
Abstract
This is the case of a 13-year-old Hispanic boy (34.2 kg, 1.14 m2) who had achieved stable therapeutic levels on voriconazole who later experienced levels reported as ‘none detected’ after the initiation of tube feeds. This case outlines the temporal relationship of the effect of tube feeds on voriconazole serum levels. Based on this information, voriconazole suspension should not be prescribed to patients also receiving supplemental enteral nutrition. In absence of formal animal or human pharmacokinetic studies, it is the recommendation of the author to separate this combination and to be very vigilant about checking serum voriconazole levels in patients on voriconazole suspension and enteral nutrition supplements.
Introduction
Recipients of Hematopoietic Stem Cell Transplant (HSCT) are immunocompromised. Infectious complications from bacterial, viral, and fungal sources constitute a major cause of morbidity and mortality in HSCT patients. Prophylactic use of antifungal agents is used to decrease the incidence of invasive fungal infections in HSCT patients. The most common fungal pathogens in HSCT patients are candida and aspergillus.1,2 Fluconazole (Diflucan, Pfizer) is one of the standard agents used for fungal prophylaxis, however, with emergence of non-albicans candida species, voriconazole (Vfend, Pfizer) is also a viable choice for antifungal prophylaxis in HSCT patients. 3
There is documentation that administration of voriconazole suspension with a high fat meal results in a significant decrease in the maximum concentration and the Area under the Concentration Curve. 4 Enteral feeding supplements have an average fat content in the range of 29–38%. This is a case report of a pediatric patient with impaired absorption of voriconazole suspension due to concurrent administration of an enteral feeding supplement.
There are not case reports either in primary literature or proprietary information from the drug manufacturer (Pfizer) that report the effect of enteral feeding supplements on voriconazole absorption or serum levels. There are medications that are noted to induce the metabolism of the CYP2C19 enzyme; however this patient was not prescribed any of these agents.
Mucositis or uncontrolled nausea and vomiting may lead to poor oral intake and lead to enteral supplementation with tube feeds for HSCT patients. Voriconazole is an agent used for fungal prophylaxis in HSCT patients. Because of this potential interaction, it is very important for HSCT patients to have therapeutic levels in order to avoid the morbidity and mortality associated with fungal infections.
Patient case presentation
This is the case of a 13-year-old Hispanic boy (34.2 kg, 1.14 m2) who had achieved stable therapeutic levels on voriconazole who later experienced levels reported as ‘none detected’ after the initiation of tube feeds. The patient had a diagnosis of myelodysplastic syndrome and Blooms syndrome. The patient received a 5/6 matched cord blood transplant. His stem cell transplant (SCT) preparative regimen was alemtuzumab, fludarabine, and melphalan. The patient also received Bactrim for pneumocystis prophylaxis and valacyclovir for viral infection prophylaxis. For graft versus host disease prophylaxis, he was prescribed mycophenolate mofetil and cyclosporine. With the initiation of vomiting and gastrointestinal bleeding, the patient was prescribed intravenous Pantoprazole and Granisetron therapy.
The patient began his HSCT preparative regimen with an infusion of alemtuzumab on transplant day −22, with one test dose followed by infusion for 3 days. Oral voriconazole was initiated on SCT day −13. The dose for the voriconazole was 5.8 mg/kg/dose given twice daily as an oral tablet. The serum voriconazole level from a sample on day −8 was reported as 1.07 mcg/mL.
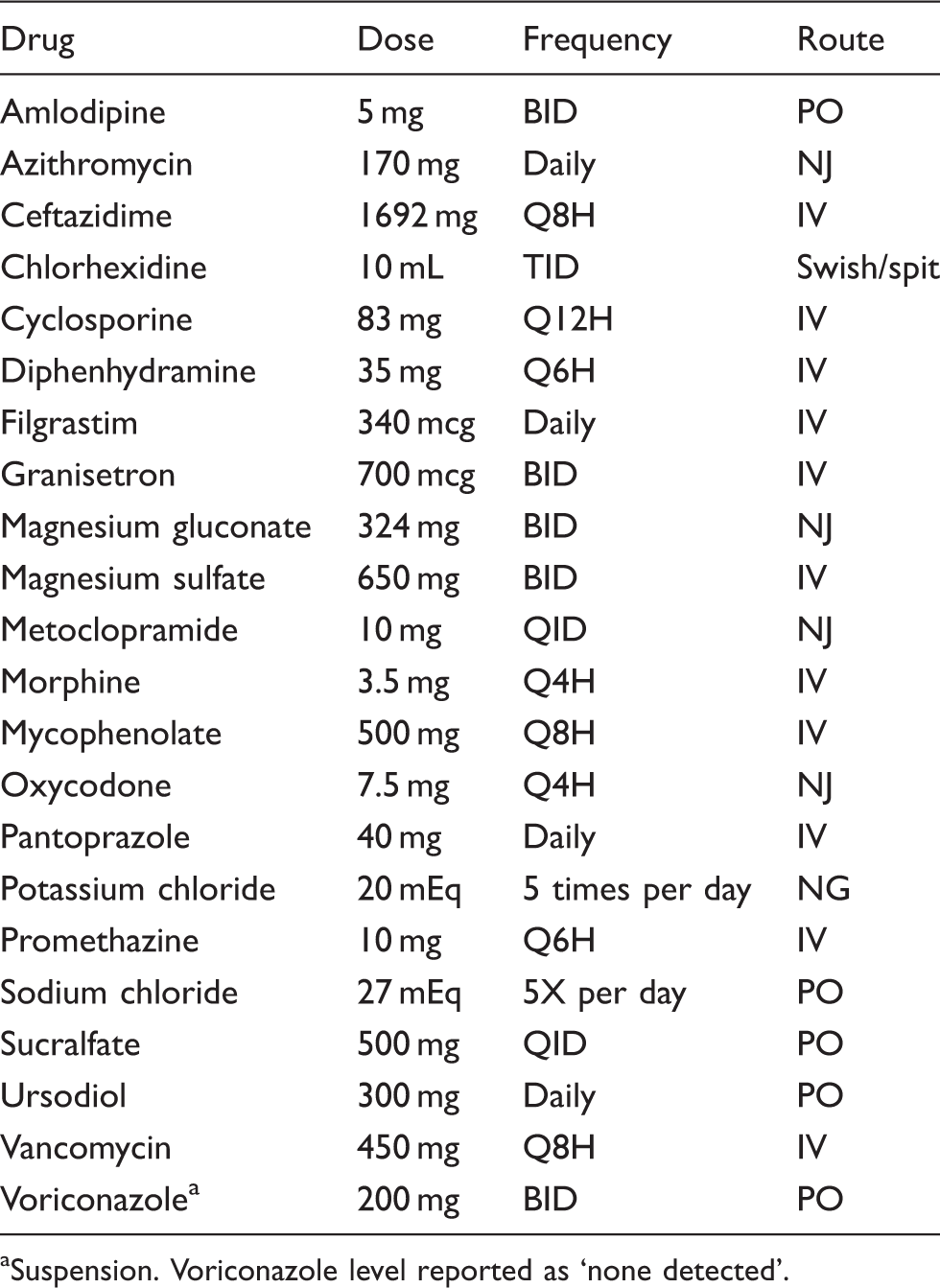
Over the course of SCT, day −2 to SCT day +8, the patient experienced nausea, vomiting, and evidence of gastrointestinal bleeding. The assessment of gastric bleed was made after one episode of blood-tinged mucous emesis on day −3. In response to the blood-tinged emesis, the patient was started on intravenous Pantoprazole at a dose of 1.1 mg/kg per day on day −2. Blood-tinged emesis was not reported again after this single episode. His last episode of emesis was reported on SCT day +4. On SCT day +8, the decision was made to start naso-jejeunem feeds in this patient. On SCT day +5, the voriconazole was changed from tablet to suspension. A serum voriconazole result from SCT day +13 was reported as ‘none detected’. This level was obtained 5 days after the start of tube feeds. A serum voriconazole level was repeated and the laboratory result form SCT day +20 was also reported as ‘none detected’. No drug–drug interactions were discovered to explain the change in serum levels.
The SCT pharmacist performed a careful review of the patient medication profile to ascertain potential drug–drug interactions that may explain the sudden decrease in therapeutic serum voricoazole levels. No drug–drug interactions were discovered to explain the change in serum levels.
Upon further review of the patient profile, the SCT pharmacist noted that the patient had been started on supplemental enteral nutrition with Isosource HN. The enteral nutrition was stared on day +8 at a rate of 15 mL/h for a 24 h continuous infusion. Isosource HN has a caloric content that is composed of 29% fat. There is a documented decrease in voriconazole maximum concentration and area under the concentration curve when voriconazole is administered with a high fat meal. 4 The maximum concentration is decreased by 58% and the area under the concentration curve is decreased by 37% when the suspension is given with a high-fat meal. Considering the fat content of Isosource HN, it is reasonable to conclude that the co-administration of the voriconazole suspension with the Isosource HN led to decreased drug absorption.
Medications on SCT day −8
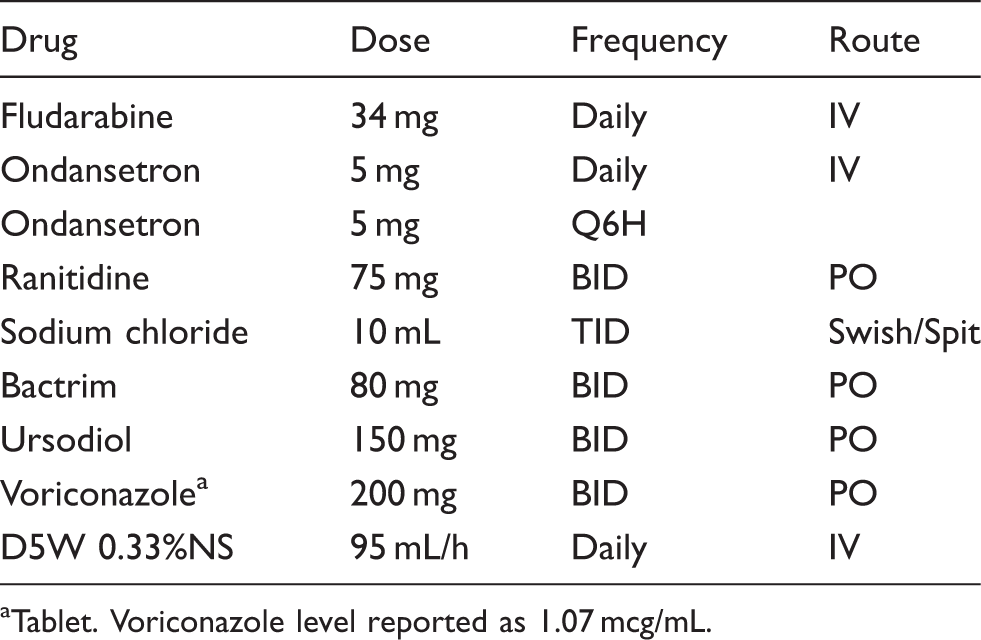
Tablet. Voriconazole level reported as 1.07 mcg/mL.
Discussion
Routine antifungal prophylaxis for HSCT patients is a necessary practice to decrease the morbidity and mortality associated with invasive fungal infections. The azole antifungals, including voriconazole, are very important agents to be used for this purpose. The pharmacokinetics of voriconazole are saturable and variable. Because of interindividual variability and interpatient variability, based on patient clinical condition, therapeutic drug monitoring of serum voricoazole levels has become a more common practice.10,11
Medications on SCT day +13

Suspension. Voriconazole level reported as ‘none detected’.
Medications on SCT day +20
Suspension. Voriconazole level reported as ‘none detected’.
Medications on SCT day +34
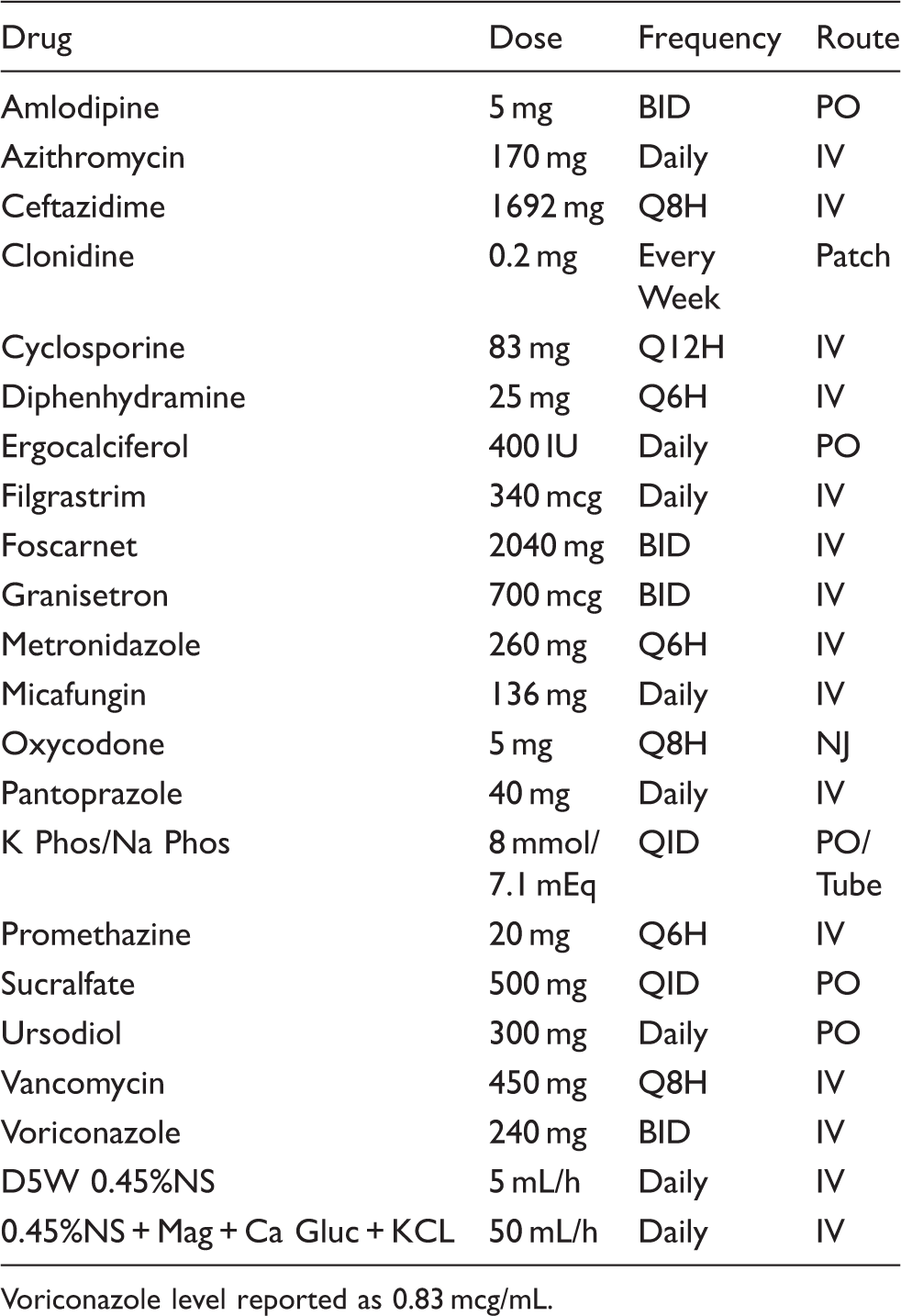
Voriconazole level reported as 0.83 mcg/mL.
Voriconazole levels during stem cell transplant course
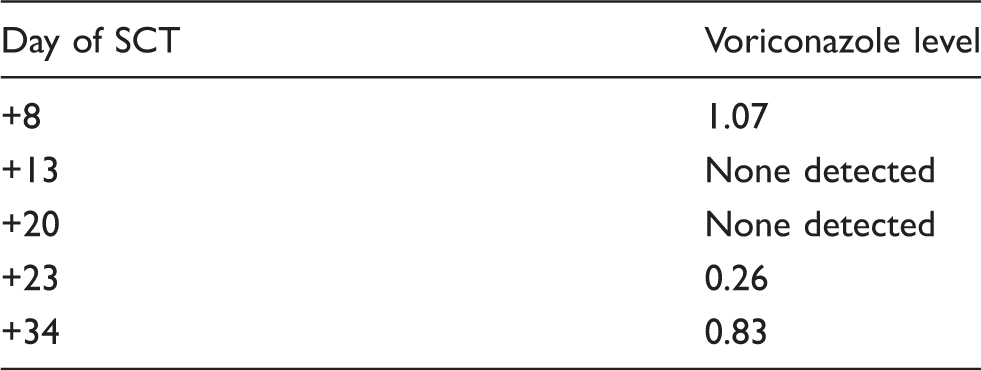
The oral bioavailability of voriconazole tablets and suspension is 96%. It is, however, important to understand that the maximum concentration and the area under the concentration time curve are decreased in the presence of a high-fat meal. 4 This case presents the fact that in addition to food, enteral nutrition supplements also affect the absorption of the oral dosage forms of voriconazole. During the course of treatment at our institution, no existing primary literature or proprietary information was discovered to explain this effect on voriconazole absorption.
The temporal relationship to changes in serum levels is within 5 days of initiating tube feeds, the voriconazole level decreased from therapeutic levels to ‘none detected’.
Based on the pharmacokinetic profile of voriconazole, it should take approximately 5 days to reach steady-state levels. When voriconazole was switched from oral to IV formulation and the serum level was rechecked 3 days later, a low level of drug was detected in the serum.
Based on the temporal relationship of serum drug levels in this patient and other observations of subtherapeutic levels of other patients prescribed tube feeds and enteral voriconazole, our SCT service physicians and licensed independent practictioners have been educated to separate dosing of this combination, or not to prescribe if the patient is receiving continuous enteral feeds. Because of this awareness and change in practice, we feel that we have decreased instances of invasive fungal infection in our HSCT patients.
Conclusion
This case outlines the temporal relationship of the effect of tube feeds on voriconazole serum levels. Based on this information, voriconazole suspension should not be prescribed to patients also receiving supplemental enteral nutrition. The HSCT service at Children's National Medical Center in Washington, DC, has made changes to the standard operating procedures for the SCT service for administration of voriconazole suspension and supplemental enteral nutrition.
The manufacturer of voriconazole, Pfizer, was contacted for solicitation of formal animal and human pharmacokinetic studies to evaluate this drugnutrient interaction; however, the lab that was used for the original pharmacokinetic studies is located outside of the United States. This situation makes it unlikely that formal evaluation of this interaction will be conducted in the near future. In the interim, it is the recommendation of the author to separate dosing of this combination, to avoid prescribing voriconazole suspension in patients receiving continuous enteral feeds, and to be very vigilant about checking serum voriconazole levels in patients on voriconazole suspension and enteral nutrition supplements.