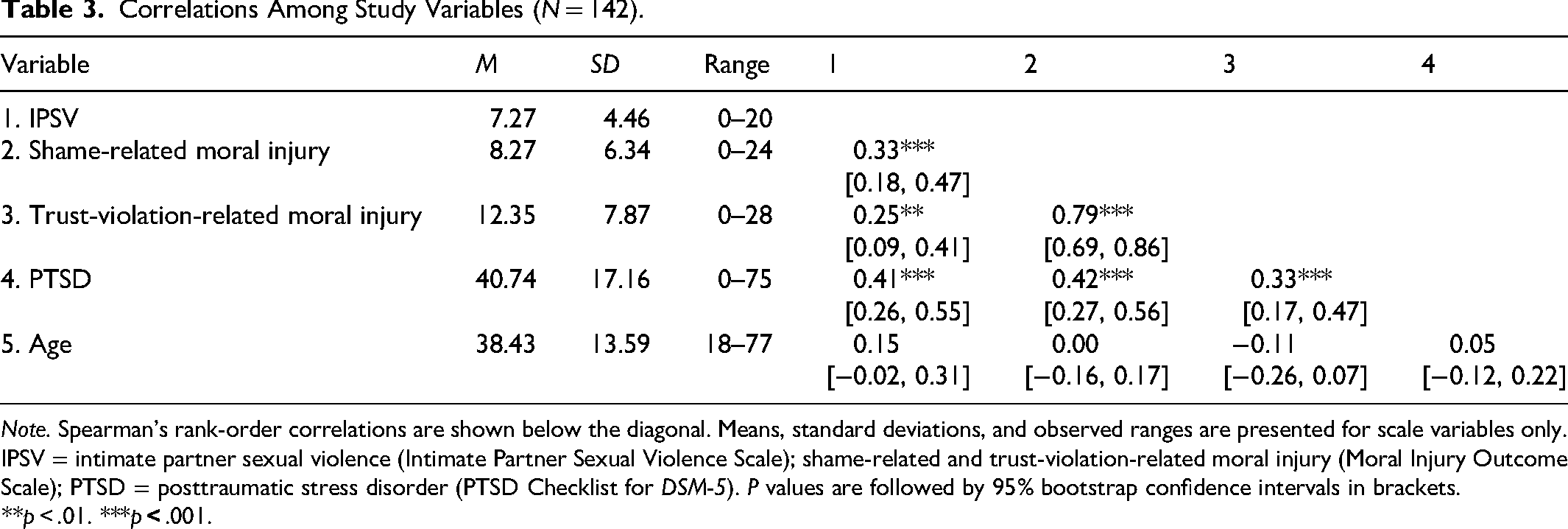
Note. Spearman's rank-order correlations are shown below the diagonal. Means, standard deviations, and observed ranges are presented for scale variables only. IPSV = intimate partner sexual violence (Intimate Partner Sexual Violence Scale); shame-related and trust-violation-related moral injury (Moral Injury Outcome Scale); PTSD = posttraumatic stress disorder (PTSD Checklist for DSM-5). P values are followed by 95% bootstrap confidence intervals in brackets.
**p < .01. ***p
Associations Between Variables. IPSV was significantly correlated with SR moral injury (ρ = 0.33, 95% CI [0.18, 0.47], p < .001), TVR moral injury (ρ = 0.25, p = .002, 95% CI [0.09, 0.41]), and PTSD (ρ = 0.41, p < .001, 95% CI [0.26, 0.55]). Meanwhile, SR moral injury (ρ = 0.42, p < .001, 95% CI [0.27, 056]) and TVR moral injury (ρ = 0.33, p < .001, 95% CI [0.17, 0.47]) were both significantly associated with PTSD. See Table 3 for correlations. Race, income, and sexual orientation showed no significant associations with primary study variables, with one exception of a small positive association observed between sexual orientation and PTSD (ρ = 0.17, p = .05, 95% CI [0.00, 0.34]), such that sexual minority participants reported higher PTSD symptoms.
Mediation Analyses. Two mediation models were conducted using structural equation modeling with bootstrapped standard errors (5,000 draws) to examine whether SR and TVR moral injury each independently mediated the relationship between IPSV and PTSD symptoms, controlling for age, income, race, and sexual minority status.
In the first model (see Figure 1), IPSV was a significant positive predictor of SR moral injury (β = 0.43, p < .001, 95% CI [0.41, 0.84]), and SR moral injury was a significant positive predictor of PTSD symptoms (β = 0.38, p < .001, 95% CI [0.58, 1.39]). The direct effect of IPSV on PTSD symptoms remained significant after accounting for SR moral injury (β = 0.17, p < .001, 95% CI [0.41, 0.84]), and the indirect effect of IPSV on PTSD symptoms via SR moral injury was also significant (β = 0.16, p < .001, 95% CI [0.31, 0.96]). None of the assessed covariates significantly predicted SR moral injury or PTSD in this model.
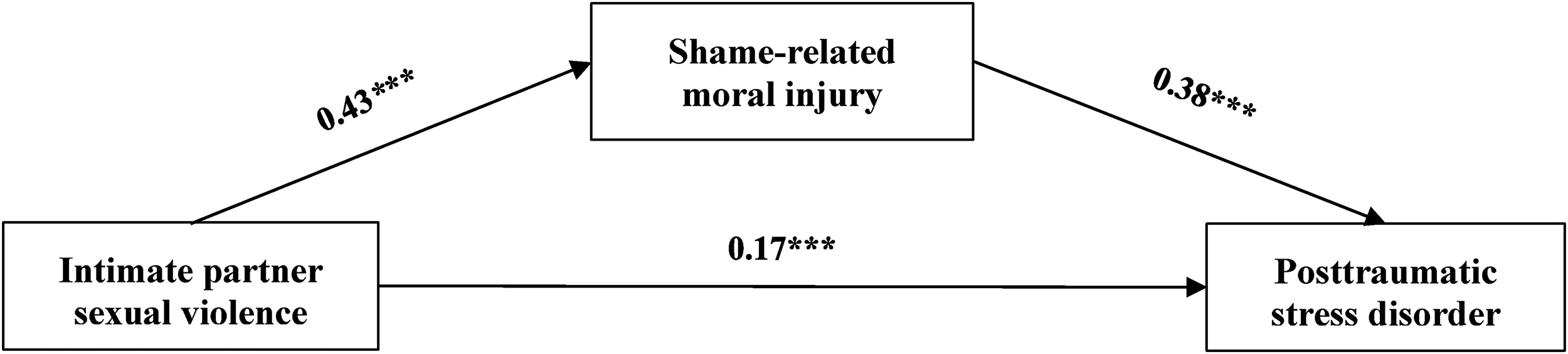
Standardized regression coefficients from a structural equation model testing the indirect effects of shame-related moral injury in the relationship between intimate partner sexual violence and posttraumatic stress disorder. Model adjusted for age, income, race, and sexual orientation. Confounder paths are not shown for simplicity. The model was just-identified; therefore, global model fit indices are not reported.
In the second model (see Figure 2), IPSV was a significant positive predictor of TVR moral injury (β = 0.41, p < .001, 95% CI [0.48, 0.97]), and TVR moral injury was a significant positive predictor of PTSD symptoms (β = 0.34, p < .001, 95% CI [0.38, 1.07]). The direct effect of IPSV on PTSD symptoms remained significant after accounting for TVR moral injury (β = 0.19, p < .001, 95% CI [0.48, 0.97]), and the indirect effect of IPSV on PTSD symptoms via TVR moral injury was also significant (β = 0.14, p = .001, 95% CI [0.24, 0.85]). With regard to the assessed covariates, age was a significant negative predictor of TVR moral injury (β = −0.20, p = .02), such that older participants reported lower TVR moral injury, and income was a significant positive predictor of PTSD symptoms (β = 0.16, p = .04), such that participants with a lower income reported significantly higher PTSD symptoms than higher income participants. No other assessed covariates predicted TVR moral injury or PTSD in this model.
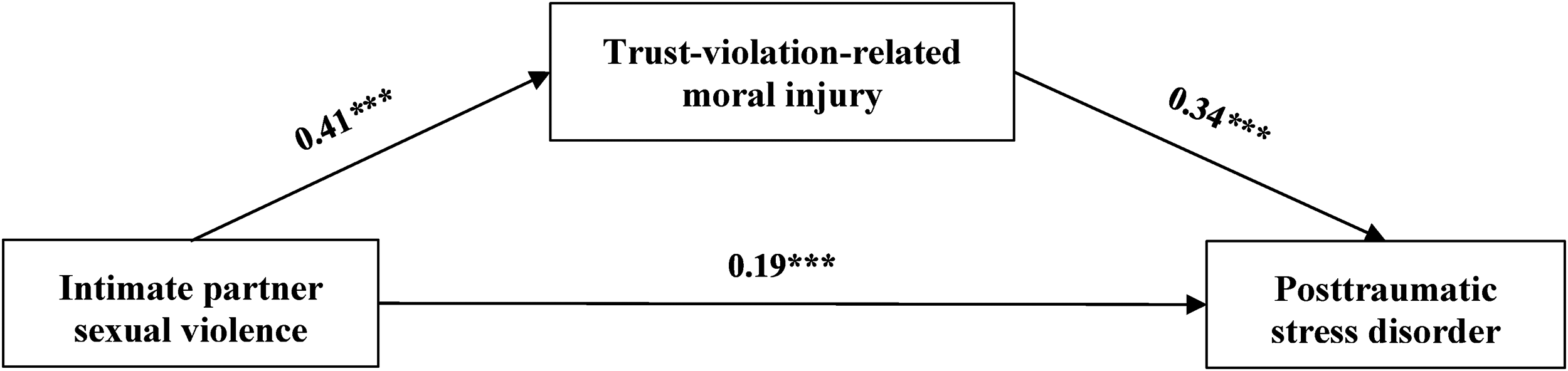
Standardized regression coefficients from a structural equation model testing the indirect effects of trust-violation-related moral injury in the relationship between intimate partner sexual violence and posttraumatic stress disorder. Model adjusted for age, income, race, and sexual orientation. Confounder paths are not shown for simplicity. The model was just-identified; therefore, global model fit indices are not reported.
Open-Ended Responses
The majority of participants responded to each of the three prompts (guilt and shame: 95.8%, n = 136; betrayal: 91.5%, n = 130; internal conflict: 89.4%, n = 127). Response length across the three open-ended items was similar (M = 27.8–30.4 words). Variability was moderate to high (SD = 23.0–25.5), and the median ranged from 20 to 26 words, indicating that most participants provided brief-to-moderate responses, while a subset wrote more lengthy accounts (range = 1–152 words).
Table 4 presents a summary of the key themes and illustrative participant quotations, each addressing distinct facets of moral injury as experienced by IPSV survivors. These themes directly reflect the study's research questions, which sought to explore how IPSV survivors experience moral injury outcomes. Three themes emerged: (a) Self-Betrayal, (b) Self-Blame, and (c) Other-Betrayal, all of which highlight the morally injurious nature of IPSV.
Overview of Theme Names, Central Idea of Each Theme, and an Illustrative Quotation.
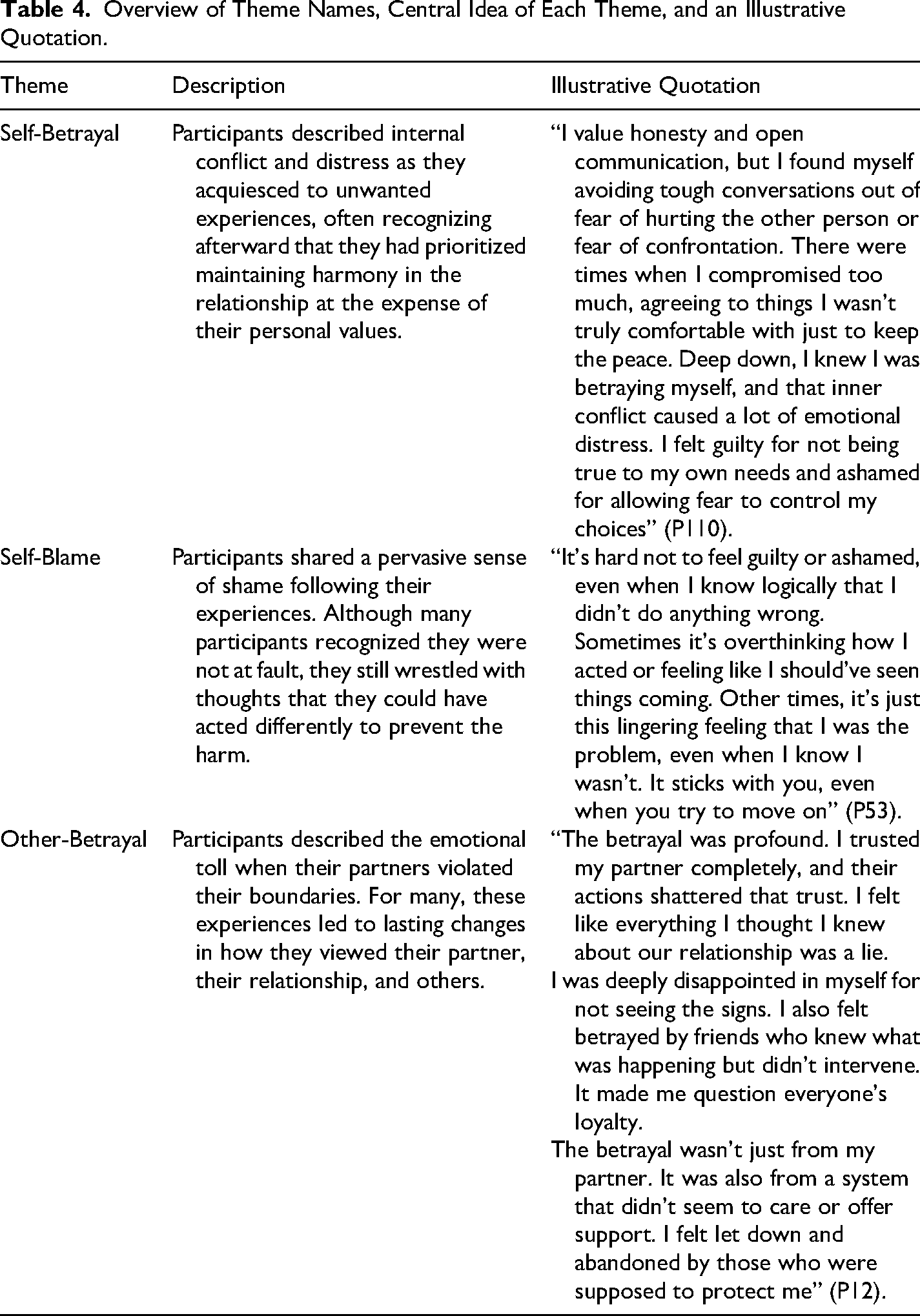
Self-Betrayal. Many survivors described a sense of immense internal conflict that stemmed from remaining silent in order to avoid confrontation and maintain harmony in their relationships. Participants reported that their self-silencing came at the expense of their personal values, leading to a felt sense that they had betrayed themselves. In many cases, this self-betrayal had significant emotional consequences. As Participant 127 explained, There were times when I went against my own values just to avoid confrontation. I’ve always believed in honesty and respect, but at certain times, I kept quiet about things that didn’t sit well with me because I was afraid of rocking the boat. That inner conflict was exhausting and I felt like I was betraying myself just to keep things “okay” on the surface. (P127) There was a time I stayed quiet when I should have spoken up. I ignored my feelings to keep the peace, but it didn’t sit right with me. I wanted to say something, to stand up for myself, but I didn’t. And I still think about it. (P120)
Participants frequently identified fear as the underlying motivation for actions that led to these acts of perceived self-betrayal. These fears included fear of conflict or being harmed: In the moment, I sometimes reacted out of fear or a desire to avoid further harm, which led me to act in ways that didn’t align with my values of assertiveness and self-respect. For instance, I might have gone along with something I didn’t want to do, and afterward, I would feel a deep sense of internal conflict for not having honored my own boundaries or stood up for myself in accordance with what I believe is right. (P109) I told myself I would never put up with something that made me uncomfortable or less than I’m worth. But here I am … putting up with it so to speak. It just is distressing overall that I don’t have the courage to stand up and do something about it. (P85)
Self-Blame. One of the most prominent themes across participant accounts was a deep and enduring sense of shame and self-blame following their experiences of coercion or abuse. As Participant 73 noted, I have been pressured to do things while being intimate that I didn’t want to do, that completely went against my moral beliefs. Experiencing this has made me doubt my partner, has made me doubt myself. I think all the time what the hell is wrong with me? Why do I allow this person to do these things to me? I feel ashamed and even embarrassed due to experiences I have had in my current and previous relationships. (P73) Even though I know logically it wasn't my fault, there are moments when my mind tells me I should [have] done something differently like left sooner, fought harder, spoken up more. The shame creeps in when I start questioning myself wondering if I let it happen in some way even though I know that's not true. (P17)
Several participants also expressed concern about how others might perceive their experiences or judge their responses to the abuse: I felt shame when I first discovered I was a victim of domestic violence, shame that it had happened to me, that I was in that situation, and shame about telling people because I knew many would say why hadn't I said anything sooner and not believe me. (P103)
Other-Betrayal. Participants described a deep sense of betrayal following experiences in which their partners violated their boundaries. These violations disrupted their sense of safety, their perceptions of the relationship, and in many cases, their ability to trust others in the future. The betrayal often left survivors feeling deceived and distressed. Several participants described how their understanding of their partner, and sometimes the relationship itself, shifted dramatically after realizing that someone they trusted had acted in ways that were fundamentally misaligned with their expectations of safety and care. There was a night I said no, and he didn’t stop. I just lay there, unsure whether to fight or let it happen. After, I stared at the ceiling, telling myself it didn’t matter. We were married. But something changed. Every touch felt different. And he acted like nothing happened. I wanted to say something, but I didn’t. I just carried it. (P120)
In some cases, the betrayal extended beyond the individual partner to include friends, institutions, or systems that failed to intervene or provide support. The emotional impact was compounded by a sense of abandonment by others whom they expected to help or protect them. As Participant 12 expressed, The betrayal was profound. I trusted my partner completely, and their actions shattered that trust. I felt like everything I thought I knew about our relationship was a lie … The betrayal wasn’t just from my partner. It was also from a system that didn't seem to care or offer support. I felt let down and abandoned by those who were supposed to protect me. (P12)
Participants also emphasized how the betrayal was not only about the act itself but also about the violation of relational intimacy and the weaponization of vulnerability. Being hurt by someone who knew them so well intensified the emotional damage. When you trust someone—especially a partner—you don’t expect them to hurt you like that. It wasn’t just the physical part; it was the fact that they knew me, knew my vulnerabilities, and still chose to do something so violating. It made me question my ability to trust anyone, not just them. (P17)
Others described how the betrayal shook their understanding of the relationship's foundation, leading them to question the authenticity of what they had once believed was a safe, caring relationship. When someone I was intimate with disregarded my boundaries and engaged in unwanted sexual acts, it felt like a profound violation of trust … This shattered my perception of the person I thought they were and made me question the authenticity of the entire relationship. (P110)
Discussion
This mixed methods study examined moral injury among survivors of IPSV. Drawing on both quantitative data and analysis of open-ended responses, we aimed to better understand how IPSV may function as a PMIE that contributes to psychological distress among survivors of IPSV. Consistent with prior research suggesting that moral injury extends beyond military contexts to survivors of sexual violence (Kanter et al., 2025a; Kanter et al., 2025b; Lathan et al., 2022), our findings indicate that IPSV is highly morally injurious: Over 80% of participants endorsed having experienced a morally injurious event, thereby highlighting the widespread impact of PMIE exposure in this population. As predicted (H1), IPSV was significantly positively associated with SR moral injury, TVR moral injury, and PTSD; both forms of moral injury were positively associated with PTSD (H2); and we observed significant indirect effects of IPSV on PTSD via both SR moral injury and TVR moral injury (H3), suggesting that both dimensions may contribute to psychological distress among IPSV survivors. Notably, of the three types of PMIEs participants could endorse on the MIOS (a personal transgression [i.e., acting or failing to act in accordance with their moral values], witnessing someone else's transgression, or being directly affected by someone else's transgression), a personal transgression was the most frequently endorsed PMIE category (28.7%), despite participants being victims rather than perpetrators of harm. This is consistent with findings from the open-ended responses discussed below and with theoretical accounts of how survivors of high betrayal trauma internalize responsibility for abuse (Freyd, 1996; Freyd & Birrell, 2013).
Three themes emerged from participants’ open-ended responses: Self-Betrayal, Self-Blame, and Other-Betrayal. These themes directly reflect outcomes and dimensions associated with moral injury and provide new and important insights into how moral injury is experienced by survivors of IPSV. In the theme Self-Betrayal, participants described feeling a profound internal conflict arising from their perceived failure to uphold their personal values, often noting that they remained silent or compliant in order to preserve harmony in their relationship. Gilligan (2014) provides a framework for contextualizing these results, arguing that women and girls are forced into a “false choice” between maintaining their voice or preserving their relationships. Gilligan describes this as a “crisis of connection” in which women and girls are compelled to hide their authentic expressions in order to conform to social expectations (2014, p. 92). In doing so, she writes that women and girls often experience a “loss of voice” because speaking up would jeopardize their belonging (Gilligan, 2014, p. 92). In support of Gilligan's position, many survivors in our study reported suppressing themselves in order to maintain their relationship, leading them to feel that they had betrayed themselves. This disorientation from oneself in order to preserve attachment may help explain why SR moral injury was a robust predictor of PTSD in this sample, and why so many survivors reported that a “personal transgression” was the most distressing aspect of the PMIE on the MIOS; many survivors reported that by betraying themselves, they had failed to live up to their moral values.
The theme Self-Blame reflected the guilt and shame experienced by many survivors. Participants commonly expressed regret for not leaving the relationship sooner or for “allowing” abuse to continue, despite often recognizing that the responsibility for the harm did not lie with them. These narratives are consistent with prior research showing that self-blame is a common symptom of experiencing IPV (Lindgren & Renck, 2008) and sexual assault (Peter-Hagene & Ullman, 2016), and further helps explain (a) the importance of SR moral injury in predicting psychological distress within our sample and (b) why so many survivors reported that a “personal transgression” was the most distressing aspect of the PMIE. Self-blame may be pronounced among IPSV survivors due to societal norms of victim blaming. For example, individuals tend to blame survivors of sexual violence more when the survivor knew the person who assaulted them as opposed to when the person who assaulted them was a stranger (Persson & Dhingra, 2020) and evaluate them more negatively if they do not leave their abuser (Halket et al., 2014). This is consistent with research finding that external stigma (i.e., being blamed or judged by others) contributes to internalized stigma, shame, and self-blame among IPV survivors (Willan et al., 2025). Therefore, one important path forward to reducing self-blame among IPSV survivors is through increased societal change such that survivors are not stigmatized, shamed, nor blamed for their morally injurious experiences.
According to Overstreet and Quinn (2013), IPV survivors experience anticipated stigma over concern about what will happen once others know about the partner abuse (e.g., social rejection). This aligns with Litz and Walker's (2025) conception of moral injury in which moral injury is fundamentally about “…a loss of kinship” (p. 264). At the same time, conceptual models of moral injury typically emphasize that SR moral injury results following an experience in which an individual perpetrates or fails to prevent a PMIE (e.g., Litz & Walker, 2025). Yet IPSV survivors are not perpetrators of any moral transgressions. The present findings suggest that SR moral injury need not be precipitated by a perpetration-based transgression per se. In support of this, prior research finds that actual wrongdoing is not necessary for the presence of shame; instead, shame strongly tracks potential devaluation by others (i.e., registering the threat of being devalued or cast out by others; Sznycer et al., 2016) irrespective of whether or not wrongdoing took place (Robertson et al., 2018). Given this research and the findings of the present study, SR moral injury should not be presumed to be solely an antecedent of perpetration-based PMIEs. Instead, SR moral injury may also present in cases wherein the victim of a moral transgression suffers devaluation by others as a result, which is highly relevant in cases of IPV and sexual violence (Overstreet & Quinn, 2013). These findings suggest that SR moral injury should be reconceptualized such that it can develop not merely as a result of perpetration-based PMIEs, but also from the shame and social devaluation that survivors can experience following interpersonal victimization.
In the theme Other-Betrayal, survivors described profound violations of trust that disrupted their fundamental assumptions about intimacy, safety, and their partners’ character. These findings are consistent with Tarzia's (2020) qualitative research, which similarly documented survivors’ accounts of betrayal and “shattered trust” in their partner. In some cases, the betrayal survivors felt was not merely directed at their partner, but also at others (e.g., friends, family) and systems for not protecting them. This broader experience of betrayal reported by survivors may help explain why TVR moral injury, which encompasses anger, disillusionment, and a loss of faith in humanity (Litz & Walker, 2025), was consistently related to IPSV in the present study. In line with BTT (Freyd, 1996), IPSV constitutes a prototypical high betrayal trauma in which the perpetrator is someone the survivor trusted deeply, making the violation of that trust particularly psychologically damaging. Our findings point to the centrality of betrayal as both a defining feature of IPSV and a key pathway through which IPSV contributes to moral injury and psychological distress among survivors.
The present findings also carry important implications for the treatment of moral injury among IPSV survivors. Existing moral injury interventions, such as Adaptive Disclosure (Litz et al., 2016) and Impact of Killing (IOK; Burkman et al., 2022), were developed primarily with military populations in mind and typically emphasize processing acts of commission or omission. That said, Litz and Walker (2025) suggest several methods of recovering from moral injury that may be especially pertinent to IPSV populations, such as obtaining compassionate validation, rebuilding trust in others, increasing one's sense of belonging, and engaging in valued activities within supportive communities.
Cognitive Processing Therapy (CPT; Resick & Schnicke, 1992), which was originally developed to treat PTSD in survivors of sexual assault, directly targets distorted cognitions such as self-blame through cognitive restructuring and has demonstrated large effect sizes in the treatment of PTSD among IPV survivors (Galovski et al., 2022; Shirzadfard Jahromi et al., 2024), suggesting it may also be well-positioned to address SR moral injury. Given that IPSV survivors in the present study described feeling profoundly betrayed not only by their partners but also by others, interventions that target the restoration of relational trust may also be important in this population. Skills Training in Affective and Interpersonal Regulation (STAIR; Cloitre et al., 2020) addresses interpersonal skills and expectations and has proven to be an effective treatment for complex PTSD (Amilhau et al., 2025). Thus, STAIR may prove beneficial for treatment of TVR moral injury. Importantly, both CPT and STAIR can be implemented in group format which, for both theoretical and empirical reasons, may be especially well-suited to treating moral injury (Litz et al., 2016; Litz & Walker, 2025). Trauma-informed approaches that address outcomes arising from both moral injury dimensions among IPV survivors represent a valuable direction for development of new clinical interventions or adaptation of existing interventions (e.g., Adaptive Disclosure; Litz et al., 2016).
Limitations and Future Directions
Several limitations should be noted. First, our cross-sectional design prevents causal conclusions, as longitudinal research would be needed to establish temporal ordering of these relationships and examine how moral injury may develop and change over time following experiences of IPSV. Second, our sample consisted predominantly of heterosexual women (81.7%), which, while reflecting the higher prevalence of IPSV among women (Basile et al., 2022), limits generalizability to individuals of other sexual orientations and gender identities. Of note, the small positive association between sexual minority status and PTSD symptoms observed in our sample highlights the importance of examining how moral injury manifests across identities.
Although our recruitment through Prolific allowed us to reach a diverse sample of IPSV survivors who might not present to clinical settings, future studies should examine these relationships in clinical populations and specialized trauma samples (e.g., domestic violence shelter residents) to better understand how moral injury manifests among those with severe or chronic IPSV histories. This would also help clarify whether the relationships we observed generalize to populations with different patterns of help-seeking behavior. In addition, while research examining quality of responses (including to open-ended survey questions) suggests that Prolific and Cloud Research outperform other platforms (Douglas et al., 2023), this method of collecting qualitative data is much more limited than collecting data from interviews. For example, open-ended survey responses do not permit probing, and as such, they can be limited in their depth (Thomas et al., 2024). As a result, future research should aim to replicate and expand on this research using data from interviews as opposed to survey responses.
Additionally, while participants were instructed to rate their PTSD symptoms in reference to their IPSV experiences, we cannot confirm that responses reflected only distress related to IPSV. This is particularly relevant given that IPSV frequently co-occurs with other forms of IPV (e.g., physical and psychological abuse; Ouellet et al., 2021), meaning that participants’ PTSD symptoms may reflect a combination of victimization experiences rather than IPSV exclusively. This limits our ability to draw firm conclusions about the specificity of the relationship between IPSV and PTSD in the present sample.
One important area for future research is a more detailed examination of how moral injury relates to specific PTSD symptom clusters. Prior work has found that moral injury is most consistently associated with the negative alterations in cognition and mood cluster of PTSD symptoms (Koenig et al., 2020; Levi-Belz et al., 2020). However, both these studies were conducted among military personnel and veterans in the United States and Israel, respectively. Thus, future research examining whether SR and TVR moral injury differentially predict specific PTSD symptom clusters among IPSV survivors would be a valuable extension of the present research. Relatedly, the qualitative themes identified in the present study reflect symptom content that overlaps substantially with this same cluster. Given the well-documented comorbidity between moral injury and PTSD (Hall et al., 2021), it is not possible to determine from the qualitative data alone whether these themes reflect moral injury specifically, PTSD symptomatology, or shared phenomenology common to both. Future research employing structured diagnostic interviews alongside moral injury measures and latent class analyses would be better positioned to disentangle the aforementioned constructs.
Of note, the present study did not assess potentially important dimensions of participants’ IPSV experiences, such as the identity of the perpetrator (e.g., current versus former partner), whether incidents were single or repeated, or the severity or intensity of the abuse. This is a notable limitation given that research consistently finds that greater frequency and severity of IPV exposure are associated with worse psychological outcomes (Dillon et al., 2013; White et al., 2024). Thus, future research should examine how these dimensions of IPSV experiences shape the development and severity of moral injury.
Future research should also explore why specific aspects of IPSV are experienced as morally injurious. Certain coercive experiences (e.g., being forced to perform a sex act with an animal or to have sex in front of one's children) may be perceived by survivors not merely as violations committed against them, but as moral violations they were complicit in perpetrating. According to the theory of dyadic morality, moral judgments are fundamentally structured around a dyad: a moral agent (who causes harm) and a moral patient (who suffers harm), with people perceiving acts as immoral when they fit this template (Schein and Gray, 2018). Therefore, IPSV experiences wherein harm is caused to oneself and others may uniquely predict SR moral injury because survivors may feel complicit in failing to prevent or engaging in acts that caused harm to others. Therefore, future studies should investigate how certain IPSV experiences shape the development and severity of moral injury.
Conclusion
The present study suggests that moral injury is a meaningful construct through which to understand the psychological impact of IPSV. The overwhelming majority of survivors in our sample reported experiencing a morally injurious event, and indirect effects of IPSV on PTSD were observed through both the shame-related and trust-violation-related dimensions of moral injury. Further, survivors in our sample described feelings of self-betrayal, self-blame, and betrayal by others that may help explain these effects. As moral injury continues to be applied beyond military contexts, IPSV should be recognized as an important area for further research and clinical attention.
Footnotes
Ethical Considerations
This study was reviewed and approved by the Institutional Review Board at California State University, San Bernardino (IRB-FY2025-171). All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments.
Consent to Participate
Informed consent was obtained from all individual participants included in the study. All participants reviewed an electronic informed consent form and provided written consent before beginning the survey.
Consent for Publication
No identifying participant information is included in the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data supporting the findings of this study are not publicly available due to the sensitive nature of the topic. Data may be made available upon reasonable request to the corresponding author.