
Abstract
Objectives
The main objective was to evaluate the impact of two methods aiming at reducing hazardous drug environmental contamination: the centralization of the priming of IV tubing in the pharmacy and the use of a closed-system transfer device. The secondary objective was to evaluate the satisfaction of pharmacy technicians using a survey.
Methods
Sites in the hematology-oncology satellite pharmacy and care unit were analyzed for the presence of cyclophosphamide, ifosfamide and methotrexate before and after the centralization of the priming of IV tubing in the pharmacy and before and after using a closed-system transfer device. The limits of detection for cyclophosphamide, ifosfamide and methotrexate were, respectively, of 0.0015 ng/cm2, 0.0012 ng/cm2 and 0.0060 ng/cm2. The pharmacy technician satisfaction was evaluated using a questionnaire.
Results
A total of 225 samples was quantified. After the centralization of priming in the pharmacy, no significant difference was found in the proportion of positive samples for cyclophosphamide, ifosfamide and methotrexate. Traces of cyclophosphamide found on the floor in patient care areas was significantly reduced (median[min-max] 0.08[0.06−0.09]ng/cm2 vs. 0.03[0.02−0.05], p < 0.0001). After using a closed-system transfer device, a significant difference was found for the proportion of cyclophosphamide positive samples (15/45(33%) vs. 0/45(0%), p < 0.0001), but no significant difference was found for ifosfamide (12/45(27%) vs. 5/45(11%), p = 0.059) and methotrexate (1/45(2%) vs. 2/45(4%), p = 0.557). Pharmacy technicians raised issues following the centralization of priming (e.g. workload) and the use of closed-system transfer devices (e.g. spills, particles, workload and handling difficulties).
Conclusion
The centralization of the priming of IV tubing in the pharmacy reduced floor contamination in patient care areas without increasing surface contamination in the pharmacy. Closed-system transfer devices reduced contamination in pharmacy, but handling issues were raised by pharmacy technicians.
Introduction
In 2004, the National Institute for Occupational Safety and Health (NIOSH) issued an alert for the prevention of occupational exposure to antineoplastics and other hazardous drugs in healthcare institutions. 1 This alert recommended preventive measures for handling hazardous drugs for workers in healthcare settings.
In Quebec, in response to this alert, the Association paritaire pour la santé et la sécurité du travail du secteur des affaires sociales (ASSTSAS) set up an expert committee to develop a prevention guide on the safe handling of hazardous drugs. A prevention guide was published in 2008. 2
Occupational exposure to hazardous drugs can occur at any point in the drug use process, especially during drug preparation and administration steps. Our research group focused on two key steps of the hazardous drug use process : (1) the priming of IV tubing and (2) the preparation.
The NIOSH alert recommended the hazardous drug tubing to be primed in the pharmacy in a biosafety cabinet (BSC) rather than in patient care zones. 1 The NIOSH alert also stated that a closed-system drug transfer device (CSTD) may be used when preparing and administering hazardous drugs. A CSTD is a medical device that minimizes the risks of leaks and spills that can happen when preparing and administering these drugs. 1
The ASSTSAS prevention guide also recommended the hazardous drugs tubing to be primed inside a BSC in the pharmacy and indicated that CSTDs can be used in certain situations. 2 For instance, the prevention guide stated that “while the use of closed-circuit systems has been shown to reduce contamination during preparation and administration, it does not entirely eliminate the risk of contamination, due to the limitations of this type of system and because other sources may be contributing to the contamination (vials whose exterior is contaminated, products which cannot be prepared using these systems, etc.). The primary obstacle to the use of these systems (CSTDs) is their high, recurring cost. Their cost-effectiveness ratio is not yet known, particularly in the context of care in Quebec. We are encouraging evaluative research to determine the role of this technology in Quebec practice. (…) Further investigation regarding the efficacy and ergonomics of these cabinets should be carried out before a general recommendation is made in this regard.” 2 Furthermore, “even if closed-circuit systems are used, the preparations should be compounded in [BSCs]”. 2 CSTDs may be useful in some situations, such as a major, documented environmental contamination problem despite compliance with the ASSTSAS guide and an inadequate infrastructure or lack of standard infrastructure for centers with very low preparation volume. 2
Numerous studies have shown the efficacy of CSTDs to reduce environmental contamination by hazardous drugs in pharmacy and patient care areas when compared to usual practice.3–15 However, few studies have looked at the impact of the priming of IV tubing in BSCs by pharmacy staff. 16
In this context, we studied the impact of the centralization of the priming of IV tubing in the pharmacy and of the use of a CSTD on reducing hazardous drug environmental contamination. We have also studied the satisfaction of pharmacy technicians in using these techniques
Methods
This is a prospective, experimental and comparative study.
Objectives
The primary objective of this study was to compare environmental contamination by cyclophosphamide (CP), ifosfamide (IF) and methotrexate (MTX) in the hematology-oncology satellite pharmacy and the hematology-oncology care unit after the centralization of the priming of the hazardous drug IV tubing compared with priming on care units. The second objective was to compare environmental contamination with CP, IF and MTX in the hematology-oncology satellite pharmacy after using a CSTD at the pharmacy for hazardous drugs preparation compared with preparation without CSTDs. The third objective was to evaluate the satisfaction of pharmacy technicians about the introduction of the centralized priming and the use of CSTDs.
Phases
The study was conducted between October 2009 and May 2010 in the hematology-oncology satellite pharmacy and the hematology-oncology care unit of a 500-bed pediatric hospital center. The study was divided into three phases.
In Phase I, the surface contamination with CP, IF and MTX was evaluated after using the center’s usual policy and procedures. Bags or syringes of hazardous drugs were prepared in the hematology-oncology satellite pharmacy and sent to the hematology-oncology care unit where the priming was done by nurses before patient administration. Nurses did the priming in a closed room dedicated to chemotherapy preparation. The priming was done by gravity with the hazardous drug contained in the bag or syringe.
In Phase II, the surface contamination with CP, IF and MTX was evaluated after the centralization of the priming of the hazardous drug IV tubing by gravity in the hematology-oncology satellite pharmacy. Bags and syringes of CP, IF and MTX were prepared in the satellite pharmacy. Priming was carried out with NaCl 0.9% in order to reduce the risk of contamination. Alaris infusion sets commercialized by Cardinal Health (Ontario, Canada) were used. Drugs were then administered to patients at the hematology-oncology care unit. This phase was preceded by a four-week training period for pharmacy technicians.
In Phase III, the surface contamination with CP, IF and MTX was evaluated only in the hematology-oncology satellite pharmacy after using a CSTD. CP, IF and MTX vials dilution and bags and syringes preparation took place in the satellite pharmacy using a CSTD. Phaseal® devices commercialized by Carmel Pharma (Ontario, Canada) were used for hazardous drugs preparation. Only MTX syringes for intrathecal injection and those administered outside the hospital were done without a CSTD and they were excluded from the study. This phase was also preceded by a four-week training period for the pharmacy staff. A three-day complementary training session was given by one employee from Carmel Pharma Inc to the pharmacy technicians. Aside the complementary training session, Carmel Pharma was not involved in the study.
Sampling sites
During Phases I and II, three sites were sampled in the satellite pharmacy: the BSC working surface, the drug delivery tray in the service hatch and the tray where the preparations were placed while waiting for the pharmacist’s validation. Two sites were sampled in the hematology-oncology unit: the floor in front of the hazardous waste container and the floor below the area where priming occurs. During Phase III, five sites were sampled in the satellite pharmacy: the BSC working surface, the drug delivery tray in the service hatch, the tray where the preparations were placed while waiting for the pharmacist’s validation, the pharmacist’s verification counter and the floor in front of the BSC. Sites were selected after being identified as those presenting the highest risk of environmental contamination based on a previous study. 17 Surface contamination was not evaluated in the hematology-oncology unit in Phase III considering the lack of time to implement and train appropriately the nursing staff with CSTDs in patient care areas.
Sites from the satellite pharmacy were sampled at the end of the pharmacy technician work day. Sites from the care unit were sampled at the beginning of the day before the cleaning staff’s shift. Sampling was performed by a different member of the research team in each phase. Each sampling site was sampled once a day for 15 days in each phase.
Thorough cleaning of work surfaces in the satellite pharmacy (counters, BSC, storage shelves and transfer, etc.) was performed before each of the three phases of the study. In addition, the hospital cleaning personnel cleaned the floors of the satellite pharmacy daily with quaternary ammonium and water. Surfaces were also cleaned daily on the care unit with quaternary ammonium and water.
Evaluation of the surface contamination
The analytic method used for the work surface sampling as well as the material required were described previously. 18 The sampling technique consisted of sampling a standard surface of about 600 cm2. Hazardous drug dosages were analyzed by high-performance liquid chromatography-tandem mass spectrometry. Each sample was analyzed for the presence of CP, IF and MTX. The limits of detection (LOD) for CP, IF and MTX were, respectively, of 0.0015 ng/cm2, 0.0012 ng/cm2 and 0.0060 ng/cm2. The limits of quantification for CP, IF and MTX were, respectively, of 0.005 ng/cm2, 0.004 ng/cm2 and 0.02 ng/cm2.
Appreciation of the new techniques
The pharmacy technician satisfaction was evaluated using a questionnaire after the introduction of the two new techniques, at the end of each phase. The questionnaire was made up of seven questions that covered the following subjects: the ease and speed of use, the clutter created by the material used, the technical problem encountered, the perceived risk of absorbing hazardous drugs through the skin or by inhalation as well as the perceived risks of injury, needle-stick incidents and spillage.
Statistical analysis
Results were entered into an Access database (Microsoft Office 2003, Seattle, WA). SPSS version 17.5 (IBM, Chicago, IL) was used for statistical analyses. A χ2 test was used to compare the proportion of the number of positive samples obtained between the phases. A value of p ≤ 0.05 was considered to be statistically significant.
Results
A total of 225 samples were obtained (75 samples in each of the three phases of the study). During Phase I, there were 129 preparations (i.e. 20 of CP, 6 of IF and 101 of MTX). During Phase II, there were 148 preparations (i.e. 26 of CP, 22 of IF and 100 of MTX). During Phase III, there were 109 preparations (i.e. 29 of CP, 27 of IF, 53 of MTX).
Centralization of the priming
Proportion of CP, IF and MTX positive samples before and after the centralization of the priming of IV tubing.
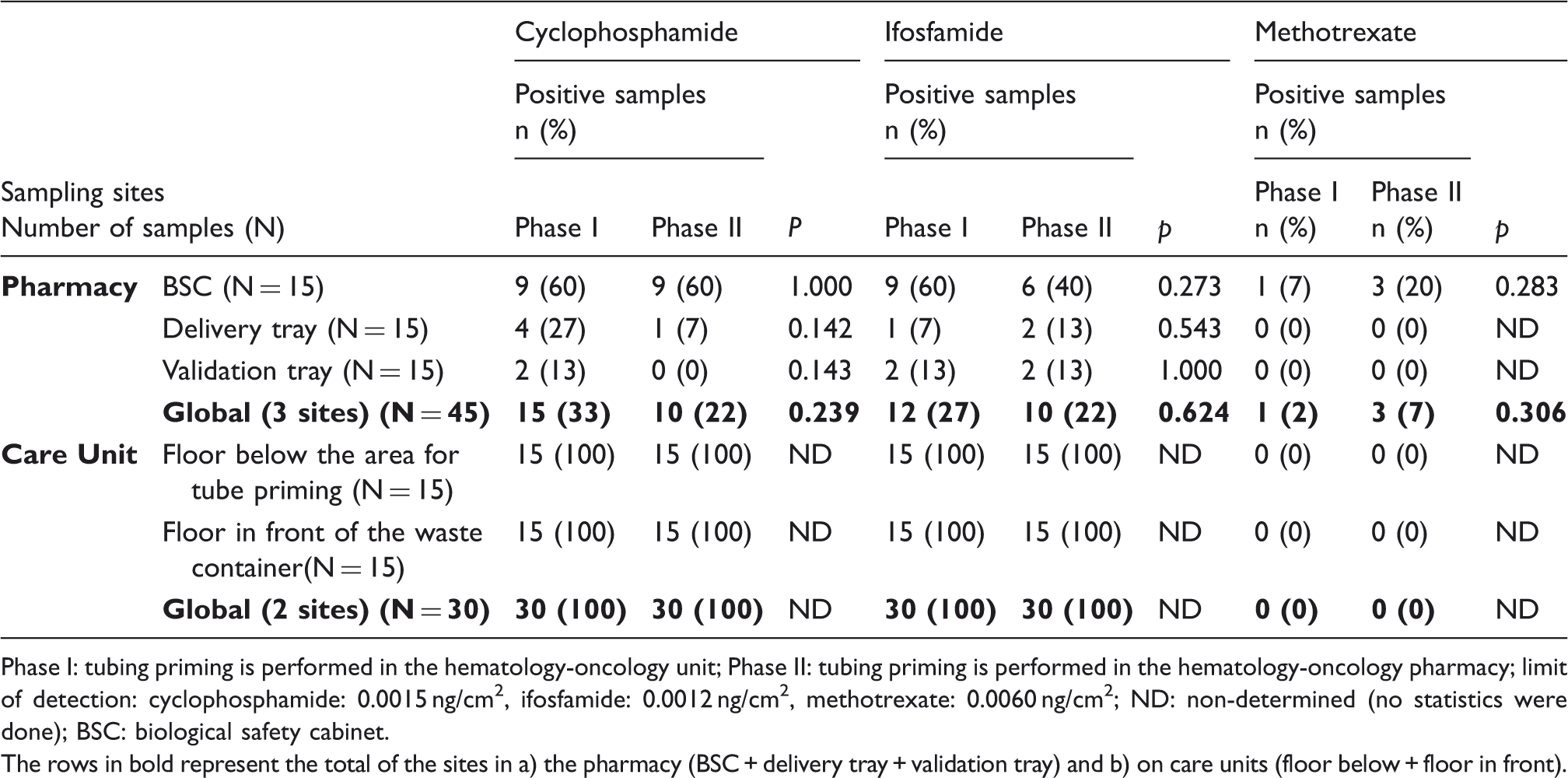
Phase I: tubing priming is performed in the hematology-oncology unit; Phase II: tubing priming is performed in the hematology-oncology pharmacy; limit of detection: cyclophosphamide: 0.0015 ng/cm2, ifosfamide: 0.0012 ng/cm2, methotrexate: 0.0060 ng/cm2; ND: non-determined (no statistics were done); BSC: biological safety cabinet. The rows in bold represent the total of the sites in a) the pharmacy (BSC + delivery tray + validation tray) and b) on care units (floor below + floor in front).
The surface concentrations measured for CP varied from <LOD to 8.80 ng/cm2 in Phase I and from <LOD to 28 ng/cm2 in Phase II at the pharmacy and varied from 0.06 ng/cm2 to 0.37 ng/cm2 in Phase I and from 0.02 ng/cm2 to 0.39 ng/cm2 in Phase II on the care unit.
The surface concentrations measured for IF varied from <LOD to 0.15 ng/cm2 in Phase I and from <LOD to 3.10 ng/cm2 in Phase II at the pharmacy and varied from 0.11 ng/cm2 to 1.20 ng/cm2 in Phase I and from 0.08 ng/cm2 to 0.94 ng/cm2 in Phase II on the care unit.
The surface concentrations measured for MTX varied from <LOD to 0.09 ng/cm2 in Phase I and from <LOD to 2.40 ng/cm2 in Phase II at the pharmacy and no MTX concentrations were detected during Phases I and II on the care unit.
In the pharmacy, there was no statistically significant difference between Phases I and II for the surface concentrations of three drugs evaluated irrespective of which site was sampled. In the care area, a statistically significant difference was observed between Phases I and II for CP and IF on the floor in front of the cytotoxic waste container (median CP: 0.08 vs. 0.03 ng/cm2, p < 0.001; median IF: 0.90 vs. 0.15 ng/cm2, p < 0.001).
Using a CSTD for hazardous drugs preparation
Proportion of CP-, IF- and MTX-positive samples before and after using a CSTD for hazardous drugs preparation.
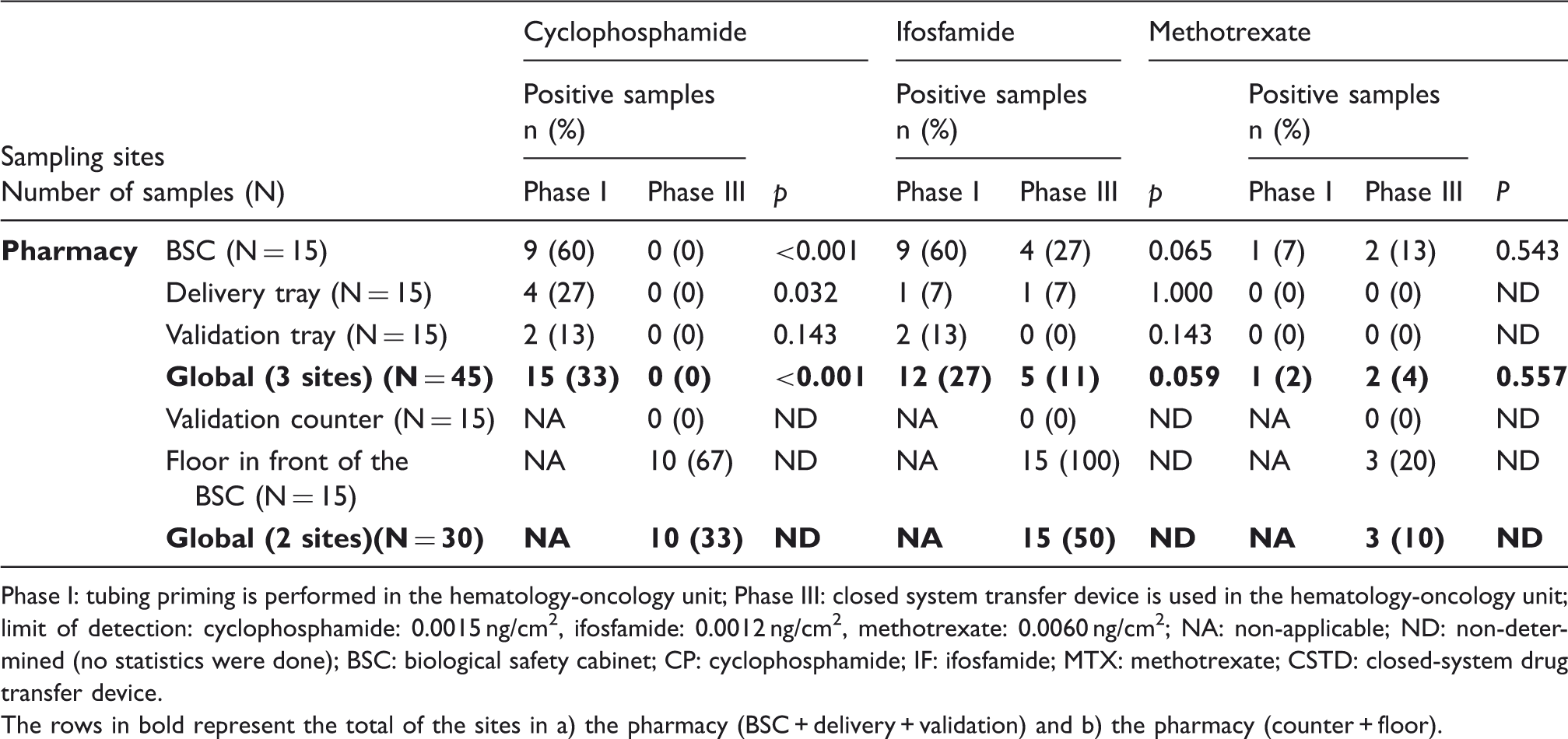
Phase I: tubing priming is performed in the hematology-oncology unit; Phase III: closed system transfer device is used in the hematology-oncology unit; limit of detection: cyclophosphamide: 0.0015 ng/cm2, ifosfamide: 0.0012 ng/cm2, methotrexate: 0.0060 ng/cm2; NA: non-applicable; ND: non-determined (no statistics were done); BSC: biological safety cabinet; CP: cyclophosphamide; IF: ifosfamide; MTX: methotrexate; CSTD: closed-system drug transfer device. The rows in bold represent the total of the sites in a) the pharmacy (BSC + delivery + validation) and b) the pharmacy (counter + floor).
Regarding the concentrations of CP, IF and MTX in ng/cm2 before and after using a CSTD for hazardous drugs preparation, there was no statistically significant difference between Phases I and III for IF and MTX. Hazardous drug concentration measured was below the LOD for most sample sites in Phase III except floor in the front of the BSC for CP and IF.
Evaluation of the level of appreciation
A total of 3/5 (60%) of the technician that participated in our survey had two or more years of experience with hazardous drugs preparation. All of the pharmacy technicians (n = 5) indicated that the centralization of hazardous drug priming was as easy as it was using current practices. However, 40% of the pharmacy technicians found that centralized priming was slower and 80% found it more cumbersome than when they used current practices. No pharmacy technician reported an increase in the number of technical issues or in their perceived risks of absorbing drugs, injury or spillage.
With respect to the use of the PhaSeal® CSTD for the preparation of CP, IF and MTX, 100% of the pharmacy technician found that using the CSTD increased technical issues and the risk of spillage, 80% considered that the CSTD was slower and more cumbersome to use and 60% considered that using a CSTD was more difficult and increased the risk of drug absorption through the skin and by inhalation.
During the study, some difficulties were met concerning the CSTD use, including the appearance of particles in vials and a problem of MTX vials pressure balance. During the second week of training with the PhaSeal® CSTD, some pharmacy technicians noted the presence of particles in two MTX and CP vials. These particles seemed to come from the vials’ protective rubber stopper after the pharmacy technician perforated the vial membrane only three times with a different Injector®. Moreover, two major CSTD-related incidents occurred during training and Phase III of the study. The pharmacy technicians had trouble with pressure balances in the MTX vials (100-mL format). The Protector® was ejected from the vial twice and the drug flowed profusely inside and outside the BSC. The BSC and floor of the sterile room required a thorough clean-up after these incidents.
Discussion
Centralization of priming
In our study, centralized priming did not lead to a significant difference in the number of positive samples in the hematology-oncology satellite pharmacy and care unit. However, centralized priming with NaCl 0.9% in the hematology-oncology satellite pharmacy was safe for the staff and for the patients. It maintained preparations in a sterile environment and minimized risks associated with spills and splashes of chemotherapy by nurses. The quantities of hazardous drugs compounded during phase II were higher than those in phase I, which might have led to a higher contamination level in the pharmacy during Phase II. However, this was not the case. Also, the introduction of centralized priming was associated with a significant reduction of detected median CP and IF concentrations on the floor in front of the cytotoxic waste container in the patient care unit. While there is still limited data about the impact of centralized priming on surface contamination, we do believe it is an appropriate and feasible practice and it does not increase surface contamination within the pharmacy.
Using a CSTD for hazardous drugs preparation
The proportion of positive samples in the BSC was reduced from 60% to 0% between Phases I and III. The study confirms findings previously published on the PhaSeal® CSTD’s ability to reduce the proportion of positive samples and the surface concentration for most sampling sites.3–15 While our study confirms the efficacy of CSTDs in a controlled study in which there was a recognized observation bias, we do believe ergonomical and economical issues must be further studied to confirm the cost-effectiveness ratio and value of CSTDs in healthcare settings. Following this study, CSTDs were not implemented in our setting. Periodical surface monitoring was performed in our center and confirmed low surface contamination. It has to be considered that there does not exist any safe occupational exposure limit. In this context, surface concentration of hazardous drugs should be kept as low as reasonably achievable.
Some technical issues associated with the PhaSeal® CSTD use arose during the study. With respect to the presence of particles in the vials, the company stated that it was safe to perforate the protective membrane of a vial up to ten times without any CSTD-related problems. However, over the course of the study, particles appeared in the protective membrane of two MTX (20 mL) and CP (100 mL) vials after inserting the PhaSeal® Injector® just three times. The clinical impact of the presence of these particles in the vials and in patients (if not detected) may represent a risk to patient safety. Surprisingly, the presence of particles in the vials with the use of the PhaSeal® CSTD is not described in the literature, although the manufacturer has verbally indicated that they have been notified of other cases than ours. We also experienced two spills with MTX vials. The most probable hypothesis that would explain these incidents would be a pressure balance problem. Given that air could not be transferred in the head space of the Protector®, since the filter was blocked by MTX, the pressure inside the vials became excessive and caused the ejection of the Protector®. This issue had already been reported in a previous study. 12 The technical issues experienced by the pharmacy technicians explain why their opinion differs from the actual reduction in contamination that was found.
Limitations
This study has limitations. It compared two techniques (i.e. pharmacy priming and CSTDs), but did not measure the impact of CSTDs in patient care areas. A significant observation bias should be considered as a research assistant has been present continuously to support the use both techniques. All staff were retrained and supported daily by a research assistant to optimize the use of CSTDs and to help resolve any technical issues. Other studies evaluating CSTDs in usual working practices still found some traces of hazardous drugs on surfaces.4–16 The surface contamination on the care areas was not evaluated while using a CSTD. Instead, additional samples sites were evaluated in the pharmacy. Satisfaction evaluation was limited to five pharmacy technicians.
Conclusion
The centralization of the priming of IV tubing for chemotherapy did reduce floor contamination in patient care areas without increasing surface contamination in pharmacy areas. CSTDs did reduce contamination in the pharmacy, but pharmacy technicians experienced technical issues with the device. Further studies are required to evaluate the cost-effectiveness ratio of both techniques considering the staff workload of centralized priming and the acquisition costs of CSTDs.
Footnotes
Acknowledgements
We would like to thank Karine Touzin, research assistant at the time of the study and Michel Lefebvre and Eric Langlois for the Institut national of Santé Publique du Québec for their contribution to surface contamination measurements.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None