
Abstract
Pseudocellulitis has been previously described with the use of chemotherapy agent gemcitabine. This condition is thought to occur due to vascular toxicity and increased localized permeability of the skin capillaries. We report herein a case of recurrent pseudocellulitis due to gemcitabine in a patient with metastatic pancreatic cancer. We believe this condition is underreported and underrecognized. Furthermore, it may be misdiagnosed as cellulitis and inappropriately treated with systemic antibiotics. As the diagnosis is clinical and the condition is self-limited, referral to other specialists is usually not required. Awareness of gemcitabine-induced pseudocellulitis is important in order to reassure the patients, their families, and non-oncology providers and to avoid unnecessary (and often costly) diagnostic work-up.
Introduction
Gemcitabine (2,2-difluorodeoxycytidine) is currently being used in the therapy of a variety of solid and hematologic malignancies. Gemcitabine has been associated with thrombotic and vascular side effects, including toxicity to skin blood vessels and capillaries. 1 We report herein a case of recurrent pseudocellulitis related to the use of gemcitabine in a patient with adenocarcinoma of the pancreas.
Case report
A 72-year-old Caucasian man presented with abdominal distention, weight loss, icterus, fatigue, along with intermittent nausea and vomiting. He was a former smoker with a 40-pack-year history and had used excessive alcohol amounts for over a decade in his 30s and 40s but desisted since. Past medical history was remarkable for a well-controlled diabetes mellitus type 2, hypertension, hyperlipidemia, Hashimoto’s thyroiditis, and gastroesophageal reflux disease. Family history was remarkable for pancreatic cancer in his father at the age of 72. His diabetes was in excellent control with insulin. Hypertension and hypothyroidism were managed successfully with lisinopril and levothyroxine, respectively.
Physical examination revealed moderate jaundice and pallor, as well as left upper quadrant tenderness and moderate hepatomegaly. A laboratory evaluation showed direct hyperbilirubinemia and a moderate elevation of transaminases. Serum carcinoembrionic antigen (CEA) and cancer antigen 19-9 (CAA19-9) levels were also moderately elevated. Evaluation with an abdominal ultrasound showed a questionable mass in the pancreatic head. A computed tomography (CT) scan revealed a 3.0 × 2.8 cm soft tissue mass in the head of the pancreas and uncinate process with associated pancreatic ductal and adjacent biliary ductal dilatation. No liver or other metastases were appreciated. A Whipple procedure was performed, and pathology was consistent with a moderately differentiated exocrine adenocarcinoma of the pancreatic head with invasion into the common bile duct and several peripancreatic lymph nodes. Intraoperatively, the operating surgeon noticed a suspicious area in the right lobe of the liver adjacent to the liver capsule. Wedge resection at that location identified liver metastases (stage T3N1M1); the margins were positive. The patient was started on single-agent gemcitabine at the dose 1000 mg/m2 weekly, which he tolerated fairly well. The only side effects were mild normocytic anemia and moderate bilateral pedal edema. Given the status post Whipple surgery, he was also treated with monthly IM cyanocobalamin injections in order to prevent vitamin B12 deficiency. Two months later, CEA and CA 19-9 levels almost normalized, and a restaging CT scan of the abdomen and pelvis showed no evidence of liver metastases.
However, on week 8, the patient developed multiple painless beefy-red lesions on his legs. He denied fever, chills, or other constitutional symptoms. Physical examination revealed confluent macular erythematous skin lesions involving bilateral lower extremities and measuring 1.0 cm in the largest diameter (Figure 1(a) and (b)). The lesions would blanch upon local pressure. Pseudocellulitis was immediately suspected, and no further therapy was administered. Gemcitabine was continued as the patient had responded well to this therapy. The patient’s lesions resolved spontaneously within two weeks. Three weeks later, the lesions reoccurred; however, they were less numerous and rather pink than red this time around. They too disappeared within a week and did not reoccur despite continuation of gemcitabine therapy. The patient was offered abundant reassurance.
(a) Pseudocellulitis featuring confluent macular erythematous skin lesions involving bilateral lower extremities. (b) Skin of the lower extremities affected by the same process (closer view).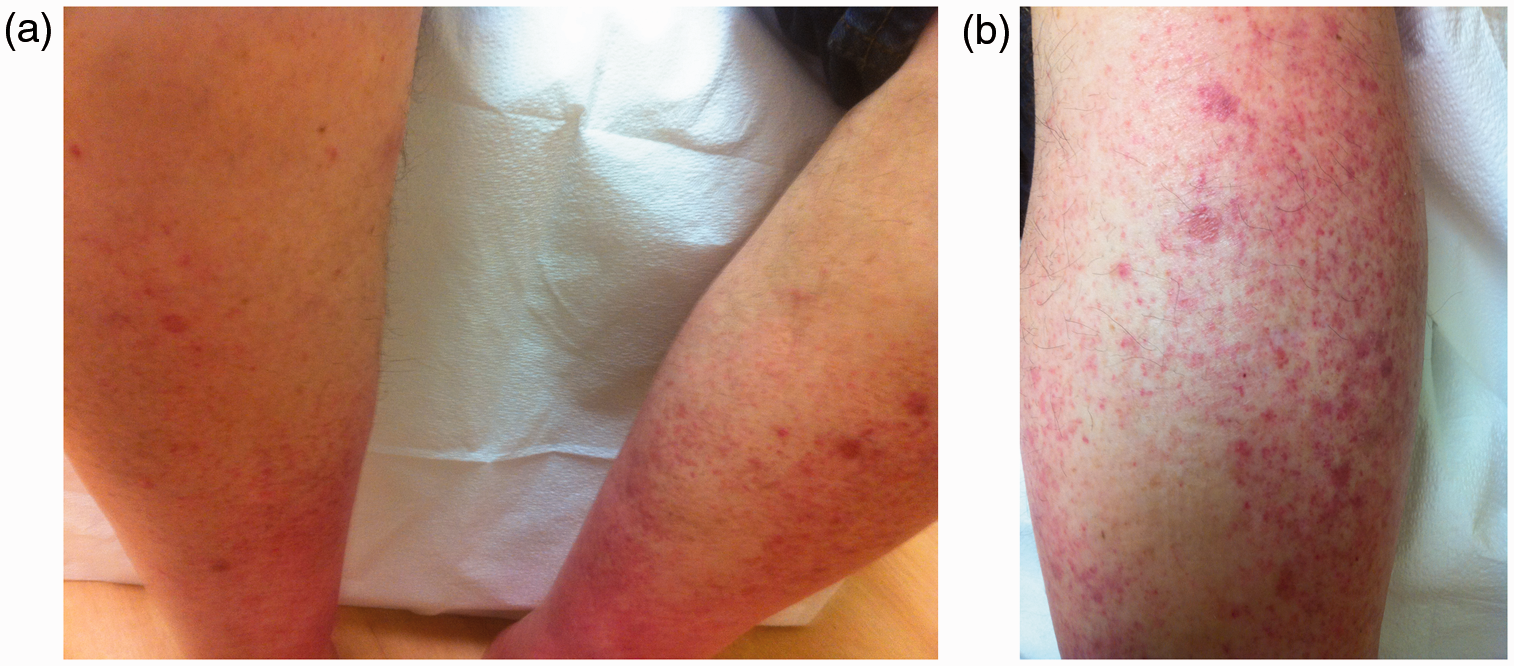
Discussion
A detailed past medical history, including a thorough drug history, is of utmost importance when evaluating patients with various skin lesions. The key feature in this case is to recognize that the skin lesions presented above are due to gemcitabine use.
Chemotherapy agents have been associated with a variety of skin lesions such as photosensitivity, radiation recall dermatitis, and hypersensitivity reactions. 2 Cutaneous reactions to gemcitabine are not infrequent and include rash, alopecia, pruritus, and hyperpigmentation.3,4 The most common one is a self-limited rash occurring in up to a quarter of patients.
Pseudocellulitis resembles cellulitis but features an uncomplicated non-necrotizing localized inflammation of the dermis and hypodermis of non-infectious etiology. These lesions are thought to occur due to increased permeability of the skin capillaries. 1 They disappear when the lesion is depressed and blood is squeezed from the skin vessels. Pseudocellulitis has been described in areas of preexisting lymphedema and tends to reoccur with re-exposure in the same areas.4,5 Distinguishing the non-infectious causes of skin inflammation from bacterial cellulitis may prove challenging as their clinical features are similar, and a specific pathogen is not isolated in most cases of skin infections. 5
Resembling pseudocellulitis, radiation recall dermatitis is characterized by an inflammatory reaction in an area previously treated with radiotherapy that develops hours to days after the first exposure to a precipitating agent. Affected skin may display maculopapular, desquamative, vesicular, or ulcerative lesions ranging in severity from a mild rash to severe skin necrosis, sometimes in a radiation dose-dependent fashion. 5 Gemcitabine is not infrequently associated with radiation recall reactions; therefore, caution is imperative when co-administering this agent with radiation therapy.1,5,6
We believe that pseudocellulitis due to gemcitabine is both underreported and underrecognized. Of course, a cancer patient with fever and erythematous skin lesions while on gemcitabine should always have blood cultures done and start systemic antibiotics. Nonetheless, fever is a known side effect of gemcitabine, affecting up to 25% of patients. As a result, many of these patients perhaps have both pseudocellulitis and fever due to gemcitabine. Heightened clinical suspicion is necessary in afebrile patients with characteristic erythematous lesions receiving therapy with gemcitabine as they likely suffer from pseudocellulitis. Unfortunately, there are no studies exploring the role of serum markers such as C-reactive protein or procalcitonine to distinguish between cellulitis and pseudocellulitis. The reason behind this is probably the rarity of pseudocellulitis as well as lack of clinical suspicion for this entity. These investigations are perhaps the task of future research.
Review of the literature identified very few cases of pseudocellulitis, and we postulate that gemcitabine was the probable etiologic agent in the presented case. First, it was the only new agent the patient was taking at that time. None of his older drugs, namely insulin, lisinopril, or levothyroxine has been known to be associated with these particular skin changes. Our hypothesis is further supported by the fact that the patient experienced pitting pedal edema, a well-known side effect of gemcitabine. Notably, the pathogenesis of pedal edema also involves increased permeability of the skin venules and capillaries. In addition, the bilateral lower extremity skin lesions reoccurred as gemcitabine was continued. According to the Naranjo’s nomogram, the causality relationship is at least probable if not definite that gemcitabine induced the pseudocellulitis in our case.
As opposed to cellulitis or a severe skin allergic reaction, lesions of pseudocellulitis are neither painful nor dangerous for the patient. The diagnosis is usually clinical. In all reported cases (including ours), this toxicity was self-limited. No interruptions of gemcitabine schedule were undertaken, although some authors prescribed antibiotics. As of today, a high level of clinical suspicion though continuous medical education is necessary in order to avoid antibiotics in this setting as they can lead to unwanted side effects, development of Clostridium difficile colitis, or resistance to antimicrobial agents.1,2 Referral to other specialists or hospitalizations are usually not required. Diphenhydramine and/or non-steroidal anti-inflammatory agents may have a role in the management of symptomatic patients. 2 In patients responding to gemcitabine, this agent can be safely continued as the lesions are completely reversible within one to two weeks.
Physician awareness of gemcitabine-induced skin injuries such as pseudocellulitis is important in order to provide reassurance and avoid unnecessary (and often not inexpensive) diagnostic work-up.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.