
Abstract
Background
Chemotherapy-induced nausea and vomiting are the most dreaded and distressing side effects for cancer patients undergoing chemotherapy treatment. These side effects have a significant impact on the patients’ quality of life and can interfere with their ability to receive intensive chemotherapy regimens. With the recent advances in antiemetic pharmacotherapy and supportive care, the current treatments for chemotherapy-induced nausea and vomiting, when used appropriately, have become highly effective in mitigating these adverse effects.
Objective
The aim of this study was to evaluate the current practice involving antiemetic treatment in newly diagnosed pediatric oncology patients at our center.
Methods
This was a retrospective cohort study of newly diagnosed pediatric oncology patients who were less than 14 years of age receiving their first cycle of inpatient chemotherapy. The data abstracted included the following: age, gender, type of cancer, chemotherapy regimen, emetogenic risk and level, prescribed prophylactic antiemetic regimen, incidence of breakthrough emesis, and breakthrough antiemetic medications used. Emetogenic risk was classified based on published guidelines into low, moderate, or high emetogenic chemotherapy, and a scoring system to determine the emetogenic level of combined chemotherapy agents was followed to monitor the efficacy of the antiemetic regimens. Clinical effectiveness was assessed based on breakthrough emesis.
Results
A total of 49 patients were eligible for the study. High emetogenic chemotherapy was administered in 28/49 (57.1%) and moderate emetogenic chemotherapy was administered in 21/49 (42.9%) patients. Only 10/49 (20.4%) received appropriate antiemetic prophylaxis, whereas 39/49 (79.6%) received inadequate antiemetic prophylaxis; 14/49 (28.6%) patients experienced breakthrough emesis. Breakthrough emesis occurred in 11/28 (39.3%) patients receiving high emetogenic chemotherapy and 3/21 (14.3%) patients receiving moderate emetogenic chemotherapy. The use of an inadequate antiemetic regimen was found in 14/14 (100%) patients with breakthrough emesis. Thus, inadequate prophylaxis resulted in a 35.9% (14/39) risk of breakthrough emesis. This risk was higher in patients receiving high emetogenic chemotherapy versus those receiving moderate emetogenic chemotherapy (39.3% versus 14.3%).
Conclusion
Inadequate antiemetic prophylaxis is associated with a high risk of breakthrough emesis particularly with high emetogenic chemotherapy regimens. Standardizing antiemetic prophylaxis based on emetogenic level could reduce breakthrough emesis and improve the quality of life in pediatric oncology patients.
Introduction
The clinical outcome of children diagnosed with cancer has improved significantly over the past several decades due to the ability to effectively and safely deliver more intense courses of chemotherapy.1–3 Monitoring and controlling the toxicities and side effects of chemotherapy agents remains a challenge. Chemotherapy-induced nausea and vomiting (CINV) is one of the most distressing side effects of chemotherapy in cancer patients.2,4 Inadequate control of CINV can lead to undesirable clinical complications, such as dehydration, electrolyte imbalance, and physical complications.4–6 These complications may prolong hospitalization, with the associated burdens on nursing time, pharmacy resources, and the overall cost implications. 7 The consequences of CINV may become more profound and may impact the patients’ quality of life, leading to lack of patient compliance and interfering with the ability to deliver more intensive chemotherapy regimens.6,8,9 It is therefore imperative to optimize the antiemetic prophylaxis regimen for each chemotherapy cycle according to the emetogenicity level of each chemotherapy regimen to minimize the probability of CINV.5,6
The established international clinical practice guidelines published by the National Comprehensive Cancer Network (NCCN), the American Society of Clinical Oncology (ASCO), and the Multinational Association of Supportive Care in Cancer (MASCC) provide healthcare providers with valuable evidence-based recommendations for the management of CINV, and the application of these guidelines must be accompanied by an accurate assessment of the risk of nausea and vomiting.10–13 The appropriate antiemetic treatment should be chosen by evaluating the emetogenic risk of chemotherapy as a single agent and as a combination therapy.14,15
For most children receiving any chemotherapy with emetogenic potential (except those with low risk), a 5-hydroxytryptamine-3 (5-HT3) receptor antagonist should form the backbone of antiemetic therapy. Children who are receiving highly emetogenic chemotherapy will certainly benefit from the addition of dexamethasone, particularly with platinum- or anthracycline-containing regimens.10,14,16,17 Most of the clinical studies and guidelines for CINV are focused on adult populations, and their findings are extrapolated for pediatric applications. This study aims to evaluate the current practice of antiemetic medication use in pediatric oncology patients using standard antiemetic interventions based on international practice guidelines.
Methods
Study site
This study was conducted at an oncology center within a 440-bed tertiary care hospital. The center was operated in 2001 with five main units: adult oncology, adult hematology/BMT, pediatric oncology, radiation oncology, and palliative care. The pediatric oncology unit currently accepts approximately 150 new oncology cases every year and is currently treating more than 1000 patients
Study design and subjects
Emetogenic risk of some of the chemotherapy agents
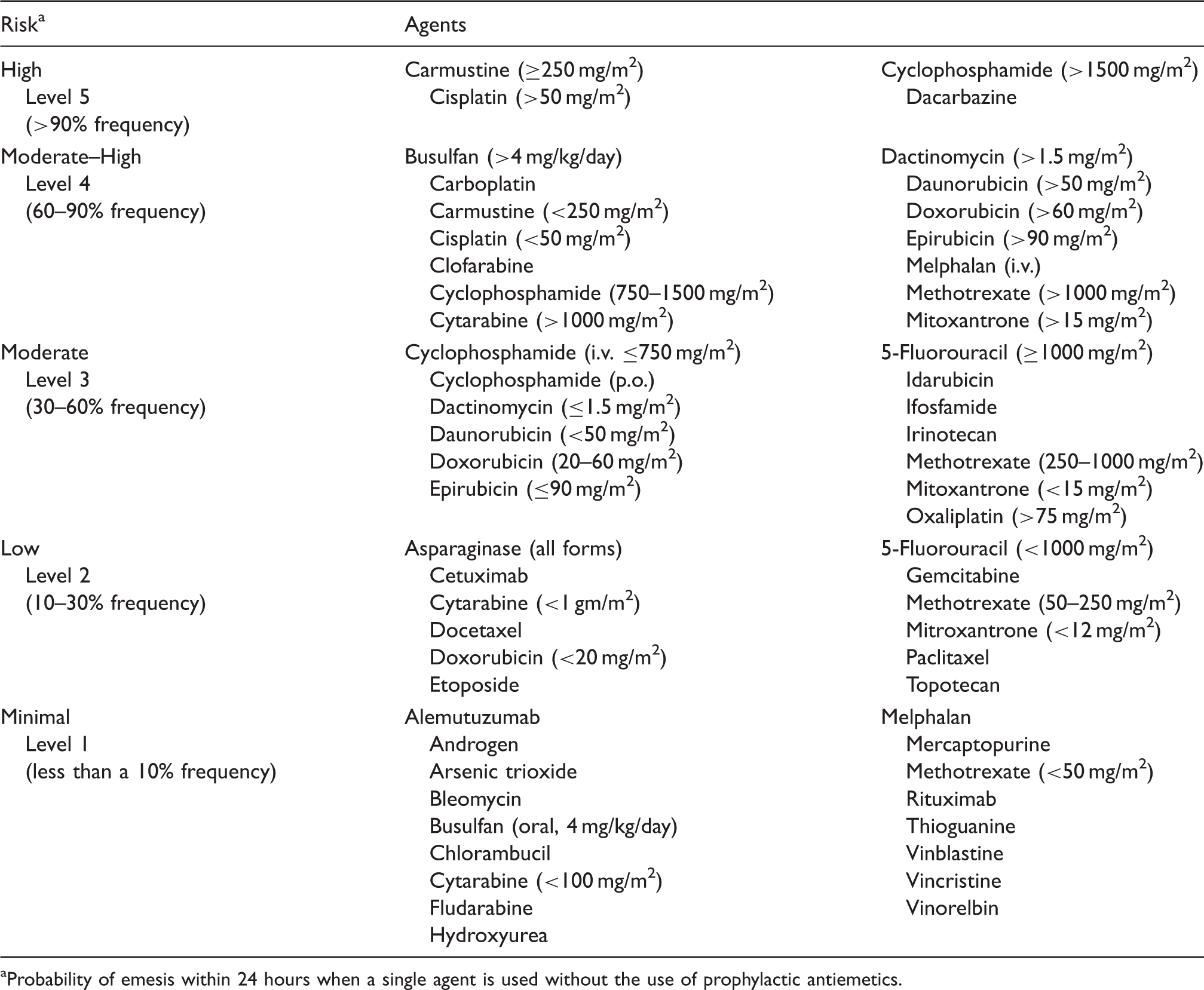
Probability of emesis within 24 hours when a single agent is used without the use of prophylactic antiemetics.
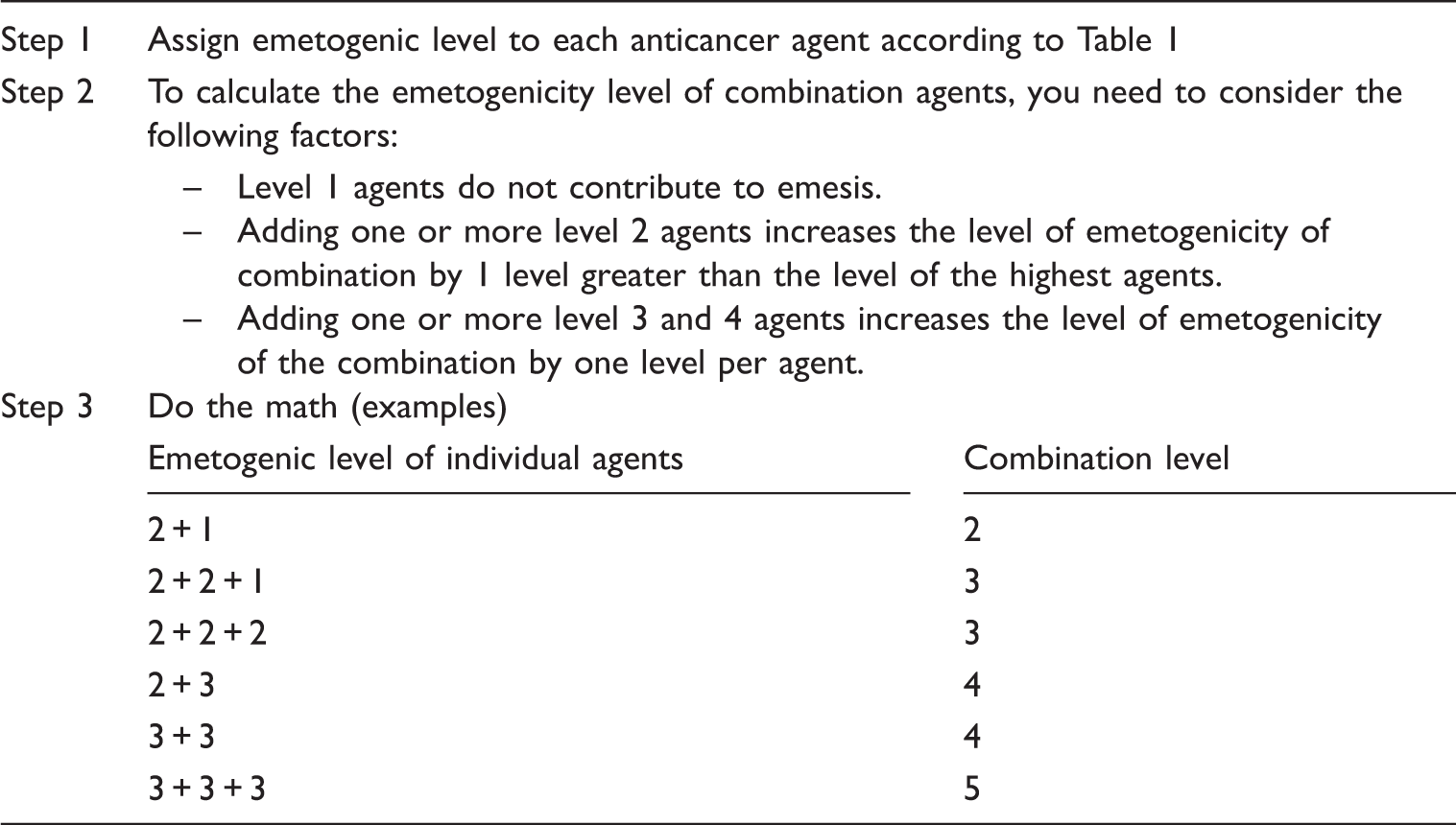
Steps to determine the emetogenicity level of combination chemotherapy
The clinical effectiveness of the antiemetic prophylactic regimen used for each patient was determined based on the incidence of breakthrough emesis or the need for additional antiemetic medications because of uncontrolled nausea. We considered those patients who had additional antiemetic treatments after they received the antiemetic prophylactic therapy as breakthrough emesis. The following data were obtained from the medical records: age, gender, diagnosis, chemotherapy protocol, prophylactic antiemetic regimen prescribed, frequency of breakthrough emesis, and the need for additional antiemetic medications.
Results
A total of 49 consecutive patients were eligible for the study. The patients’ ages ranged from 6 months to 13.8 years with a mean age of 6.5 years (SD 3.7); 21 (46.9%) were less than 6 years, 28 (57.1%) were 6 years and older, and there were 23 (46.9%) boys and 26 (53.1%) girls.
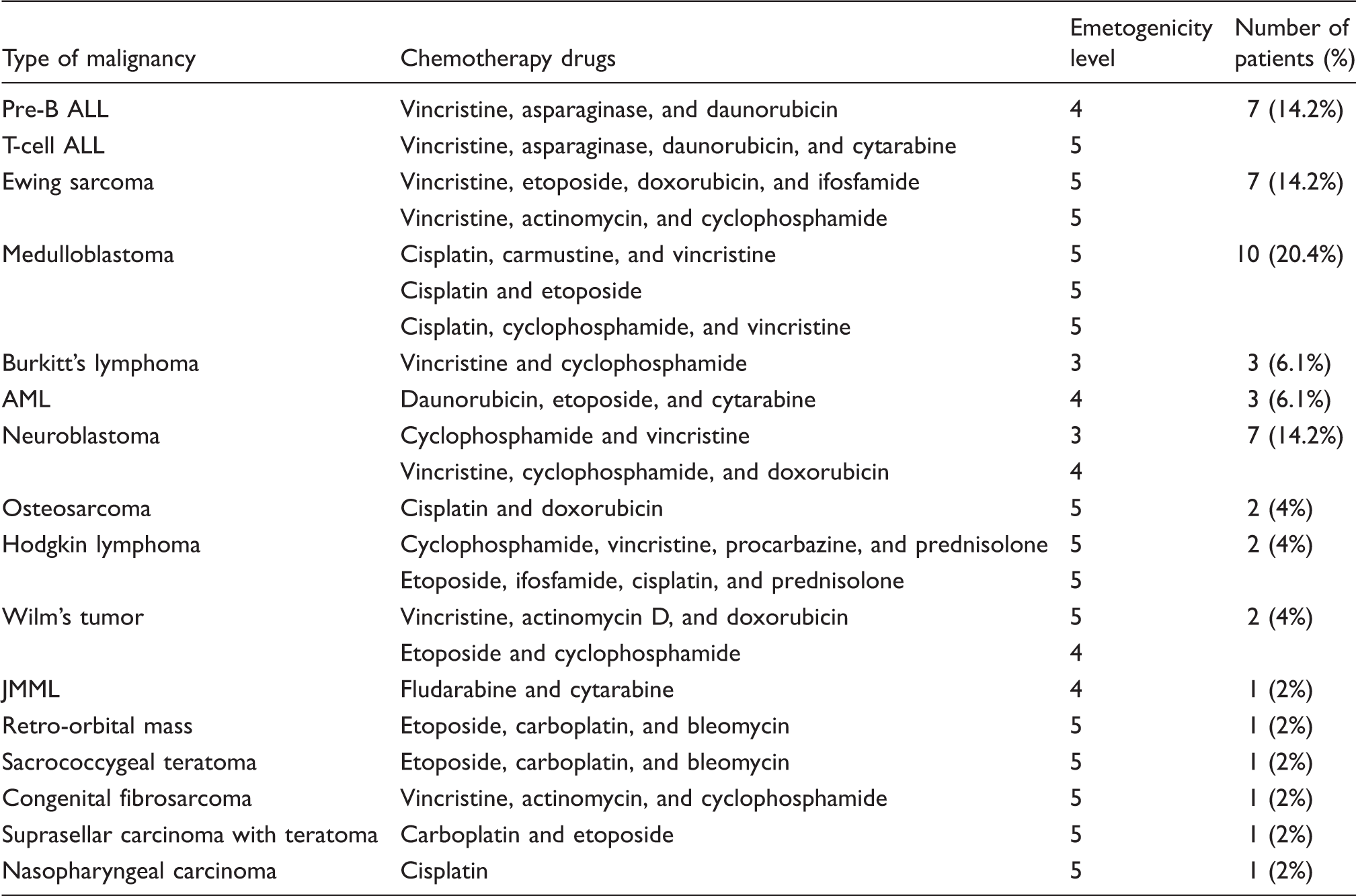
Chemotherapy agents and emetogenicity level (n = 49)
Emetogenicity level of chemotherapy and the appropriateness of the antiemetic regimen received (n = 49 patients)

HEC: high emetogenic chemotherapy; MEC: moderate emetogenic chemotherapy; LEC: low emetogenic chemotherapy.
Breakthrough emesis was absent in patients who received appropriate antiemetic prophylaxis, while 14 out of 39 (35.9%) patients who received inadequate antiemetic prophylaxis had breakthrough emesis. The difference in the number of breakthrough emesis between patients treated with appropriate and inappropriate antiemetic regimen was statistically significant (p = 0.044). Among patients who had breakthrough emesis, no differences were found based on gender (p = 1) and age (p = 0.542). However, breakthrough emesis was more frequent in patients receiving HEC regimens. Eleven out of 28 (39.3%) patients receiving HEC and 3 out of 21 (14.3%) patients receiving MEC suffered from breakthrough emesis. However, there was no statistically significant difference in incidence of breakthrough emesis between HEC and MEC risk patients (p = 0.066).
Discussion
The use of optimal antiemetic prophylaxis is important to ensure optimal treatment and reduce the complications of CINV. The current study provides retrospective evaluation of the use of antiemetic treatments across common chemotherapy regimens used in pediatric oncology patients at our center. Overall, we found that prophylactic antiemetics were underutilized in more than two-thirds of our patients. Inadequate antiemetic prophylaxis was documented in several chemotherapy regimens included in this study, particularly with HEC regimens. This study showed that inadequate antiemetic prophylaxis was responsible for all of the breakthrough emesis. The rate of breakthrough emesis showed no difference based on gender or age group but was more frequent in patients receiving inadequate antiemetic prophylaxis and HEC regimens. On the contrary, the study results have shown that appropriate antiemetic prophylaxis was effective at preventing CINV in children recruited in this study.
Several barriers to optimizing CINV control have been identified in the literature, including the underestimation of CINV prevalence by clinicians, lack of routine assessment, and poor knowledge and lack of adherence to published CINV guidelines.5,18 Grunberg and colleagues found that more than 75% of physicians and nurses underestimate the incidence of CINV following HEC and MEC. 19 Additional barriers to optimizing antiemetic prophylaxis include underutilization of and non-compliance with international practice guidelines, which were developed to help healthcare practitioners caring for cancer patients deliver high-quality care; however, this goal will be only achieved through adherence to the recommendations and their integration into everyday clinical practice. 18
The findings of this study revealed an important fact: standardizing and unifying the use of antiemetic prophylaxis is an important part of successful chemotherapy management in pediatric oncology patients. Most clinicians rely on 5-HT3 antagonists as antiemetic prophylaxis and do not consider the emetogenicity level of the combined chemotherapy agents. The consequences of CINV are unpleasant and are often devastating for children and their families, and the cost implications on hospital resources cannot be ignored. Thus, there is a need for quality improvement projects that mandate the use of pre-printed order sets for chemotherapy regimens including appropriate supportive care prior to and after chemotherapy treatment. The order set should address the appropriate timing and choice of prophylactic antiemetic treatment to provide the maximum protection and to prevent CINV-related complications. This practice will insure that patients receiving chemotherapy will receive appropriate management of antiemetic prophylaxis according to the emetogenicity level and will prevent inconsistencies in prescribing practice. We believe that the modified method used in Table 2 in our study may help better guide the standardization of antiemetic prescribing practice.
Over the last 3 years at our center, we were successful in implementing preprinted chemotherapy order sets that standardize the chemotherapy regimens, doses, and administration times. Our future project can focus on including standard prophylactic antiemetic regimens that will be based on the emetogenicity level of the chemotherapy regimen; the use of these regimens by physicians and nurses prior to chemotherapy will then be mandated. Once this practice is developed, another similar study will be conducted to test the impact of antiemetic standardization practice on the rate of CINV at our center.
To the best of our knowledge, there have been few studies that evaluate the use of standard antiemetic prophylaxis in pediatric oncology patients receiving chemotherapy regimens. Our study has a few limitations. First, it is retrospective in nature and has all of the limitations of retrospective studies. Due to the retrospective nature of this study, we were not able to look at the outcome or the severity of CINV due to inappropriate antiemetic prophylaxis therapy using standard classification method such as Common Terminology Criteria for Adverse Events (CTCAE) that was developed by the National Cancer Institute. In addition, Patients’ communication of the need for antiemetics and/or the nurses’ documentation of the patients’ episodes of emesis may have been inconsistent. Second, the variable treatment protocols used in this study resulted in small numbers of patients receiving certain protocols. Third, the study included a small number of patients. Despite this, our results indicate that breakthrough emesis was absent in all patients receiving appropriate antiemetic prophylaxis compared to 35.9% breakthrough emesis in those receiving inappropriate antiemetic prophylaxis. Fourth, this is a single center study and results may be difficult to reproduce. Nevertheless, single center studies have the advantage of ethnic homogeneity compared to heterogeneous ethnic groups in multicenter studies. We believe that this may be applicable when generalizing to ethnically matched groups particularly when drug sensitivity/toxicity is being addressed. Lastly, the study did not evaluate the possibility of nausea and vomiting after hospital discharge, but most patients stayed in the hospital 48–72 h after their chemotherapy regimen. Despite this limitation, our results indicate that inadequate antiemetic prophylaxis is common and is associated with a high incidence of breakthrough emesis in pediatric oncology patients at our hospital. This result underscores the need for standardized antiemetic prophylaxis based on emetogenicity level of different protocols.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.