
Abstract
This study assessed how barriers to treatment, stigmatization, and coping strategies may be associated with help-seeking for intimate partner violence (IPV) and whether these characteristics could yield profiles to predict differences in informal and formal help-seeking. Hispanic females (N = 236) completed an online questionnaire assessing IPV, barriers to treatment, stigmatization, coping strategies, and help-seeking behaviors. A Latent Profile Analysis generated four profiles based on background characteristics (e.g., stigmatization) to predict informal and formal help-seeking. The results from pairwise comparison tests indicated significant differences between profile membership and informal and formal help-seeking behaviors for IPV among Hispanic women.
Introduction
Intimate partner violence (IPV), including physical, sexual, and psychological harm within a relationship, is a public health challenge that is particularly prevalent among Hispanic women. Specifically, 37.1% of Hispanic women within the United States report experiencing IPV within their lifetime (Hardesty & Ogolsky, 2020). Help-seeking for IPV, specifically behaviors related to seeking assistance or treatment, is infrequent among Hispanic women (Rizo & Macy, 2011) and usually begins as private strategies that may progress to public strategies (Renner & Hartley, 2022). Private strategies include placating, resisting, and avoiding the perpetrator. However, a “turning point” may occur in which the abuse or its consequences may escalate and thus prompt public strategies, specifically disclosing IPV to an informal (i.e., family, friends) or formal (i.e., health professional, police officer) network (Liang et al., 2005; Renner & Hartley, 2022). Seeking help is crucial as delays can exacerbate the negative sequelae of IPV, particularly regarding physical and psychological health (Cho et al., 2020), in addition to preventing IPV survivors from experiencing the benefits of support. Indeed, a study by Schmidt et al. (2023) notes that informal support may provide emotional aid and informational support, serving as a key facilitator for minoritized IPV survivors in accessing formal resources. The reception of formal treatment or psychological interventions is further associated with improved posttraumatic stress disorder (PTSD) symptoms, quality of life, and overall health for IPV survivors (Cardenas et al., 2024).
Studies primarily conducted among U.S.-residing Hispanic women find that they often do not seek help, delay seeking help, or primarily seek informal support instead of formal treatment (Rizo & Macy, 2011). While 75.3% of Hispanic women report seeking help from informal networks at least once (Cuevas et al., 2014) in comparison to 52% of non-Hispanic women (Kaukinen et al., 2013), rates of formal help-seeking are lower among Hispanic women, as 43% have sought formal treatment for IPV at least once (Cuevas et al., 2014) compared to 52.2% of non-Hispanic women (Ansara & Hindin, 2010). Minority women's reduced help-seeking is often attributable to sociocultural factors and inequities that negatively affect engagement with treatment sources (Padilla-Medina et al., 2022; Robinson et al., 2021). These inhibitors of support-seeking can result in psychological consequences, such as PTSD (Cho et al., 2021) and substance use (Sullivan et al., 2016) from the delay in access to treatment. This is particularly alarming for Hispanic women, as they disproportionately report psychological symptoms (Reyes et al., 2023) and increased alcohol use (Villalba et al., 2025) after an occurrence of IPV. Examination of sociocultural influences that facilitate or inhibit help-seeking is crucial, as these influences can cause victimized Hispanic women to have unequal access to treatment.
Sociocultural Influences of Help-Seeking Behaviors
According to Liang et al.'s theoretical framework, the process of seeking assistance among IPV survivors is impacted by societal, interpersonal, and individual influences (Liang et al., 2005). Societal influences affect the accessibility of support networks by creating barriers to treatment (Liang et al., 2005). Interpersonal factors further impact help-seeking behaviors through affecting how IPV survivors perceive consequences, such as stigmatization, that may occur because of seeking help from a support network (Liang et al., 2005; Overstreet & Quinn, 2016). Moreover, individual influences, such as coping strategies, influence help-seeking behaviors by altering IPV survivors’ perceived abilities to deescalate IPV and seek assistance independently (Liang et al., 2005; Rizo, 2016). Prior theoretical work and literature reviews indicate that these sociocultural influences are impactful on help-seeking behavior across diverse samples of IPV survivors (Liang et al., 2005; Ong et al., 2025; Robinson et al., 2021). However, the Syndemic Model suggests that Hispanics’ health and treatment outcomes may be more likely to be negatively affected following IPV because of the synergistic interactions of various social, economic, and political factors, which together create a greater burden of disease (González-Guarda et al., 2011). In comparison to non-Hispanic women, sociocultural factors (i.e., community attitudes, lack of support, and little information about resources) significantly undermine Hispanic women's abilities to seek assistance following victimization (Schmidt et al., 2023) and should be investigated to determine how these factors disproportionately and collectively prevent help-seeking for IPV among this population.
Barriers to Treatment
Societally, barriers to treatment may inhibit help-seeking behaviors for Hispanic women through altering the feasibility of support (Saint Arnault & O’Halloran, 2016). Indeed, women experience external and internal barriers to treatment, such as low socioeconomic status (SES), shame, and lack of knowledge of resources. External barriers to treatment inhibit help-seeking by limiting women's structural and financial access to resources (Schmidt, 2019). In contrast, internal barriers affect help-seeking by fostering feelings of isolation and hesitancy to disclose experiences of IPV to support networks (Mookerjee et al., 2015; Robinson et al., 2021). Barriers to treatment are especially impactful on help-seeking among Hispanic women as there are culturally specific barriers, such as immigration or language concerns, that contribute to low rates of treatment-seeking behavior (González-Guarda et al., 2011; Rizo & Macy, 2011; Sabina et al., 2015). Assessing how barriers to treatment may be contextualized with other sociocultural factors (i.e., stigma) and differentially predict help-seeking behaviors may elucidate how Hispanic women may navigate treatment for IPV.
Stigmatization
Interpersonally, stigmatization is negatively associated with help-seeking behaviors among Hispanic women as it contributes to fears of social consequences from seeking assistance (Overstreet & Quinn, 2016). Interpersonal forms of stigma may include two types: anticipated stigma (i.e., expectations of discrimination from providers) and internalized stigma (i.e., negative beliefs regarding IPV), both of which negatively impact women's likelihood of seeking assistance (Overstreet & Quinn, 2016). Women survivors of IPV report stigmatization toward their experiences of IPV (Overstreet & Quinn, 2016), characterized by anticipated fears of not being believed or bringing “shame” onto their family that inhibit help-seeking behavior (Bridges et al., 2018). Furthermore, women survivors of IPV describe internalized feelings of shame and guilt toward IPV, as well as perceived responsibility for their history of abuse, which can further dissuade help-seeking efforts (Cardenas, 2023). Although stigma affects survivors of IPV across ethnicities, stigma may be particularly detrimental and prevalent among Hispanic women as they are exposed to more cultural ideologies that delegitimize IPV in comparison to non-Hispanics (Satyen et al., 2019). Specifically, U.S.-residing Hispanic women report community attitudes stemming from their country of origin (i.e., Mexico) that denigrate survivors’ experiences and stigmatization rooted in traditional gender roles that dissuade disclosure and seeking help in favor of preserving familial relationships (Schmidt et al., 2023). These ideologies may contribute to their internalization of detrimental beliefs regarding IPV and anticipation of stigmatization from support networks when seeking help for IPV (Cardenas, 2023; Cardenas, 2022). Investigating stigmatization is vital for Hispanic women as they may anticipate and internalize greater negativity toward IPV, which may have increased consequences for their informal and formal help-seeking behaviors.
Coping Strategies
Individually, coping impacts help-seeking behaviors for Hispanic women by providing perceived control over strategies that address their abusive situation and distress, thereby influencing pathways of seeking assistance (Liang et al., 2005). Coping strategies, known as a set of traits that affect an individual's behavior in response to stress, are often characterized as approach or avoidant (Algorani & Gupta, 2023). Approach coping strategies (i.e., problem-solving, emotion-focused) are associated with greater help-seeking to reduce physical harm or manage psychological distress from IPV (Renner et al., 2024). In contrast, avoidant coping strategies may be linked to less help-seeking as women attempt to avoid thinking about the abuse and focus on distracting themselves (Sere et al., 2021). While the extant literature examining coping strategies among U.S.-residing Hispanic women is limited (Rizo et al., 2017), one study by Weiss et al. (2017) suggests that Hispanic women may utilize coping strategies less often in response to IPV in comparison to non-Hispanic women. Related literature reviews further find that U.S.-residing Latinas’ coping strategies for IPV do not differ from those of other ethnic minority women, but do differ from those of Caucasian women (i.e., increased coping among Latinas; Rizo et al., 2017). Furthermore, immigrant Latinas may have a greater propensity to engage in religious and emotion-focused coping due to cultural values that emphasize faith in God and familial unity (Ozturk et al., 2019). These mixed findings regarding U.S.-residing Hispanic women's utilization of coping strategies following IPV are problematic, as coping helps women manage the abuse, mitigate distress, and seek help (Renner et al., 2024). Evaluating Hispanic women's coping strategies through a sociocultural perspective (i.e., accounting for stigmatization and barriers) may clarify mixed findings and elucidate the role of coping in engagement with support networks when experiencing IPV.
Present Study
Given that Hispanic women residing in the U.S. experience multi-level sociocultural factors that may influence their willingness to seek assistance for IPV (Cardenas, 2023; Mookerjee et al., 2015; Weiss et al., 2017), identifying the relationships between these factors and help-seeking behaviors may provide insight into how these variables may affect informal and formal help-seeking patterns. Prior research has often used variable-centered approaches (e.g., regression) to identify the influence of certain variables on help-seeking, yet these approaches assume the same parameters for the population. In a person-centered approach (e.g., latent profile analysis [LPA]), one can identify distinct homogeneous groups with their own parameters based on response profiles across various indicators. This provides a more holistic view of subgroups of individuals who may differ in their help-seeking behaviors. Thus, the present study used LPA to construct profiles with the following indicators: barriers to treatment, stigmatization toward formal help-seeking, and coping strategies. Within the present study, we also assessed whether profile membership predicted seeking informal and formal help for IPV among U.S.-residing Hispanic women. Based on the extant IPV and help-seeking literature within Hispanic women, the authors hypothesized:
Method
Participants
A total of 574 participants were invited through Prolific to take part in the present study. Inclusion criteria for the present study consisted of participants being female, self-identifying as Hispanic/Latina, having experienced any form of IPV in their lifetime (i.e., physical, psychological, sexual victimization, and experiences of injury from a partner), English-speaking, and residing within the United States. Among the 574 invited participants, 387 participants enrolled in the present study. Exclusion criteria consisted of not passing two or more of the nine attention checks (n = 12), not completing the survey (n = 31), or withdrawing from the study (n = 2). Furthermore, data from seven participants were removed due to failure to meet the demographic eligibility criteria (i.e., Hispanic, female) at the time of the study. Moreover, due to the focus on help-seeking for IPV, data from 99 participants who did not report any experiences of IPV (i.e., psychological aggression, physical assault, sexual coercion, injury by a partner) or exclusively perpetration were removed. The final sample consisted of 236 Latina participants who completed the survey (Mage = 32.24, SD = 10.03).
Procedure
University Institutional Review Board approval was obtained prior to data collection, which took place from September 2023 to March 2024. All participants provided informed consent. Participants were recruited via Prolific, a secure web-based recruiting system where they completed a 5-min screener in English. Upon completion of the screener, potential participants received $1.00, and those who met the inclusion criteria in the screener were invited to participate in the online survey that was English-only. Those who completed the survey were then compensated with $12.00, debriefed, and provided with national resources for trauma and alcohol usage.
Measurement
Sociodemographic Variables
A sociodemographic questionnaire assessed participants’ age, sex at birth, ethnicity, marital status, education level, and household income. Ethnicity was separated into Mexican or Mexican American, Cuban, Puerto Rican, South American, Central American, Spanish, and other ethnicity. Although there are nuances relating to geography and language when using the terms Hispanic and Latinx, both of these groups were included in the study, and the term Hispanic is used for simplicity. Marital status was categorized into single, married, divorced, widowed, living with an intimate partner, in a relationship, and separated. Education level was separated into less than high school, high school graduate, and some or completed college education. Household income was categorized into annual income.
Intimate Partner Violence
The Conflict Tactics Scale–Revised Short Form (Straus & Douglas, 2004) is a 20-item scale that assesses different forms of IPV in an individual's past or current relationship history (i.e., Physical Assault, Psychological Aggression, Injury, Sexual Coercion). Items were answered on a 7-point Likert scale from 0 (this has never happened before) to 6 (more than 20 times), where higher scores indicated greater frequency of lifetime experiences of relationship violence. Subscale scores were obtained by calculating the sum of midpoint scores per item within each subscale. The physical assault, psychological aggression, sexual coercion, and injury victimization subscales were utilized to assess the history of abuse. This scale was used as a descriptive variable when constructing participant characteristics for the study's sample. Per Straus & Douglas (2004), reliability estimates (e.g., Cronbach's alpha) were not calculated, given the absence of total score and two items per subscale within the scale. This measure demonstrated acceptable construct validity with couple conflict (r = .08–.16) and violent approval in prior studies (r = .11–.17; Straus & Douglas, 2004).
Barriers to Help-Seeking
The Barriers to Help-Seeking–Trauma Version (Saint Arnault & O’Halloran, 2016; Saint Arnault & Zonp, 2022) is a 24-item survey that assessed different types of barriers (i.e., structural, internal) that are reported when seeking assistance for IPV. Structural barriers included items from the following subscales: unavailability/unhelpfulness, financial concerns, discrimination, and external constraints. Items included “I am worried that if others discover my health problems or my situation, I could lose housing, security, or my children.” Internal barriers included items from the following subscales: shame, frozen/confused, and management beliefs. Items included “I thought my situation was too personal or wanted to keep it private.” Items were answered on a 4-point Likert scale from 1 (did not influence me) to 4 (strongly influenced me), where higher scores indicated more barriers that influenced an individual's decision of whether or not to seek help for IPV. Subscale scores were obtained by calculating the sum for items within each subscale. This scale was used as an independent variable when constructing background characteristics for the LPA. Furthermore, this measure demonstrated acceptable reliability for all subscales in the present study (α = .87–.88), similar to past studies (α = .87). This scale has demonstrated convergent validity with similar scales (r > .23; Beliefs Towards Mental Illness; Saint Arnault & Zonp, 2022).
Stigmatization Toward Seeking Help
The Attitudes About Seeking Formal Help (Cardenas, 2023) is an 8-item scale that assessed attitudes toward seeking formal help (i.e., professionals) among interpersonal violence survivors. Items are answered on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree), where higher scores indicate greater negative attitudes toward obtaining formal help. Subscale scores were obtained by calculating the mean for items within each subscale.
This scale was used as an independent variable when constructing background characteristics for the LPA. Furthermore, this scale has demonstrated acceptable reliability in the present study (α = .76) similar to that of past studies (α = .75; Cardenas, 2023). Furthermore, this scale has demonstrated construct validity with fatalism (r = .30, p < .001) and traditional gender role attitudes regarding family (r = .48, p < .001) and romantic relationships (r = .31, p < .001; Cardenas, 2023).
Coping Strategies
The Brief COPE (Carver, 1997) is a 28-item scale that measures 14 distinct coping strategies for stress that fall into three categories: problem-solving, emotion-focused, and avoidant (Dias et al., 2012). In the present study, subscales derived from Carver (1997) were categorized as follows (Mehrtash, 2023): problem-solving (i.e., active coping, use of informational support, positive reframing, planning), emotion-focused (i.e., emotional support, venting, humor, acceptance, self-blame, religion), and avoidant (i.e., self-distraction, substance use, denial, and behavioral disengagement). Items were answered on a 4-point Likert scale from 0 (I haven’t been doing this at all) to 3 (I’ve been doing this a lot), where higher scores indicated greater engagement in problem-solving, emotion-focused, and/or avoidant coping strategies. Subscale scores were obtained by calculating the mean for items within each subscale. This scale has demonstrated adequate reliability in the present study (α = .72–.85) similar to those found in other studies (α = .75–.91). Furthermore, this measure has demonstrated test–retest reliability (ICC = .72) and criterion validity between maladaptive coping strategies and changes in caregiver burden (r = .32–.33) and depressive symptoms (r = .59; DeDios-Stern et al., 2017).
Help-Seeking Behaviors
The present study assessed lifetime utilization of support networks (i.e., formal, informal) for experiences of IPV through a 13-item survey adapted and modified from prior literature (Brabeck & Guzman, 2009). To assess formal help-seeking, participants were asked, “When you experienced Intimate Partner Violence, did you ever seek help from an agency or service in regard to the abuse in your relationship?” and provided options of formal resources in which they indicated whether they had used each resource by selecting (1) yes or (0) no. To assess informal help-seeking, participants were asked, “When you experienced Intimate Partner Violence, did you ever talk about the abuse with anyone?” and were provided options of informal resources in which they indicated whether they had used each resource by selecting 1 (yes) or 0 (no). Higher scores reflected greater utilization of help-seeking resources for IPV. Subscale scores were obtained by calculating the sum for items within each subscale. This measure demonstrated acceptable reliability (α = .70) in the present study.
Approach to Analyses
Descriptive analyses yielded participant characteristics (see Table 1), and skewness, kurtosis, and bivariate correlations for all study variables (see Table 2). Furthermore, Mplus Version 8.11 was utilized to generate profiles based on participant background characteristics (i.e., barriers, stigma, coping strategies). Two through eight profile solutions were conducted in which model fit (see Table 3) was determined by comparing Akaike information criterion (AIC), Bayesian information criterion (BIC), and entropy. Once researchers identified the number of profiles that yielded the best-fitting model, profile membership was then used to predict formal and informal help-seeking behaviors for IPV, utilizing pairwise comparison tests while controlling for marital status and SES using the three-step BCH procedure. 1
Descriptive of Sample.
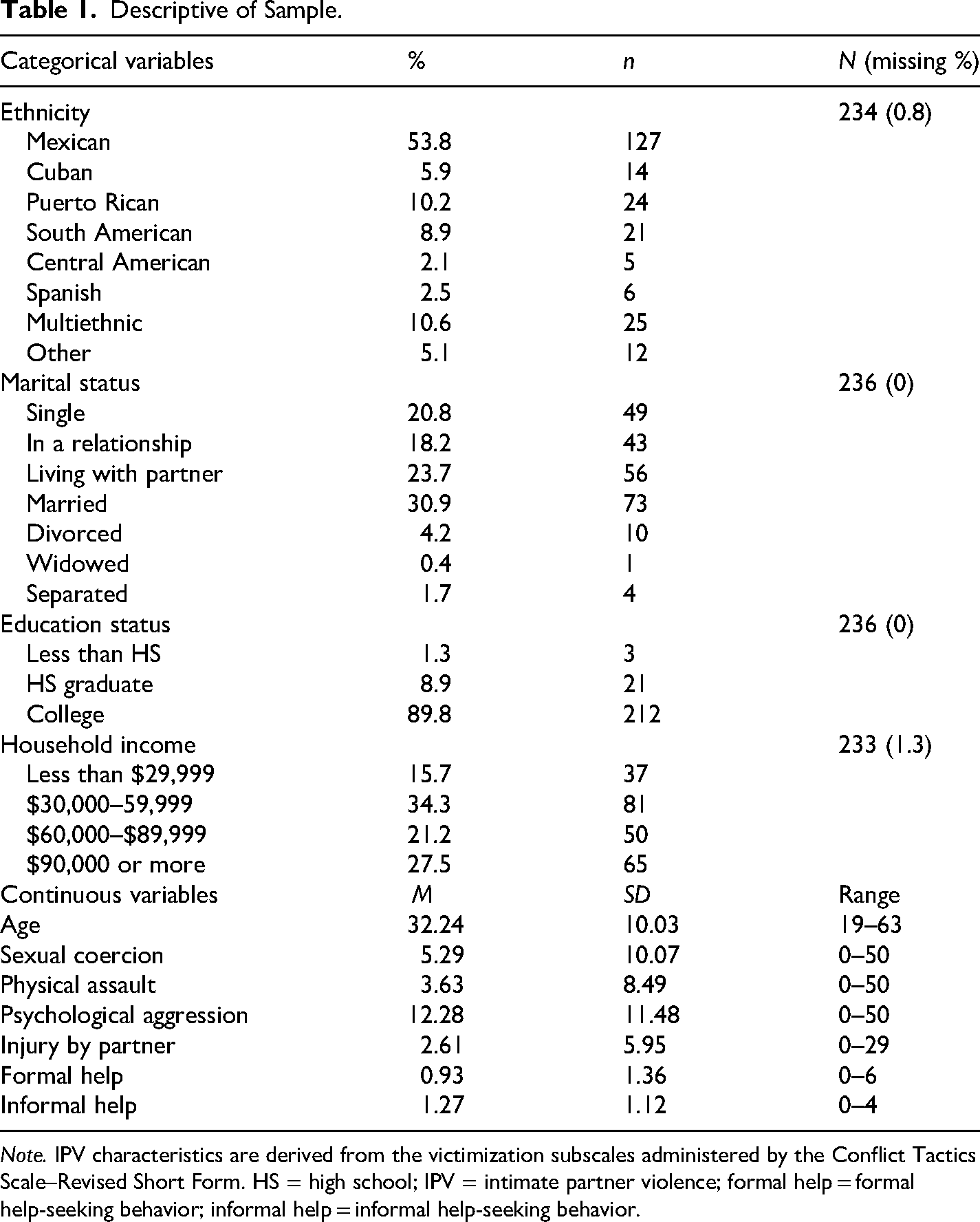
Note. IPV characteristics are derived from the victimization subscales administered by the Conflict Tactics Scale–Revised Short Form. HS = high school; IPV = intimate partner violence; formal help = formal help-seeking behavior; informal help = informal help-seeking behavior.
Correlation Matrix, Means, Standard Deviations, Skewness, and Kurtosis.
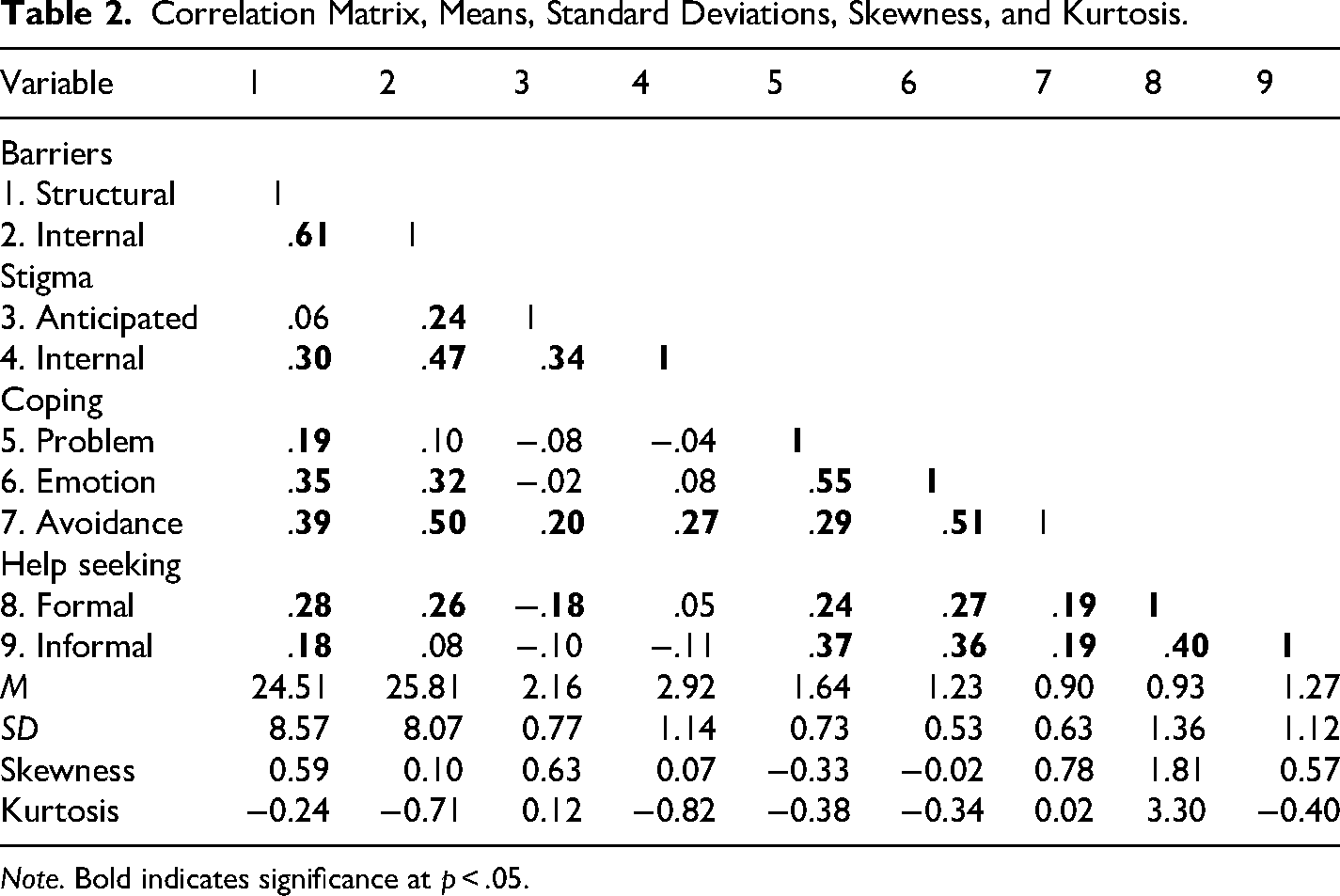
Note. Bold indicates significance at p < .05.
Model Fit Statistics.
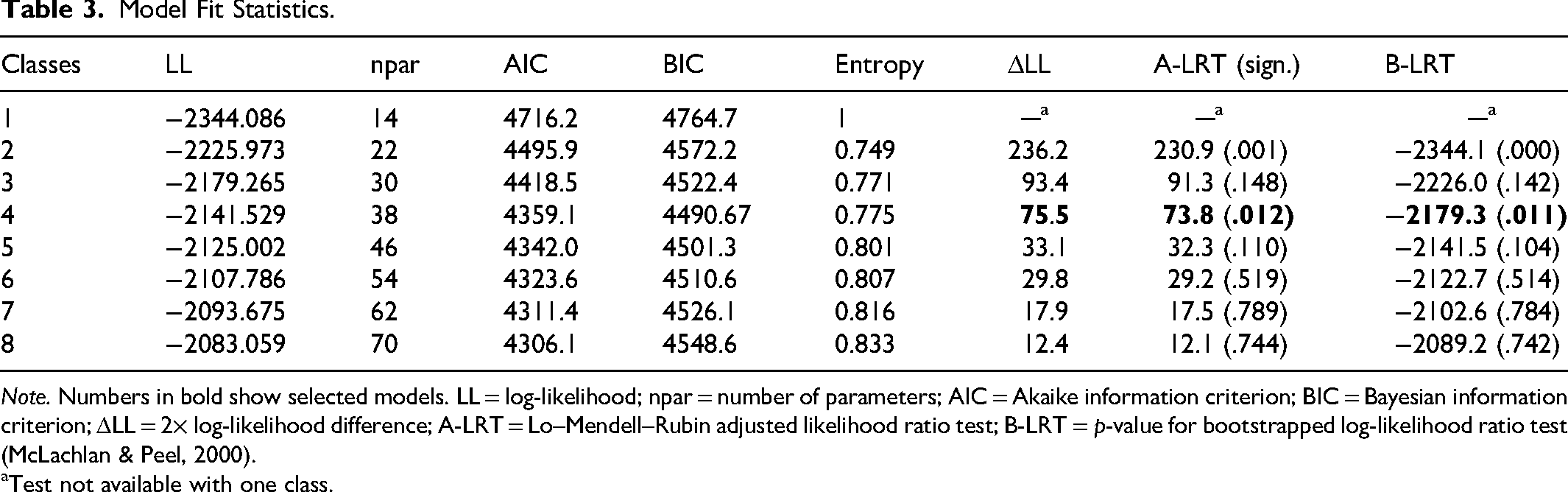
Note. Numbers in bold show selected models. LL = log-likelihood; npar = number of parameters; AIC = Akaike information criterion; BIC = Bayesian information criterion; ΔLL = 2× log-likelihood difference; A-LRT = Lo–Mendell–Rubin adjusted likelihood ratio test; B-LRT = p-value for bootstrapped log-likelihood ratio test (McLachlan & Peel, 2000).
Test not available with one class.
Results
Descriptive Analyses
Missing data analyses were conducted on SPSS for all of the independent variables in which data were missing completely at random per missing data analysis patterns. All variables had less than 6% missing data; thus, the authors created five imputed datasets, which sufficed given the level of missingness (Graham et al., 2007). Results for subsequent analyses were conducted using the aggregate of the five imputed data sets. Participant characteristics were assessed through descriptive statistics (see Table 1) in which skewness and kurtosis for all variables fell within the recommended range of |SK| < 2 and |KU| < 7 (Kim, 2013; see Table 2). Participants in the study were 100% female and Hispanic with a mean age of 32.24 (SD = 10.03). Within this sample, 97.5% of participants indicated having experienced psychological aggression, 49.2% experienced physical assault, 38.6% experienced injury by a partner, and 51.7% experienced sexual coercion within their lifetime. Additionally, participants were more likely to report both victimization and perpetration (93.2%) than exclusively victimization (6.8%). The lifetime frequency of IPV victimization within each profile can be found in Figure 1. Regarding support and services utilized by this sample of Hispanic women in response to IPV, 45.8% sought one or more formal services for help, and 69.1% had sought support from one or more informal networks. Formal and informal help-seeking behaviors within each profile can be found in Figure 2. Bivariate correlations for barriers to help-seeking, stigmatization, coping strategies, and help-seeking behaviors can be found in Table 2.
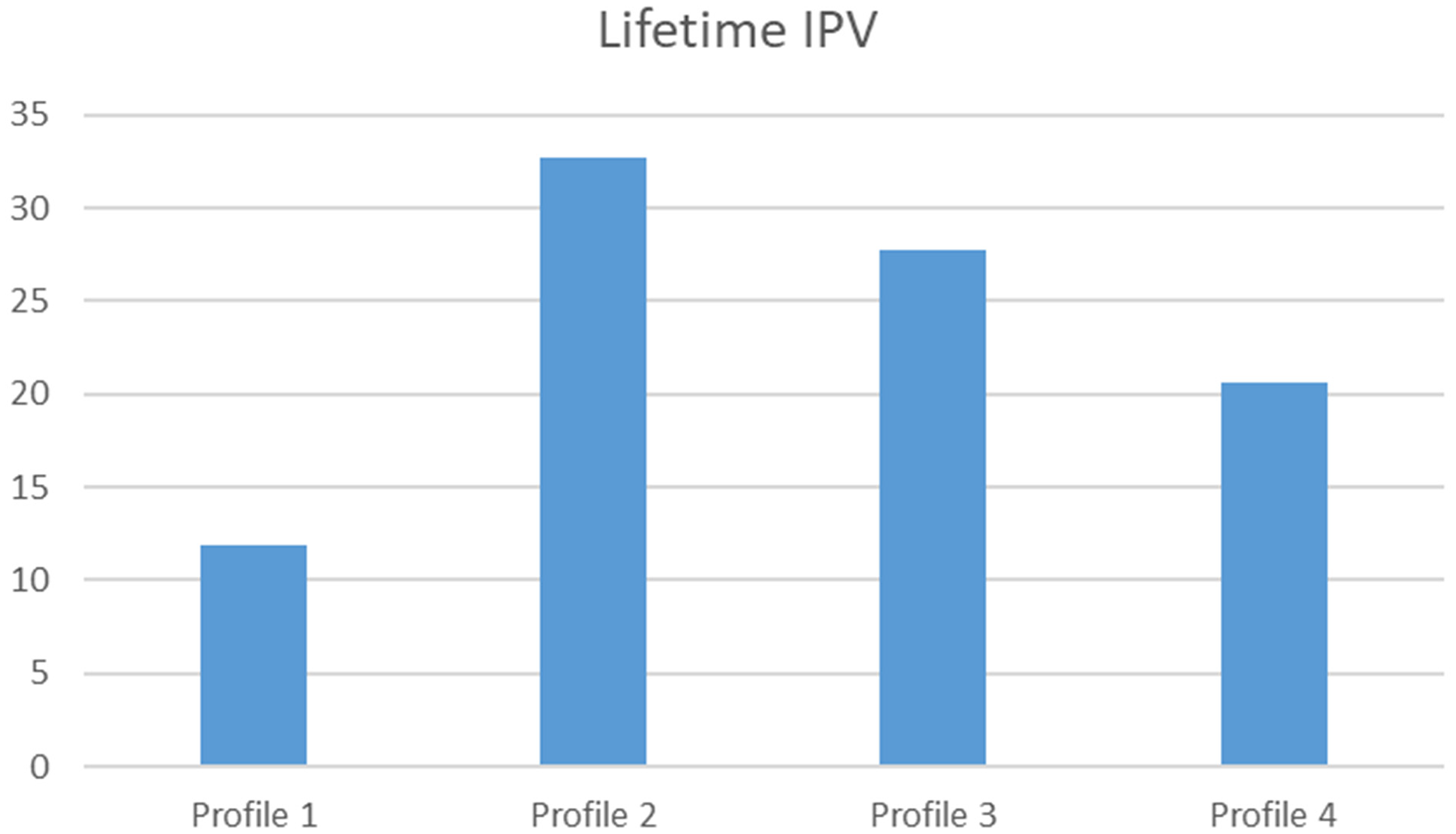
Average of lifetime frequency of intimate partner violence (IPV) victimization by profile.
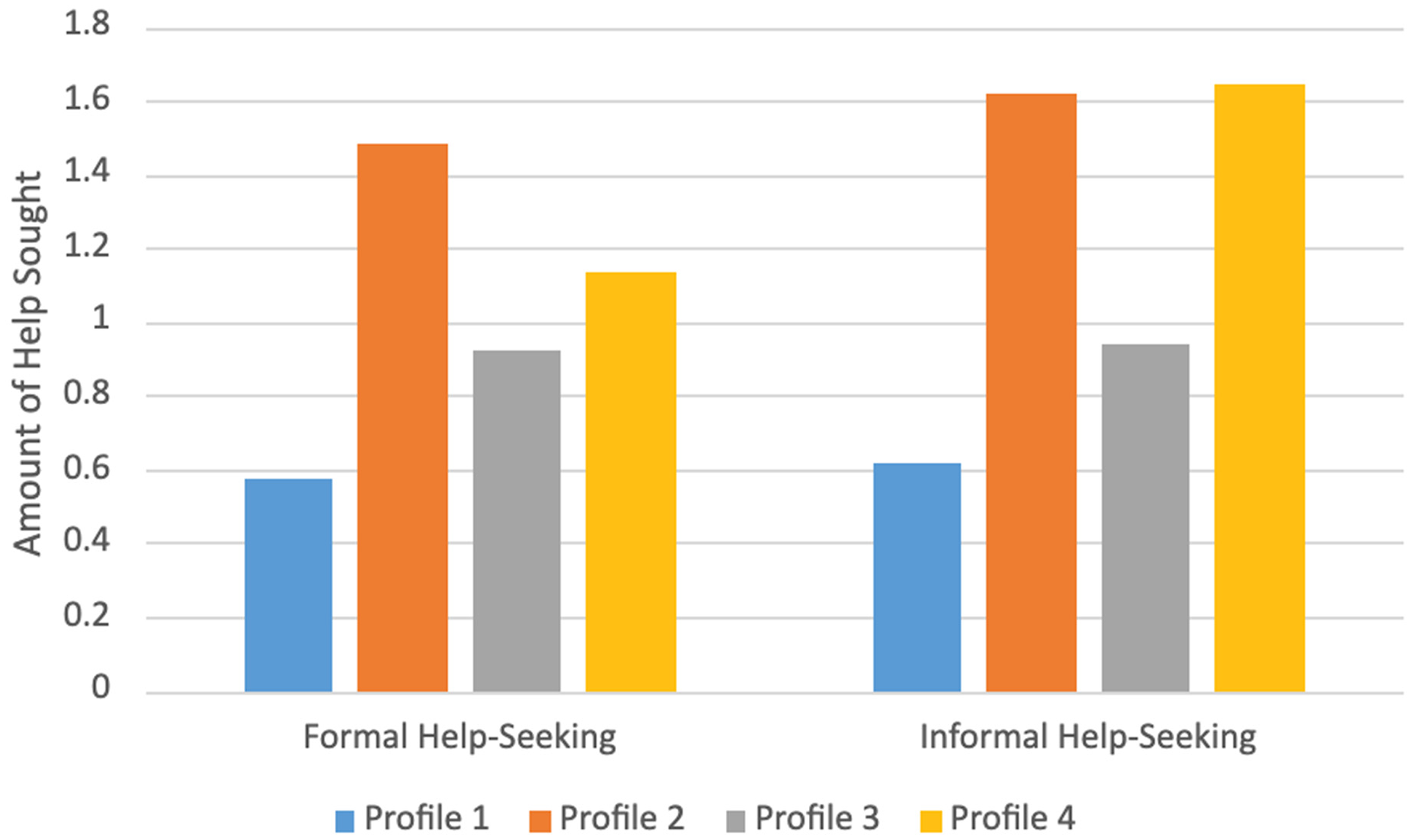
Help-seeking by profile.
Latent Profile Analysis
Mplus Version 8.11 (Muthen & Muthen, 2025) was used to generate profiles based on the type of perceived barriers (i.e., structural, internal), stigma (i.e., anticipated, internalized), and participant coping strategies (i.e., problem, emotion, avoidance). Several model fit statistics were used to identify the best solution when iteratively evaluating two- through nine-profile solutions. Smaller AIC and BIC (Ferguson et al., 2020) and high entropy values (>.80; Tein et al., 2013), revealing the accuracy of profile assignment, were considered when identifying the best solution. Additionally, neighboring profile models were also compared using bootstrapped likelihood ratio test (LRT; Nylund et al., 2007) and Lo–Mendell–Rubin adjusted LRT. Significant LRT indices indicate that the more parsimonious model with k profiles fits better than one with fewer profiles (k-1). Furthermore, profile interpretability and theoretical alignment were also considered when selecting the final profile. The four-profile solution seemed to be the best-fitting model, given that there was an attenuation of AIC (Δ 59.47) and BIC (Δ 31.762) at the four-profile solution. The lowest AIC and BIC values were observed at the eight- (4306.118) and four-profile (4490.683) solutions, respectively. Entropy values continued to increase at the eight-profile solution. When looking at the LRT, only the two- and four-profile solutions were statistically significant. Models that produced small profiles, <5%, were not considered, given that this reduces power and affects the precision of the model (Ferguson et al., 2020).
When visually examining the three- to five-profile solution, the three-profile solution reflected profiles that differed in their levels, with one profile stacked on top of the other, and were qualitatively different from each other. Extraction of the additional profile in the four-profile solution revealed a new profile that was qualitatively different than all other profiles. The five-profile solution did not differ characteristically from the four-profile solution, such that the extraction of the new profile only differed in level (i.e., a profile split into two new profiles only differed by the level on indicators). Given both statistical criteria and interpretability, the four-profile solution was selected for subsequent analyses.
Standardized participant composite characteristics for each of the profiles are depicted in Figure 3. Low, medium, and high levels of the variables were arbitrarily constructed based on average scores for each of the variables in relation to their observed mean within the sample. Profile 1 (n = 39) was characterized by relatively low levels of structural and internal barriers (−1 to −1.5 SD), moderate levels of anticipated and internalized stigma (0 to −0.5 SD), and low levels of problem, emotion, and avoidance coping (−1.5 to −2 SD). Profile 2 (n = 40) was characterized by high levels of structural and internal barriers (+1.5 to +2 SD), moderate levels of anticipated and internalized stigma (+0.5 to +1 SD), and moderate to high levels of problem-solving, emotion-focused, and avoidance coping (+0.75 to +2 SD). Profile 3 (n = 86) was characterized by consistently moderate levels of structural and internal barriers, anticipated and internalized stigma, and problem-solving, emotion-focused, coping, and avoidance coping. Profile 4 (n = 69) was characterized by moderately low levels of structural and internal barriers (−0.5 to −1 SD), moderate levels of anticipated and internalized stigma (−0.5 to −1 SD), and moderate levels of problem-solving, avoidance coping, and emotion-focused coping (−0.25 to +1 SD).
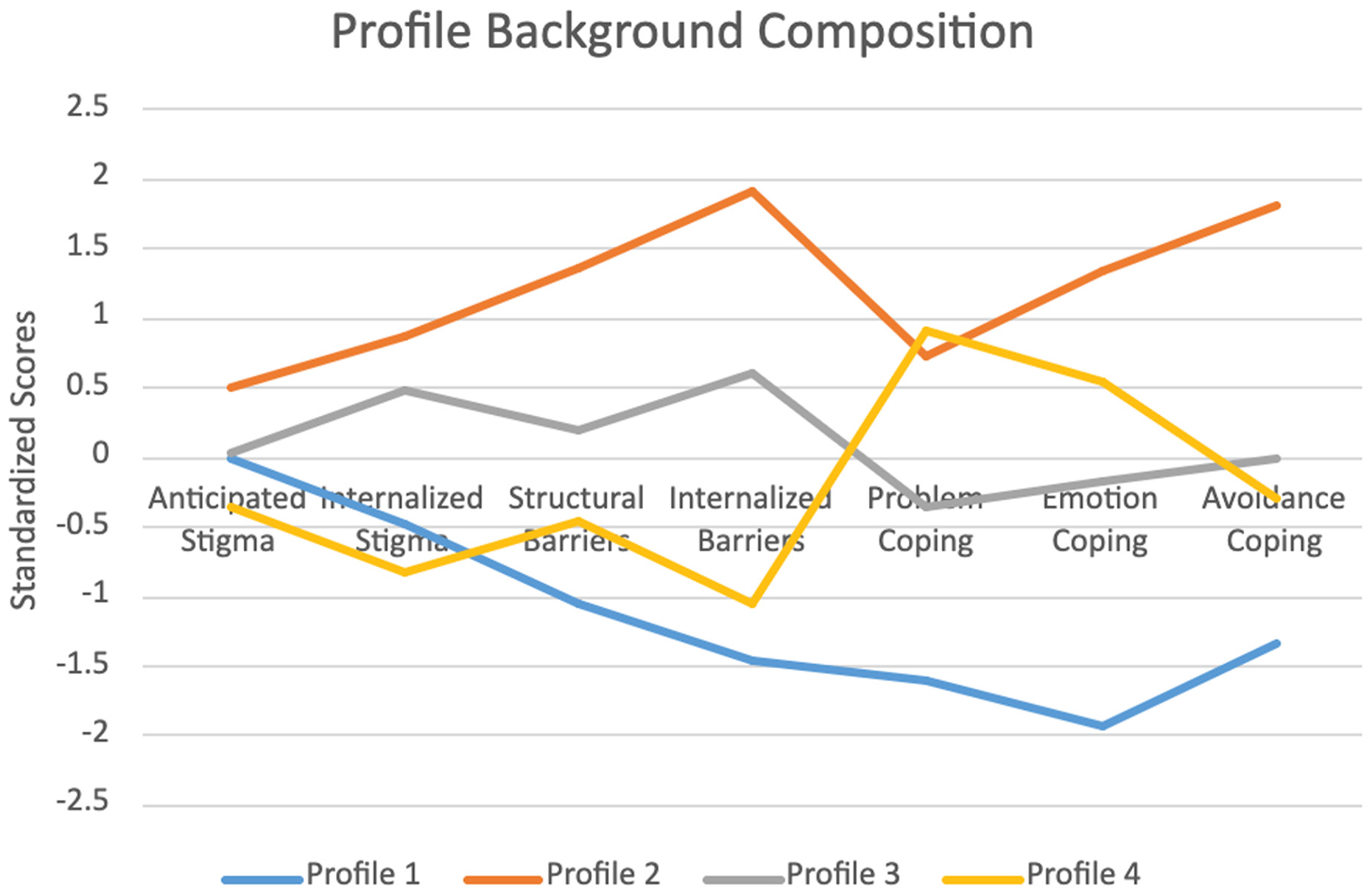
Profile background characteristics.
Formal Help-Seeking
When controlling for marital status and SES, there were statistically significant differences between profile membership on formal help-seeking. Those in Profile 1 (
Informal Help-Seeking
When controlling for marital status and SES, there were also statistically significant differences between profile membership on informal help-seeking. Those in Profile 1 (
Discussion
The present study assessed how perceived barriers (i.e., structural, internal), stigma (i.e., anticipated, internalized), and coping strategies (i.e., problem-solving, emotion-focused, avoidance) may be associated with formal and informal help-seeking for IPV. Moreover, we assessed whether these background characteristics could be categorized into distinct profiles and associated with differences in formal and informal help-seeking behaviors. Overall, these hypotheses were supported, such that barriers, stigma, and coping strategies were associated with formal and informal help-seeking. Furthermore, these background characteristics were used to create four distinct profiles that predicted differences in formal and informal help-seeking for IPV. Across profiles, coping strategies and barriers to treatment differed significantly; however, stigmatization was moderate and demonstrated the least variability for all profiles.
Notably, four profiles were identified in which they varied significantly on barriers and coping strategies, and less so on stigma. Profile 1 was characterized by moderate stigma, low perceived barriers, and low reported use of coping strategies. This could signal a group of women who are not actively engaged in help-seeking and thus might not be aware of potential obstacles. Profile 2 was characterized by high amounts of stigma, perceived barriers, and high reported use of various coping skills, reflecting a group that is highly engaged in seeking assistance, but who struggles based on stigma and various barriers to receiving support or assistance. Profile 3 was characterized by moderate levels of stigma, perceived barriers, and moderate reported use of various coping skills, indicating a group that may be ambivalent or may only seek help in certain situations. Profile 4 was characterized by moderately low amounts of stigma and perceived barriers, but moderate to high reported use of various coping strategies, indicating that this consists of a group of women who actively utilize various forms of help-seeking outlets and thus may have success navigating formal and informal help systems. Across formal and informal help-seeking behavior, Hispanic women in Profile 1 consistently reported the fewest utilization of help-seeking resources, and those in Profile 4 utilized the most help-seeking resources.
Formal Help-Seeking
Those in Profile 1 displayed the lowest propensity to utilize formal treatment for IPV when compared to those in Profiles 2, 3, and 4, potentially because Profile 1 was uniquely characterized, in part, by fewer coping skills in comparison to all other profiles. However, this result is unexpected given Profile 1 reported the lowest barriers to treatment and moderate levels of stigma, while those in the remaining three profiles specifically reported slightly elevated to greater levels of barriers to treatment. While this is congruent with prior studies suggesting that higher levels of coping strategies, particularly problem-solving (Shannon et al., 2006), are associated with utilization of formal IPV treatment, this finding stands in contrast to extant literature demonstrating less formal treatment seeking for Hispanic women experiencing stigmatization and barriers (Mejia, 2023). When looking at these variables holistically, coping skills may allow Hispanic women to seek more formal help, in which they are equipped to navigate barriers and overcome stigmatization when engaging with systems of treatment. Indeed, coping strategies may help women regulate their emotions and take action when experiencing IPV (Lazarus, 1993; Shannon et al., 2006). This facilitatory effect of coping on utilization of formal help-seeking may extend to Hispanic women who have experienced extensive IPV, as those in Profiles 2, 3, and 4 reported greater lifetime frequencies of IPV in comparison to Profile 1. Indeed, this finding could contribute to extant facilitators of formal help-seeking in the face of severe violence (Schmidt et al., 2023). Given that another profile difference appeared—such that Profile 3 sought less formal help than Profile 2—it is plausible that the extant interpretation still applies, given that Profile 3 reported greater engagement in coping strategies than Profile 2. Overall, our results may indicate that engagement in coping may provide IPV survivors with strategies that enable greater utilization of help-seeking resources in the face of barriers or stigmatizing norms toward seeking assistance for IPV.
Informal Help-Seeking
Those in Profiles 1 and 3 had lower propensities to utilize informal support for IPV when compared to Profiles 2 and 4, likely due to the moderate to high levels across all coping strategies within the latter profiles. Past literature supports our finding as women are shown to utilize informal support to aid with their attempts to cope with the abuse (Ozturk et al., 2019; Puente-Martinez et al., 2023). Furthermore, women seek resources that align with their coping strategies, such that those who utilize approach coping (i.e., problem-solving, emotion-focused) often seek resources that can provide solutions or support (Renner et al., 2024). This pattern further appears within ethnic minority women as they seek more informal support from family and friends (Rizo & Macy, 2011), often to cope with and survive IPV (Ozturk et al., 2019). Thus, Hispanic women in Profiles 2 and 4 may have utilized more informal support for experiences of IPV, as it complements their greater utilization of problem-solving and emotion-focused coping strategies.
While Profiles 2 and 4 also reported moderate stigmatization, this factor was relatively similar across profiles, which may indicate that coping strategies are the distinguishing variable that primarily dictates utilization of informal resources among Hispanic IPV survivors. Given the greater barriers yet also increased utilization of informal resources in Profiles 2 and 4, these findings may also suggest that coping strategies may facilitate help-seeking in the face of extensive barriers—similar to formal help-seeking. Conversely, it may also be possible that Hispanic women who seek less help perceive fewer barriers due to their minimal experiences navigating support systems, as shown in Profiles 1 and 3. However, future research should continue to investigate whether Hispanic women anticipate more barriers as they utilize informal support and formal services.
Implications for Policy and Intervention
Findings from the present study elucidate different mechanisms by which Hispanic women may utilize or encounter when seeking help for IPV victimization. Stigma seemed to be a common occurrence in all profiles, which is consistent with past literature noting greater exposure to societal and cultural stigma among Latina and other ethnic minority women IPV survivors (Hernandez et al., 2024; Satyen et al., 2019). Stigmatization may be addressed by teaching service providers how to utilize trauma-informed and compassionate approaches (i.e., openness, gentleness) to increase survivors’ comfort level with IPV disclosure and further help-seeking (Ravi et al., 2022). Findings related to barriers are what stand in contrast, such that those in the profiles who were most likely to seek help reported the greatest extent of barriers, revealing the cumbersome nature of these systems. Barriers may be mitigated in such systems by educating informal supports on how to provide encouragement toward individuals experiencing IPV, while increasing the accessibility of services and providers’ knowledge of how IPV manifests across cultures (Ravi et al., 2022). Furthermore, those in profiles who had greater use of coping strategies displayed greater informal and formal help-seeking. Interventions for IPV survivors should address fortifying coping skills and increasing coping self-efficacy to promote emotional regulation and problem-solving, which may help prevent revictimization (Ortega Pacheco et al., 2024). This is particularly important as extant reviews (Cardenas et al., 2024) seem to indicate that interventions among Hispanic women IPV survivors have yet to focus on coping strategies and their role in facilitating treatment engagement.
Limitations
The present study contains several notable limitations. While there is no current consensus on the minimum required sample size for LPA (Daumiller et al., 2023), our profile sizes were small (n < 50), which may have resulted in not capturing more “rare” patterns (Nylund-Gibson & Choi, 2018) of help-seeking behavior within the profiles. Moreover, this study was cross-sectional, so causal inferences cannot be made about profile membership and help-seeking behavior. In addition, this study did not assess the influence of different types of IPV (i.e., physical, sexual, psychological) on profile membership, which may potentially affect Hispanic women's recognition of violence (Rojas-Solís & Romero-Méndez, 2022; Villagrán et al., 2024) and future help-seeking behavior. Lastly, the present study lacks subgroup variability and in-depth analysis of cultural concepts, as Hispanic women were analyzed as an aggregated group without differentiation by nationality, and inter- and intrapersonal constructs were predominant. Future research should address these limitations by examining within-group differences in help-seeking across national subgroups among Latinas using this four-profile solution and through the incorporation of additional sociocultural factors (e.g., community norms, cultural values) that were unmeasured in the present study.
Conclusions
The present study extends our limited understanding of how sociocultural factors across multiple levels (i.e., societal, interpersonal, and individual) may culminate to differentially affect formal and informal help-seeking for IPV among Hispanic women. Consistent with past research (Renner et al., 2024), those in profiles who scored high in coping strategies displayed the greatest amount of help-seeking behaviors. However, contrary to prior literature (Overstreet & Quinn, 2016; Rizo & Macy, 2011), profiles who also scored high in barriers to treatment and stigmatization displayed the greatest amount of help-seeking behaviors, potentially due to their elevated rates of coping (Shannon et al., 2006). Through understanding the influence that multi-level factors have on Hispanic women's help-seeking, our findings may inform community-based prevention efforts that aim to reduce IPV among minority communities through targeting individual and interpersonal risk factors to improve accessibility of support (Mancini et al., 2006).
Given that profiles with elevated rates of any coping strategy sought more help, this suggests a need for research to investigate how engagement with coping across maladaptive and adaptive forms may facilitate help-seeking behavior. This is particularly relevant because profiles characterized by higher levels of coping strategies—despite experiencing greater barriers and stigmatization—utilized more help-seeking resources than profiles with lower barriers, comparable stigma, and fewer coping strategies. Furthermore, prior research has suggested an effect of coping self-efficacy on help-seeking during active abuse (Shah et al., 2024), which may indicate a benefit for prospective studies to assess the role of coping self-efficacy across various coping strategies on help-seeking for lifetime IPV. Overall, these findings support the utility of sociocultural theoretical frameworks when examining help-seeking, as our results highlight the interrelationships between barriers to treatment, stigmatization, and coping strategies in relation to formal and informal help-seeking behavior among Hispanic IPV survivors.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.