
Abstract
Purpose
The primary purpose of this study was to determine the rate of infusion reactions to cetuximab in oncology patients treated at the University of North Carolina Cancer Hospital. Secondarily, we sought to evaluate predictors of grade 3–4 hypersensitivity, including geography.
Methods
Data were collected by retrospective chart review for patients treated with cetuximab at the University of North Carolina Cancer Hospital between 15 November 2006 and 31 December 2010. Data were analyzed for occurrence of hypersensitivity reaction in 125 patients with various cancer types.
Results
Of the 125 subjects, 31 (24.8%) experienced an infusion reaction of any grade. Of 125, 18 (14.4%) experienced a grade 3 or 4 reaction. The odds ratio for patients with an allergy history having a grade 3 or 4 reaction was 2.57 (95% CI 0.93 to 7.09, p = 0.07). Pretreatment with steroids was associated with absence of grade 3 or 4 reaction with an odds ratio of 0.21 (95% CI 0.05 to 0.83, p = 0.04). Mapping of reaction rates by county revealed higher rates in some of the more rural counties of North Carolina, however, statistical power was lacking.
Conclusions
Rates of hypersensitivity reaction at UNC are similar to rates seen in other areas of the southeastern United States and higher than in other regions of the United States and Europe. Rates of both hypersensitivity reactions and grade 3 to 4 hypersensitivity reactions have not substantially changed over time. Geography, allergy history, and perhaps smoking or cancer type may help predict who will react to cetuximab. Steroids should be strongly considered as premedication in addition to diphenhydramine.
Introduction
Cetuximab is a chimeric human/murine IgG1 monoclonal antibody that binds to the EGFR receptor to inhibit MAP-Kinase signaling and induce antibody-dependent cellular cytotoxicity. 1 Cetuximab is FDA-approved to treat metastatic colorectal cancer (CRC) and squamous cell carcinoma of the head and neck (SCCHN). 2 In the BOND trial, 3 patients with CRC who had progressed after irinotecan-based therapy responded to cetuximab monotherapy and to cetuximab plus irinotecan. Radiologic tumor response to therapy occurred in 22.9% of patients in the combination group and 10.8% of patients in the monotherapy group (p = 0.007). Bonner et al. 4 compared radiotherapy alone to radiotherapy plus weekly cetuximab in SCCHN and found the median duration of locoregional control was 24.4 months with combined therapy and 14.9 months with radiotherapy alone (p = 0.005). The median survival time was 49.0 months in patients who received combined therapy and 29.3 months in patients receiving radiotherapy alone (p = 0.03). Studies have also examined cetuximab treatment for non-small cell lung cancer (NSCLC), breast cancer, and hepatocellular carcinoma (HCC).5–7
Cetuximab is a relatively well-tolerated agent, compared to other antineoplastic drugs. Cutaneous adverse reactions including papulopustular rash, nail changes, and pruritis are the most common side effects, but fatigue, nausea, and other adverse reactions typically associated with cytotoxic antineoplastic agents are rare.1,2 However, infusion reactions are a known adverse effect associated with cetuximab. The reaction is a hypersensitivity (HSR) or anaphylactic reaction that most often occurs early during the first infusion of cetuximab. Pyrexia, dyspnea, chills, rigors, urticaria, bronchospasm, and hypotension may occur in an infusion reaction.
The cetuximab package insert notes mild infusion reactions occur in 15–21% of patients while severe reactions, grades 3 and 4, occur in 2–5% of patients. 2 Multiple sources of data from the United States and the world back up this assertion. Foley et al. 8 examined infusion reactions requiring medical intervention with data extracted from a nationwide United States claims database and found a rate of 8.4%. A post hoc analysis of the MABEL study conducted in Europe found that 2.4% of patients experienced grade 3 or 4 infusion-related reactions and 15.6% experienced any grade infusion-related reactions. 9 In another trial conducted in Europe, Cunningham et al. 3 found severe anaphylactic reactions occurred in 1.2% of patients. In the EPIC trial conducted at sites worldwide, 1.4% of patients had a grade 3 or 4 infusion reaction. 10
In contrast, higher rates of infusion reactions have been consistently found in the southeastern United States. O’Neil et al. 11 retrospectively reported on 90 patients treated at the University of North Carolina (UNC) and 53 patients treated at the Vanderbilt Ingram Cancer Center and the Sarah Cannon Cancer Research Institute, both in neighboring Tennessee. At UNC, 20% (95% CI, 12% to 43%) of patients had a hypersensitivity reaction (HSR) of any grade and 14% (95% CI, 8% to 23%) had a grade 3 or 4 HSR. Considering only patients on clinical trials at UNC and at the two sites in Tennessee, the rate of grade 3 to 4 HSR was 22% (95% CI, 13.5% to 32%). Subsequent reports of patients treated roughly contemporaneously confirm this reaction rate. For example, George et al. 12 found that 27% of patients experienced a grade 2 to 4 hypersensitivity infusion reaction at a Florida Veterans Affairs facility between 2004 and 2008. At Morris Oncology Treatment Center in North Carolina between 2005 and 2007 an HSR of any grade was experienced by 29% of patients. 13
Physicians and nurses at UNC have observed higher reaction rates in recent years than the 14% rate previously reported. 11 In addition to previously reported associations of allergy history, nurses have noted association with geography within North Carolina. The primary purpose of this study was to determine the rate of infusion reactions to cetuximab at UNC Hospitals between 15 November 2006 and 31 December 2010. Secondarily, we sought to evaluate predictors of grade 3–4 hypersensitivity, including geography.
Methods
Patients
Patients treated with cetuximab at the University of North Carolina Cancer Hospital between 15 November 2006 and 31 December 2010 were identified using pharmacy records. Data collected by retrospective chart review included presence of infusion reaction to cetuximab, symptoms of reaction, cycle number when reaction occurred, outcome of reaction, medications administered to treat a reaction, premedications administered, history of allergy to medications, food or environmental exposures or presence of a non-sedating antihistamine on the current medical record, as well as cancer type and demographic information. The grade of the infusion reaction was determined as noted in the medical record or by review of the symptoms associated with the reaction as noted in the medical record. National Cancer Institute Common Toxicity Criteria for Adverse Events version 3.0 was used to assess grades of hypersensitivity reactions; version 3.0 was chosen to allow comparison with the prior study conducted at UNC by O’Neil et al. 11 Subjects were included if they were over 18 years of age, cetuximab was ordered by the treating oncologist, and the infusion initiated. Subjects were excluded if they received their first dose of cetuximab before 15 November 2006. Cetuximab reactions were mapped based on county of patients’ residence for patients from North Carolina including the patients in our study and the patients in the previous study conducted by O’Neil et al. 11 from patients treated with cetuximab prior to 15 November 2006. Approval for the study was obtained from the Institutional Review Board at the University of North Carolina at Chapel Hill.
Statistical analysis
Descriptive statistics were conducted to determine the demographics of the study population. The primary endpoint was defined as the proportion of patients who experienced a grade 3 or 4 cetuximab reaction. Chi-square analysis was performed to determine what factors are associated with a severe (grade 3, 4 or 5) HSR. Adjusted odds ratios (ORs) were obtained using logistic regression. All statistical analyses were performed with SAS v. 9.3 and significance level at 0.5.
Geographic distributions were obtained for patients treated with Cetuximab and their respective county of residence. Maps were generated using ArcGIS 10.0 software.
Results
Demographics.
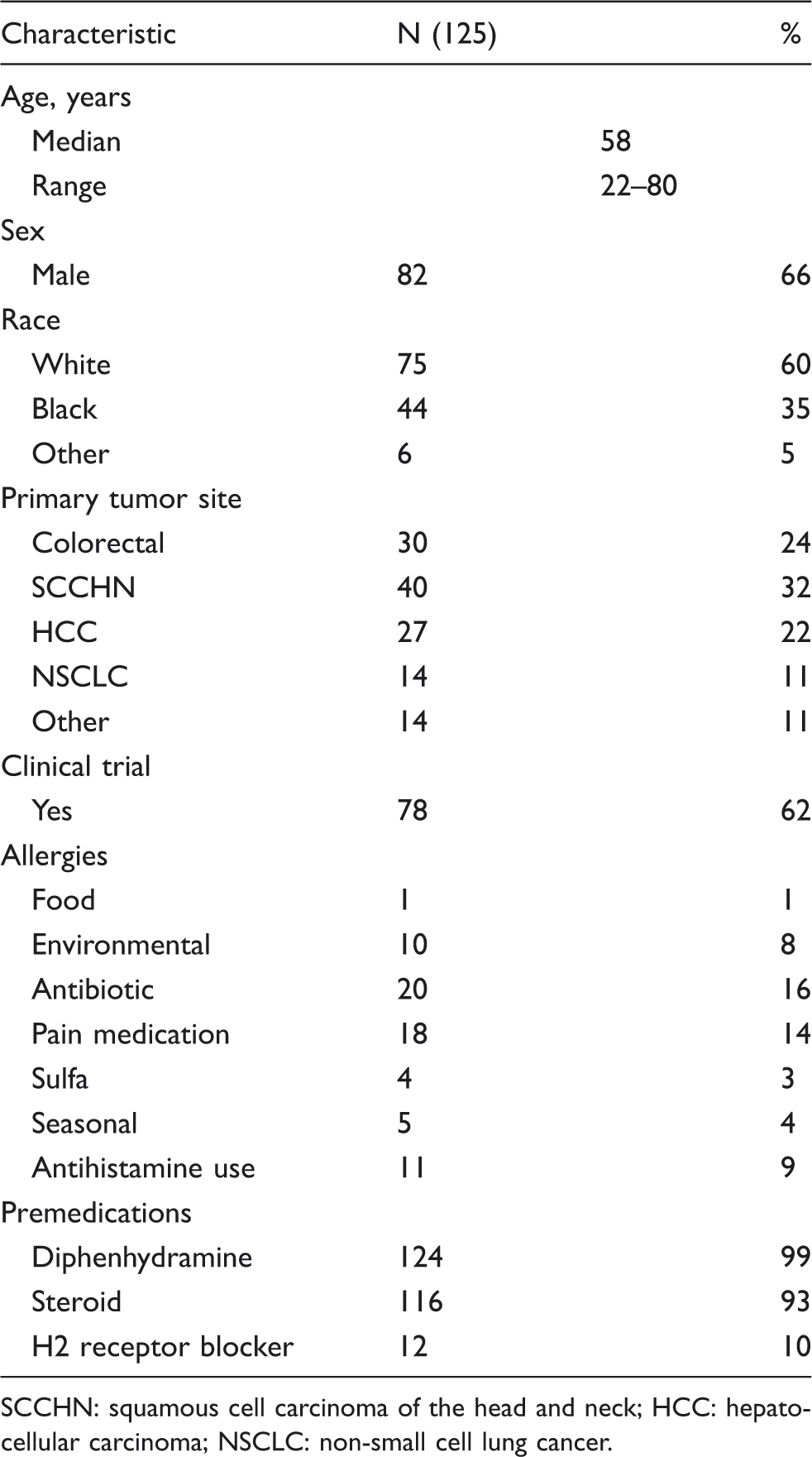
SCCHN: squamous cell carcinoma of the head and neck; HCC: hepatocellular carcinoma; NSCLC: non-small cell lung cancer.
Considering only the patients that had an infusion reaction; 2 of 31 (6.5%) experienced a grade 1 reaction, 11 of 31 (35.5%) grade 2 reaction, 15 of 31 (48.4%) grade 3 reaction, and 3 of 31 (9.7%) grade 4 reaction. Of the patients that had an infusion reaction 18 of 31 (58.1%) resolved after stopping the infusion either with or without additional treatment. Three of 31 (9.7%) resulted in emergency room (ER) admission and 4 of 31 (12.9%) resulted in hospitalization. Of the three patients sent to the ER, two patients had grade 3 reactions, and one patient had a grade 4 reaction. Of the four hospitalizations, one patient had a grade 2 reaction, one patient had a grade 3 reaction, and two patients had grade 4 reactions.
Six of 125 (4.8%) patients who had an infusion reaction to cetuximab were rechallenged and able to continue receiving cetuximab. Two of the rechallenged patients were desensitized then able to continue cetuximab. Three of the patients were treated with additional medications (diphenhydramine and/or steroid) to treat their symptoms; the infusion was restarted without another infusion reaction. One patient was restarted at half the infusion rate after treatment with diphenhydramine, prochlorperazine, and calcium carbonate and was able to receive the entire dose.
Correlation patients’ known allergies on having a grade 3 or 4 HSR.
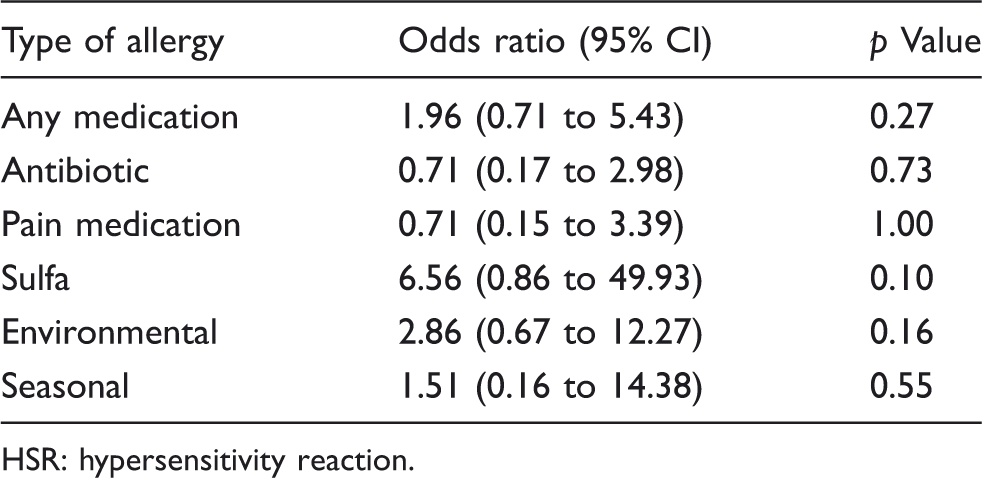
HSR: hypersensitivity reaction.
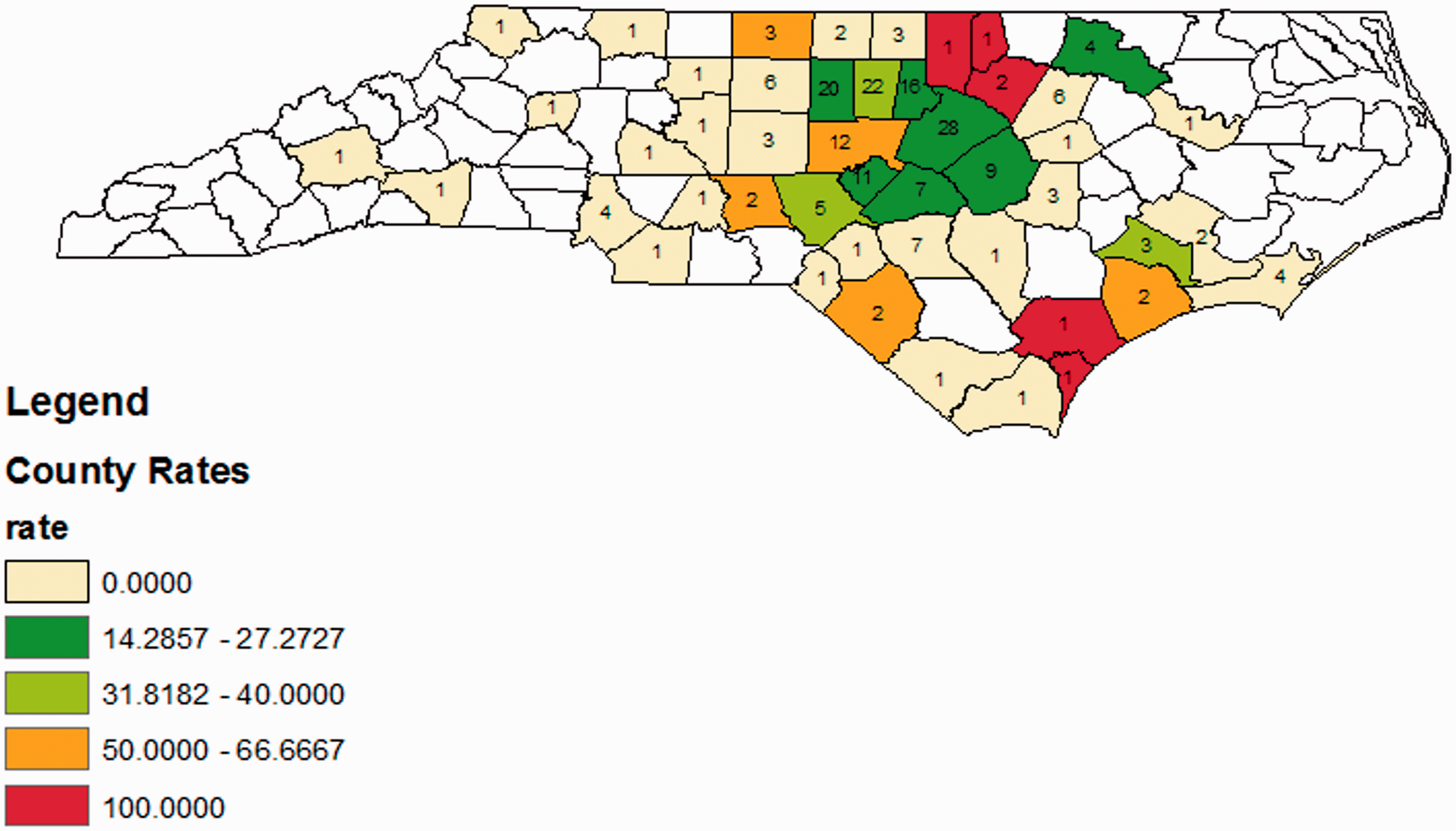
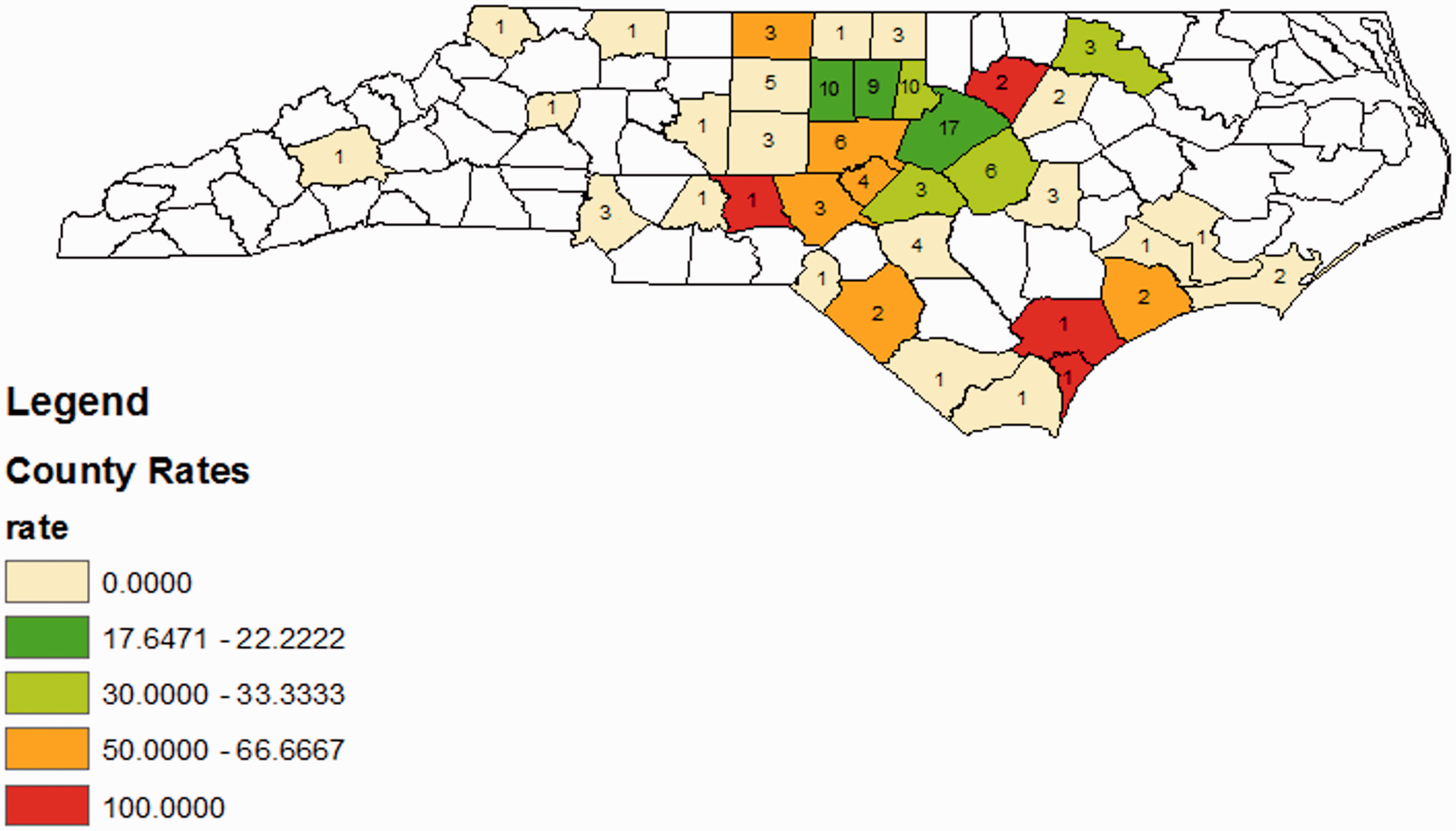
Mapping of patients’ county of residence was done to determine if higher rates of reaction could be linked to known geographic factors. For reference, population density is shown in Figure 1. While some clustering can be seen in Figures 2 and 3, statistical power was not adequate to prove any relationships. Geographic data were not available at the time of analysis from the O’Neil study and has not been previously published. We therefore were able to increase the power to evaluate the meaning of these clusters by incorporating patient data from that time period. Data were granular to the level of county. Anecdotally patients from rural areas appear to be more likely to have an infusion reaction. Some evidence of this is seen in the maps; the more rural counties of Chatham and Franklin have a higher rate of infusion reactions and a higher average grade of infusion reaction when compared with the more urban Wake County. Unfortunately, the statistical power for formal layered-map analysis remained too small. Further, we lack adequate data for much of North Carolina; patients treated at UNC were far more likely to live in counties close to Orange County where UNC is located.
Map of population density by county in North Carolina (2010). Map of HSR by county. Rate is the number of patients divided by the number of patients treated in each county then multiplied by 100. The numbers on the map are the number of patients treated in each county. Map includes data from this study and the study by O’Neil et al.
11
Map of HSR by county. Rate is the number of patients divided by the number of patients treated in each county then multiplied by 100. The numbers on the map are the number of patients treated in each county. Map includes data from this study only.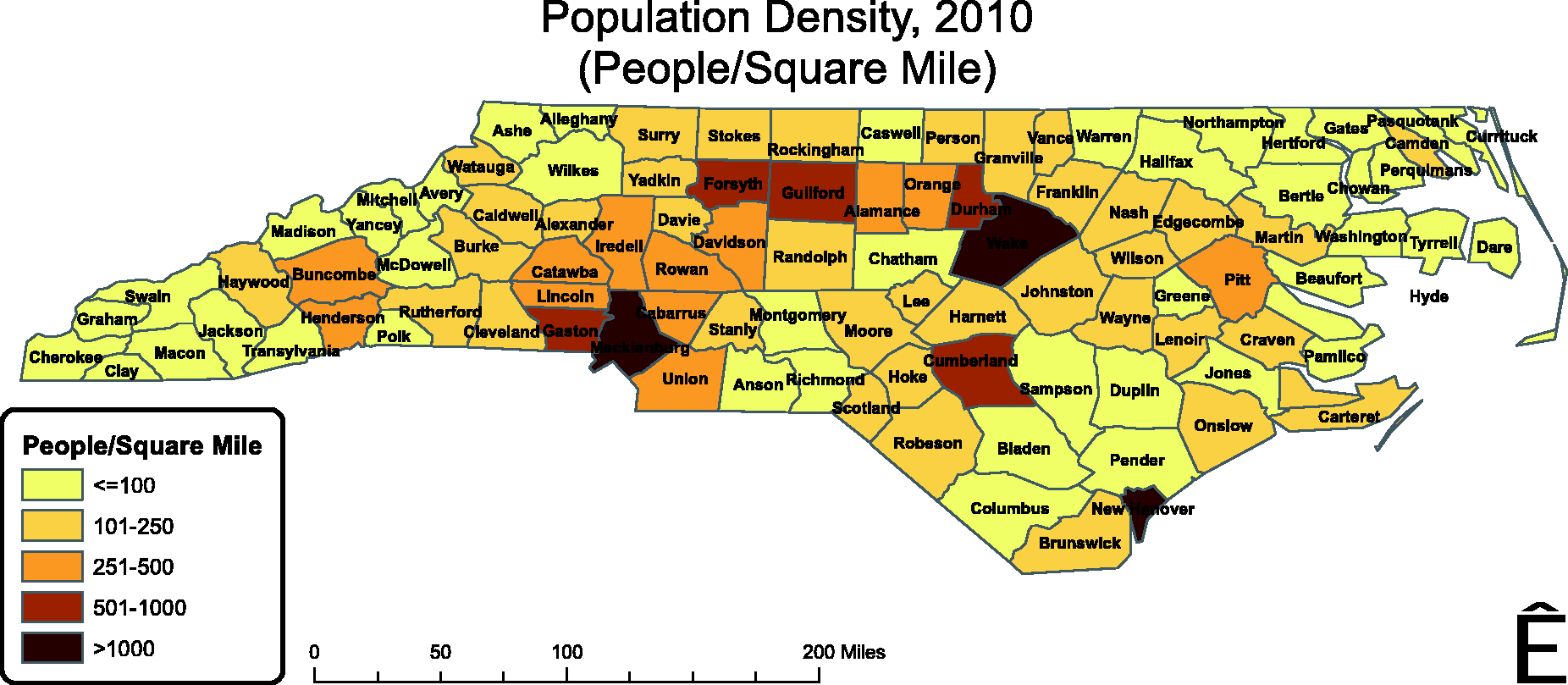
Discussion
Although cetuximab can add to treatment efficacy for colon cancer, head and neck cancer, and perhaps other malignancies, infusion reactions represent a significant problem. In the high-risk region of the United States, many patients who might otherwise benefit from cetuximab do not receive it due to fear of infusion reactions. When mild reactions occur, they can cause discomfort and anxiety to the patient and more severe reactions can be life threatening. Finally, infusion reactions are expensive—the analysis by Foley et al. 8 demonstrated a median additional cost of $2168 when only outpatient care was needed and $6670 when admission was required. Notably, these costs do not include the costs of non-productive cetuximab, which is over $3000.
The rates of reaction at UNC found in this study were similar to the rates found in the prior study by O’Neil et al. 11 In the current study, 14.4% of patients experienced a grade 3 or 4 reaction as compared to 14% in the prior study completed at UNC and two sites in Tennessee. Likewise, reactions of any grade were found in 24.8% in this current study as compared to 20%. Therefore, the hypothesis that infusion reaction rates have substantially increased over time is unfounded.
O’Neil et al. 11 found that patients with a significant allergy history were significantly more likely to experience an HSR; while some other studies have supported this trend, 13 others have not.8,12,14 In our study, patients with an allergy history trended to a higher likelihood of experiencing a grade 3 or 4 HSR, especially those patients with a sulfa allergy although this was not statistically significant, perhaps due to a small number of patients who had a sulfa allergy. Patients with an environmental allergy also trended toward increased infusion reactions. The current study was not able to differentiate true allergic reactions from adverse reactions labeled as allergy in the chart. In particular, adverse reactions to pain medicines are commonly listed as allergies; these reactions could have weakened the statistical power of the analysis.
Smoking has been previously hypothesized to influence cetuximab reaction rates. In a series from the Oklahoma University Health Sciences Center, the relative risk from ongoing smoking was 4.3. 14 Although smoking status was not assessed in the O’Neil study, patients with NSCLC had higher infusion reaction rates and a trend toward increased grade 3−4 reactions. In contrast, this link was not found in patients with SCCHN in the O’Neil study despite the strong link between smoking and SCCHN. Infusion reaction rates, severe infusion reaction rates, and location of recruitment in major head and neck cancer studies4,15–17 have been too variable to allow for firm conclusions regarding the link between smoking and infusion reaction or malignant disease process and smoking. In the current study, rates of any HSR were similar across cancer types, although there was a trend toward increased reaction rate with NSCLC. This study did not collect data on smoking history so no comparison could be made between smoking and reaction rates; in retrospect, these data should have been collected and its absence is a weakness of this work. Further, a major weakness of our geographic work is the clustering of patients near UNC; if resources had allowed, we would have preferred to conduct a multi-center study that would increase the statistical power of layered map analysis by both providing geographic diversity and a higher n.
The tick population data in Figure 4 are particularly significant because one dominant hypothesis to explain the clustering of cetuximab infusion reactions in the southeast of the United States is that it is caused by Amblyomma americanum (Lone Star Tick).
18
The geographic area of the United States where the tick is endemic extends westward to include Oklahoma and Missouri, where high rates of cetuximab anaphylaxis have also been reported.14,19 This region overlaps heavily with the geographic region where delayed anaphylaxis to beef is common. This latter fact is particularly significant as preformed IgE antibodies specific for the carbohydrate galactose-α-1,3-galactose, which is present on the cetuximab heavy chain, have been linked both to cetuximab hypersensitivity and to meat allergy.
20
Two case reports of patients with allergies to red meats found that intradermal skin testing with cetuximab resulted in wheal formation at the site of testing.
21
Tick distribution in North Carolina.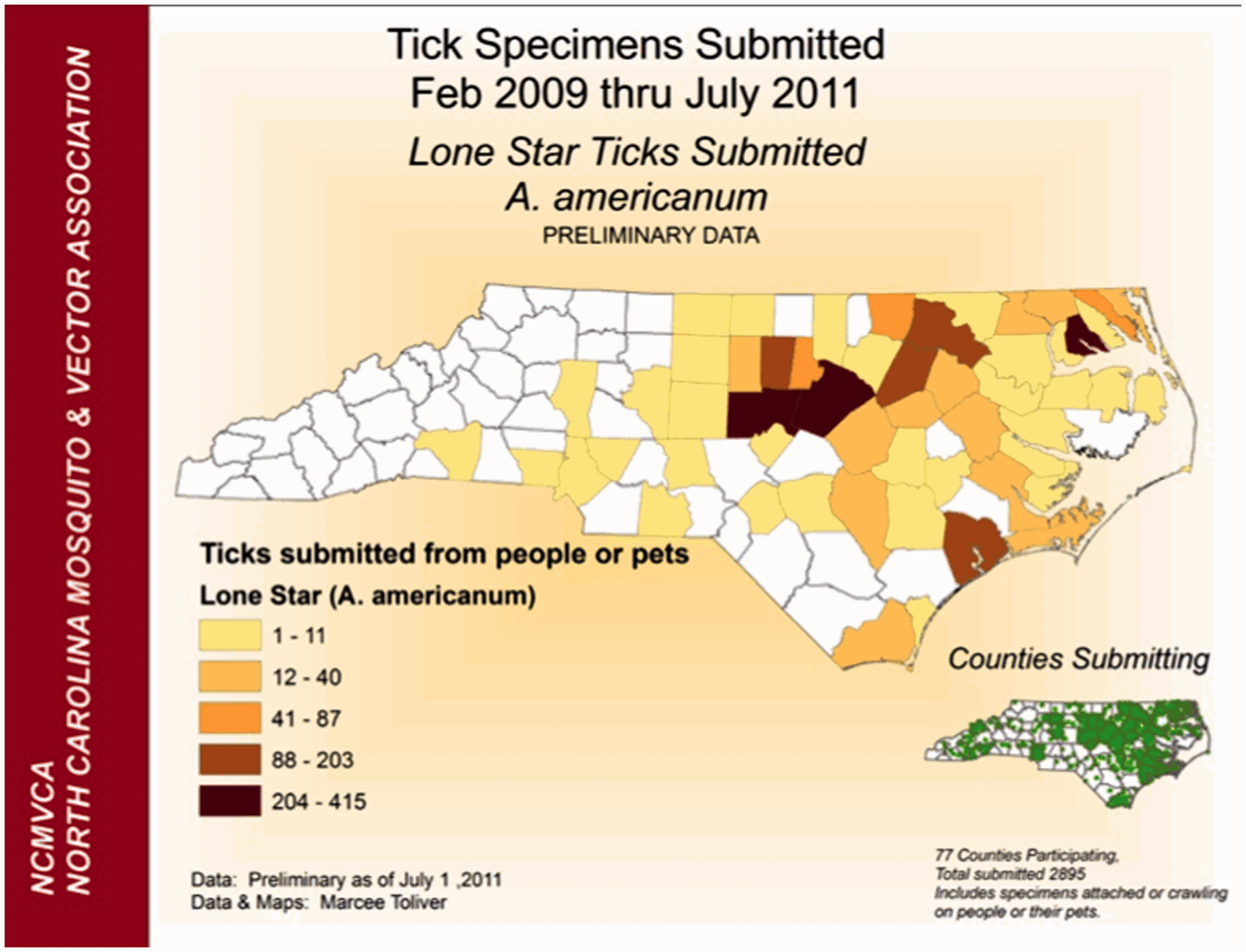
Chung et al. 22 examined serum samples from patients in different regions of the United States to look for IgE antibodies specific for galactose-α-1,3-galactose. A group of 76 patients that had received cetuximab, 25 of whom had a HSR, were screened for detectable levels of the IgE antibody using pretreatment serum samples. Of the 25 patients with HSRs, 17 had the antibody; in contrast 1 of 51 patients who did not react to cetuximab had the antibody. Control testing was done on patients from Tennessee, California, and Boston. In Tennessee, 15 of 72 (20.8%) had the IgE antibodies, in California 3 of 49 (6.1%) had the IgE antibodies, and in Boston 3 of 341 (0.6%) had the IgE antibodies. This data raises the hypothesis that the presence of antibodies for galactose-α-1,3-galactose might be used to predict cetuximab hypersensitivity reactions. Unfortunately, banked serum samples are not available on the patients described herein for analysis. However, we are currently evaluating this hypothesis as part of a prospective study of a cetuximab-containing regimen for induction chemotherapy for advanced SCCHN. 23
In addition to predicting cetuximab reactions, it would be clinically useful to prevent them. The UNC protocol for cetuximab infusions includes premedication with intravenous diphenhydramine, dexamethasone, and an H2 receptor blocker. Infusion time is 120 minutes for the first infusion and 60 minutes for subsequent infusions. For patients receiving their first infusion the treating physician is present for the first 15 minutes in case of a reaction. We found that most patients received diphenhydramine and a steroid; only 10% received an H2 receptor blocker. In the prior study by O’Neil et al., 11 91% of patients received diphenhydramine and a steroid, 23% of patients also received an H2 receptor blocker. This study found that pretreatment with steroids, in addition to diphenhydramine, resulted in a lower risk of experiencing a grade 3 or 4 HSR. These data are consistent with a post-hoc analysis of the MABEL trial. 9 In the MABEL study, 67 of 700 (9.6%) patients who were premedicated with an antihistamine and a steroid experienced infusion reactions while 108 of 422 (25.6%) patients treated with an antihistamine alone experienced an infusion reaction. Considering only grade 3 and 4 reactions, 7 of 700 (1.0%) treated with antihistamine and steroid and 20 of 422 (4.7%) treated with only an antihistamine experienced infusion reactions. The authors recommend routine premedication with steroids.
Desensitization was conducted for two patients in our study that had infusion reactions to cetuximab. Although the medical record did not record the specific protocol, both patients were admitted to the hospital for 24-hour observation. They were premedicated with steroids, diphenhydramine, and an H2 receptor blocker; in addition the cetuximab infusion time was extended.
In conclusion, the incidence of HSR with cetuximab reported here is about 24% with severe reactions occurring in about 14% of patients. The incidence of both HSRs and grade 3−4 HSRs have not substantially changed over time as compared to the incidence at UNC in prior years. 11 Geography, allergy history, and perhaps smoking or cancer type may help predict who will react to cetuximab. However, once validated, an ELISA assay for preformed IgE antibodies against galactose-α-1,3-galactose may ultimately have superior predictive capacity and may be more clinically useful. Steroids should be strongly considered as premedication to reduce incidence and severity of HSR. For patients with colon cancer who live in high-risk areas, the fully humanized EGFR antibody panitumumab may be considered in place of cetuximab 24 ; its role in the treatment of SCCHN is less promising.25,26 We and others are evaluating the role of other EGFR inhibitors in the treatment of SCCHN. Finally, as most reactions occur early in the first infusion, close supervision of the beginning of the first infusion is prudent.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declare that there is no conflict of interest.