
Abstract
Leucovorin is a reduced form of folic acid, which has multiple uses.1 In this case report, it is used in combination with fluorouracil in the treatment of colon cancer. We describe a 53-year-old male, who was started on FOLFOX 6 + bevacizumab who experienced a hypersensitivity reaction to leucovorin. There have been very few cases of leucovorin hypersensitivity reactions reported in the literature. In this case, symptoms include flushing, hives, body pain, headaches, elevated blood pressures, and general discomfort. Although leucovorin reactions are considered rare, one should be aware of the types of reactions that can occur with leucovorin.
Introduction
Leucovorin is a reduced form of folic acid, supplying the necessary cofactor blocked by methotrexate that enters the cells via the same active transport system as methotrexate. It stabilizes the binding of 5-dUMP and thymidylate synthetase, enhancing the activity of fluorouracil. Leucovorin has multiple uses – as an antidote for folic acid antagonists (methotrexate) and rescue therapy following high-dose methotrexate; in combination with fluorouracil in the treatment of colon cancer; in the treatment of megaloblastic anemia when folate is deficient as in infancy; sprue; pregnancy; and nutritional deficiency when oral folate therapy is not possible. 1
Leucovorin is included in the FOLFOX regimen for the treatment of colon cancer. 1 FOLFOX 6 consists of folinic acid (leucovorin), fluorouracil (5-FU), and oxaliplatin. FOLFOX and FOLFIRI regimens are used in the treatment of colorectal cancer. FOLFIRI consists of irinotecan instead of oxaliplatin along with leucovorin and fluorouracil.
FOLFOX 1 to 7 have all been used in the treatment of colon cancer. FOLFOX 4 is the most commonly used regimen. The use of FOLFOX 6 and 7 is increasing as it is more convenient for the patient and oxaliplatin intense. 2 The FOLFOX 6 regimen is given every two weeks with usual doses of oxaliplatin 100 mg/m2 and leucovorin 400 mg/m2 on day 1 followed by a 400 mg/m2 fluorouracil (5-FU) bolus and 46-h infusion dosed at 2400–3000 mg/m2. 3 Bevacizumab is dosed 5 mg/kg for colon cancer. 3 Bevacizumab, a monoclonal antibody has been shown to improve response rates in patients with stage IV colon cancer when used with 5-FU and oxaliplatin.
While there have been frequent incidences of allergic reactions to oxaliplatin, there have been few reported cases of leucovorin hypersensitivity. There are several adverse reactions reported with oxaliplatin use, the most common being sensory neuropathy associated with paresthesia of the hands and feet.
Our patient experienced elevated blood pressures, diaphoresis, extreme headaches, and severe generalized body pains lasting hours but resolving within 24 h. Our literature search using PubMed found descriptions of hypotension, urticaria, rash, and breathing difficulty in reported cases of leucovorin hypersensitivity. Search terms used included: leucovorin hypersensitivity, folinic acid hypersensitivity, and leucovorin allergy. The reaction we describe in this report is unlike the other reactions reported.
Case report
A 53-year-old Caucasian male diagnosed with Stage IV Colon Cancer was initiated on FOLFOX 6 + bevacizumab in May 2008. The patient’s medical history was significant for benign prostatic hyperplasia and a prior event of deep vein thrombosis. Prescribed medications included tamsulosin 0.4 mg orally daily and lorazepam 1 mg orally every 4 h as needed for nausea. Over the counter medications included acetaminophen and ibuprofen on an as-needed basis. The patient had no known drug allergies. All medications listed in the case were given intravenously unless otherwise noted. He completed all twelve cycles of treatment by October 2008. After several months in remission, the patient relapsed and was initiated on FOLFIRI + bevacizumab in July 2009. He completed all 12 cycles of FOLFIRI by December 2009. Prior to each FOLFOX and FOLFIRI treatments, the patient was premedicated with dexamethasone and palonosetron.
Unfortunately, new lesions were found on his PET scan shortly after completion of FOLFIRI + bevacizumab. Because the patient was positive for KRAS mutation, he was not a candidate for cetuximab or panitumumab. 4 Patients with tumors having KRAS mutations have a poor outcome when treated with cetuximab or panitumumab. 4 There were no open clinical trials at that time and it was decided that since the patient did not show clear evidence that he was resistant to chemotherapy, specifically oxaliplatin, he would be re-initiated on FOLFOX 6 + bevacizumab.
Summary of reactions at each cycle of treatment
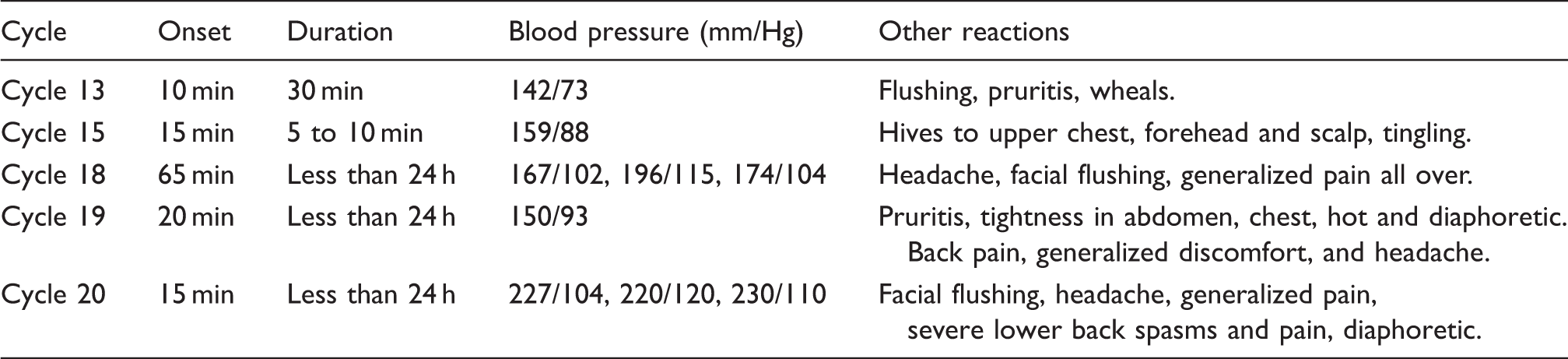
For subsequent cycles, diphenhydramine and ranitidine were given as premedications in addition to dexamethasone and palonosetron. When the patient returned for his 15th cycle, it was noted that he developed hives to the upper chest, forehead, and scalp (Table 1). Patient stated that he also experienced a couple of minutes of itching and tingling but that it had passed. He was able to complete the remaining infusion that day without complication.
The dose of leucovorin was reduced to 500 mg for the 18th cycle for undocumented reasons. At the 18th cycle of FOLFOX 6 + bevacizumab, 5 min into the infusion of oxaliplatin and leucovorin, the patient began to experience redness, pain, headache, and slight facial flushing, which subsided in 15 min. Similar reactions had been reported during cycles 13 and 15 (Table 1). Acetaminophen was given by mouth for his headache, and the infusion was continued. However 50 minutes later, the patient complained of an extreme headache, sensation of swelling of his entire body, and severe pain. The infusion was stopped. Meperidine and promethazine were given. His blood pressure remained elevated (Table 1). 5-FU was held for the 18th cycle due to this reaction. He was still experiencing a severe headache and was transferred to a neighboring ER where he was monitored overnight and discharged the next day.
Since reactions to oxaliplatin are frequently reported, it was suspected that the patient was still experiencing a hypersensitivity reaction to oxaliplatin. Therefore, the plan was to admit the patient for cycle 19 for oxaliplatin desensitization.
Instead of oxaliplatin desensitization, the patient was given a reduced dose of oxaliplatin. Oxaliplatin 180 mg and leucovorin 500 mg were scheduled to be given. Bevacizumab was not given during this treatment. Premedications given included ondansetron, dexamethasone, famotidine, and diphenhydramine.
Within 7 min of initiating the infusion of leucovorin and oxaliplatin, the patient began to experience pruritis, followed by a headache and elevated blood pressure (Table 1), and then tightness in the abdomen and chest, hotness, and extreme diaphoresis. Supportive medications given included subcutaneous epinephrine, hydrocortisone, diphenhydramine, lorazepam, meperidine, and ketorolac. Eight hours after the initial start of infusion, the patient was restless and reported back pain, generalized discomfort and headache. 5-FU was not administered in this cycle. Hydromorphone was administered for pain control. By the next morning, he was ready to be discharged.
It was assumed that the patient was experiencing hypersensitivity to oxaliplatin. Therefore when the patient returned to the clinic for his 20th cycle of therapy, oxaliplatin was discontinued and the plan was to administer bevacizumab 550 mg, leucovorin 500 mg, and 5-FU 900 mg bolus followed by a 46-h infusion of 4500 mg. Premedications given were dexamethasone, palonosetron, ranitidine, and diphenhydramine. Bevacizumab was administered with no complications. Fifteen minutes after the start of leucovorin infusion, the patient became very flushed in the face and neck and stated that he felt fuzzy headed and felt an onset of a throbbing headache. The leucovorin infusion was stopped. Ten minutes after stopping the infusion, the patient stated that he had a severe headache, severe back spasms, and general pain all over (Table 1). His blood pressure was elevated (Table 1), and he became very pale and sweated profusely. Supportive medications given included methylprednisolone, lorazepam, and hydromorphone. Due to the severity of symptoms, the patient was taken to the neighboring ER via ambulance. At the emergency room, the patient was given hydralazine, diazepam, and oral potassium bicarbonate. After overnight observation, he was discharged the next morning.
Based on the suspicion that the patient in fact had a leucovorin allergy, he was admitted to the hospital at a later date to be re-challenged on oxaliplatin monotherapy. Oxaliplatin 230 mg was given. Premedications included ondansetron, dexamethasone, diphenhydramine, and famotidine. Within a few minutes of the oxaliplatin infusion, he experienced the same erythematous spots on his face and chest with slight pruritis on his scalp as he had during his previous oxaliplatin treatments. Approximately 20 min later, the rash and itching had subsided. However, unlike the previous treatments that had been given with leucovorin, the patient was able to complete the oxaliplatin infusion without any complications. No severe headaches, body aches, or elevated blood pressures occurred with oxaliplatin monotherapy. To date, the patient has had four cycles of bevacizumab and oxaliplatin without any complications.
Discussion
In each cycle, generic leucovorin was dispensed. Additionally, it was thought that the patient developed a sensitization reaction to leucovorin since he did not react to the first round of FOLFOX & FOLFIRI. Based on the adverse events that the patient experienced from the last five cycles of therapy which included leucovorin, and on the minimal complications when oxaliplatin was administered as monotherapy, it can be deduced that the patient had developed a sensitization to leucovorin.
Case reports of Leucovorin reactions

A second case reported by Vermeulen and colleagues 5 involved a 57-year-old patient who was treated for metastatic rectal cancer with palliative treatment of 5-FU and leucovorin. The patient developed diffuse urticaria and difficulty in breathing during the initial treatment with a positive skin test with leucovorin performed three months after the reaction (Table 2). 5 A second case presented on the same report involved a 59-year-old man who was initiated on leucovorin, 5-FU, and oxaliplatin, for metastatic colon cancer following a colectomy. 5 The patient developed diffuse urticaria during the first and second infusions and reacted positively to a leucovorin skin test 3 weeks after the reaction (Table 2). However, oral desensitization was successful for this patient and they were able to complete treatment using leucovorin.
Although there have been cases of leucovorin hypersensitivity reported, the reaction in our patient is unlike the reactions seen in the other patients. Leucovorin hypersensitivity is a rare occurrence but it is imperative that practitioners and other healthcare professionals be aware of this possibility when prescribing and administering leucovorin. Based on the Naranjo’s Adverse Drug Reaction Probability Scale, 6 the score totaled 6 out of 10, categorizing this as a ‘probable’ adverse reaction. Oxaliplatin, bevacizumab and fluorouracil each scored less than one on the Naranjo scale. According to the Naranjo scale, these would be categorized as ‘doubtful’, thereby warranting a good reason for practitioners and other healthcare professionals to be aware of this possible hypersensitivity.
Conclusion
Patients should always be monitored closely when administered leucovorin, and it should not always be assumed that the patient is experiencing an allergic reaction to another likely medication such as oxaliplatin. Although reactions to leucovorin are rare, the possibility is there and health care providers should be aware of this possibility.