
Abstract
Stevens–Johnson syndrome/toxic epidermal necrolysis overlap is an acute hypersensitivity reaction that compromises the integrity of mucous membranes and cutaneous tissue. While the pathophysiology of this syndrome has not been fully elucidated, it is commonly associated with the medication use and carries a significant mortality risk of approximately 30%. No commonalities among causative medications have been identified, and determining the offending agent can be challenging. This case report describes fatal Stevens–Johnson syndrome/toxic epidermal necrolysis overlap in a patient after receiving his first cycle of allopurinol, rituximab, and bendamustine treatment for non-Hodgkin’s B-cell lymphoma. An analysis of FDA Medwatch adverse reaction case reports involving allopurinol, rituximab, and bendamustine is also presented.
Keywords
Introduction
Stevens–Johnson syndrome (SJS), Stevens-Johnson syndrome/toxic epidermal necrolysis overlap (SJS/TEN), and toxic epidermal necrolysis (TEN) are a spectrum of acute hypersensitivity reactions based on body surface area skin detachment of <10%, 10–30%, and >30%, respectively. Compromised mucocutaneous tissues with extensive tissue sloughing and separation of the first epidermal layer are defining characteristics. Numerous medications with diverse indications have been reported as the potential causes of these life-threatening and potentially fatal skin reactions, yet no commonalities have been identified that predict the risk of reaction.1,2 Allopurinol, bendamustine, and rituximab have all been demonstrated to cause variable skin toxicities, some of which have progressed to severe, life-threatening, and fatal toxicity.3–13 Here, we present a case report where the concomitant use of allopurinol, rituximab, and bendamustine induced fatal SJS/TEN in a patient with non-Hodgkin’s B-cell lymphoma.
Case report
Rituximab + bendamustine chemotherapy regimen.
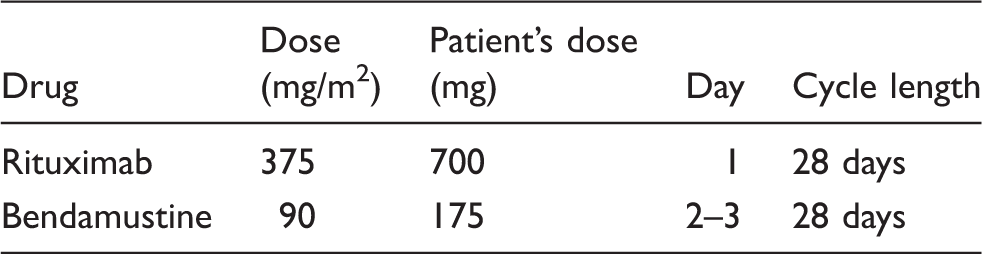
Fourteen days after starting chemotherapy, the patient presented to his local hospital with a 3-day history of sore throat, extreme fatigue and weakness, severe pain throughout his skin that was aggravated by even slight touch, and a widespread non-pruritic macropapular rash. The patient had extensive skin sloughing of multiple body surfaces and mucous membranes as well as fragile skin throughout the remainder of his body. He received supportive care and, upon stabilization, was immediately transferred to our facility for treatment the day of his admission.
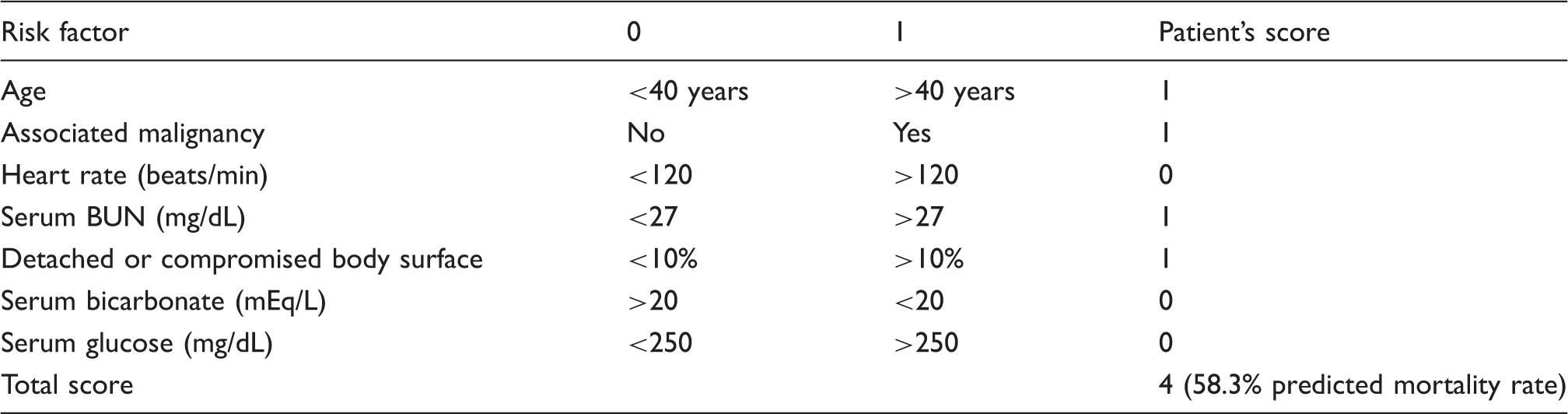
The patient was admitted to the burn surgery service for further assessment where tissue involvement was noted to include the patient’s face, anterior and posterior trunk regions, upper and lower extremities, oral mucosa, ocular conjunctiva, and genitalia, all of which were Nikolsky’s sign positive. The Lund–Browder Burn calculation was used to determine the percentage of total body surface area affected and estimated 14% involvement, consistent with a diagnosis of SJS/TEN.2,14 The patient was also tachycardic, hypotensive, and febrile. Allopurinol was discontinued following confirmation that the patient had taken the medication as directed for 13 days with his last reported dose being the day before hospital admission. Supportive care measures including hydration, wound debridement, systemic and topical antibiotics, ophthalmic irrigation and lubrication, nutritional support, and pain management were provided. With further progression of symptoms, the patient requested palliative measures and died secondary to complications of SJS/TEN.
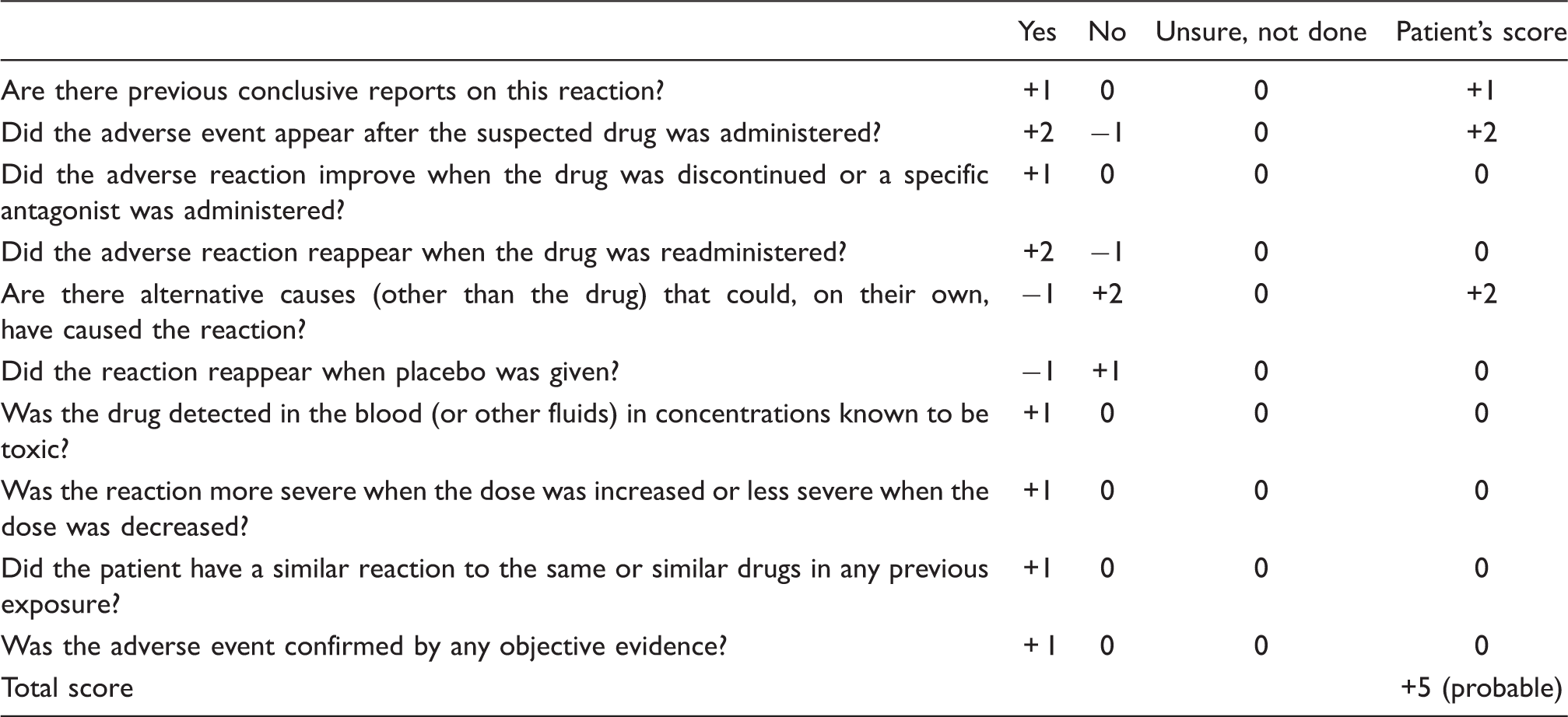
The patient had recently started palonosetron, dexamethasone, prochlorperazine, allopurinol, rituximab, and bendamustine as part of his treatment regimen and continued to take maintenance medications including vitamin D, aspirin, levothyroxine, and lorazepam. He had no known medication allergies and had not been previously treated with allopurinol, bendamustine, or rituximab.
Naranjo ADR probability scale. 16
SCORTEN severity-of-illness index. 16
FDA Adverse Event Reporting System TEN case reports from October 30, 2008 to October 30, 2013—unless noted all data in parenthesis is % of TEN cases.
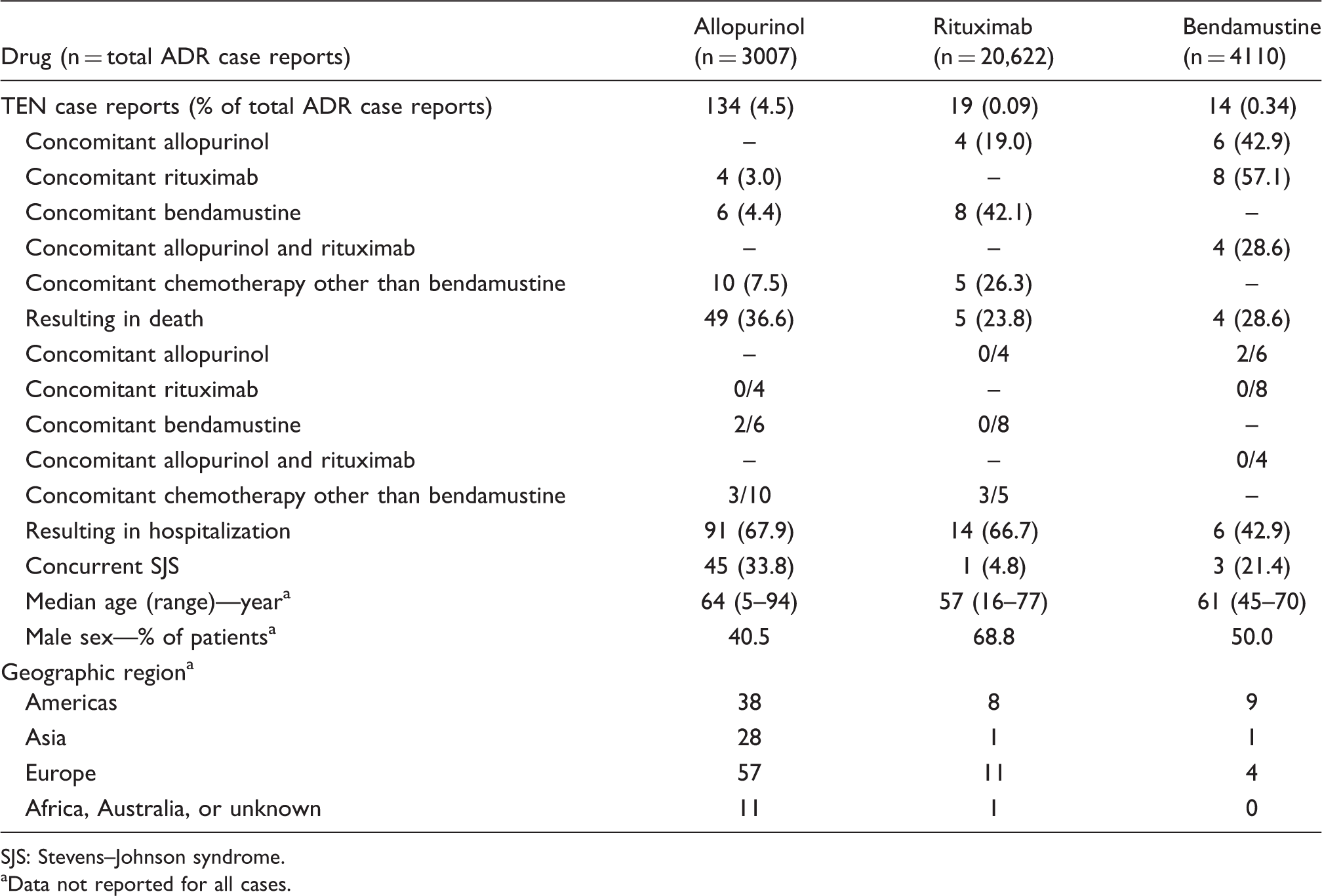
SJS: Stevens–Johnson syndrome.
Data not reported for all cases.
Allopurinol had the fewest total adverse drug reaction reports but the highest number of TEN reaction reports at 134, which was seven times higher than that reported for rituximab and approximately 10-fold higher than for bendamustine. Percentage of allopurinol TEN reactions resulting in patient death was also the highest at 36.6%, followed by bendamustine at 28.6% and rituximab at 23.8%.
Out of four TEN case reports of patients that received concomitant allopurinol, rituximab, and bendamustine, none died; however, two out of six patients that received concomitant allopurinol and rituximab died. TEN reactions due to allopurinol and rituximab resulted in a similar percentage of hospitalized patients with reactions due to bendamustine resulting in fewer hospitalizations. While eight of 19 rituximab TEN reactions occurred with concomitant bendamustine, another seven rituximab reactions occurred without concomitant allopurinol, bendamustine, or non-bendamustine chemotherapy (data not included in table). Three of 14 bendamustine reactions occurred without concomitant allopurinol or rituximab.
Discussion
Allopurinol is a xanthine oxidase inhibitor, which blocks uric acid formation, and is utilized as prophylaxis in patients with an elevated risk of hyperuricemia and tumor lysis syndrome. It is generally well tolerated; however, it is known to cause hypersensitivity reactions including rash that may progress to more severe skin reactions including SJS, SJS/TEN, and TEN.5–8 It is of interest that 4.5% of all reported FDA Medwatch allopurinol adverse effect reports were TEN reactions, a relatively large percentage. Only 12% of these cases occurred in the setting of chemotherapy, six of which were with concomitant bendamustine. It is possible that our patient may not have encountered this serious adverse effect or may have developed a more mild to moderate case had he taken a shorter course of allopurinol than 13 days. A retrospective study did show that immediate withdrawal of potential offending drug at the onset of SJS/TEN symptoms decreased the risk of death. 17 FDA Medwatch data do not routinely ascribe duration of therapy but this would have been an interesting contribution to our analysis.
Rituximab is a monoclonal antibody used as a chemotherapeutic agent to target CD20 + blood cells. Rituximab can cause severe mucocutaneous reactions, some with fatal outcomes. Case reports have linked rituximab with SJS, SJS/TEN, and TEN as well as paraneoplastic pemphigus, lichenoid dermatitis, and vesiculobullous dermatitis.9–11 Our patient would be the first patient reported to FDA Medwatch that died secondary to a SJS/TEN reaction following allopurinol, rituximab, and bendamustine exposure. Of course, it is possible that rituximab use was underreported in patients receiving this treatment regimen as rituximab as a causative agent of SJS/TEN is rare, and some would argue controversial. 11 It is noteworthy that no deaths occurred among the FDA Medwatch TEN cases of concomitant allopurinol and rituximab, bendamustine and rituximab, or a combination of the three drugs. Three of five patients that received rituximab with concurrent chemotherapy other than bendamustine died and were the majority of rituximab-related deaths. The first of these patients received cyclophosphamide, the second received fludarabine, cyclophosphamide, doxorubicin, and vincristine, and the third received cyclophosphamide, methotrexate, vincristine, and doxorubicin. Case studies of TEN have been reported for cyclophosphamide, fludarabine, methotrexate, and doxorubicin. A black box warning for TEN is included in the methotrexate package insert.
Bendamustine is a nitrogen mustard compound that functions as a chemotherapeutic agent with both DNA alkylation and anti-metabolite properties. Phase II clinical trial and post-marketing reports demonstrated rare cases of severe, life-threatening skin reactions including SJS and TEN.12,13 To date, there are no published reports demonstrating that bendamustine alone causes SJS, SJS/TEN, or TEN; however, a single case reported that single agent bendamustine caused a severe cutaneous interface drug eruption. 4 In the bendamustine package insert, it is noted that SJS and TEN have been reported with concomitant allopurinol and other medications known to cause these severe skin reactions. 12
As allopurinol, bendamustine, and rituximab have all been known to cause severe skin reactions, questions remain regarding which agents are causative when, and whether or not the possibility of an additive risk of SJS/TEN when multiple drugs known to be associated with SJS/TEN are administered concomitantly. Given the severity of the reaction and the high-mortality risk, re-challenging one or more drugs in patients to fully elucidate the underlying cause of SJS/TEN is not acceptable. FDA Medwatch data have several limitations. There is no certainty that the reported adverse events are actually due to the drug identified, and submission of reports is voluntary and dependent on a broad variety of factors. The information from these reports cannot be utilized to calculate adverse event incidence. While difficult to draw strong associations with these limitations and the limited number of TEN case reports, the available Medwatch data on concomitant allopurinol, rituximab, and bendamustine use available at this time do not show additive risk.
Conclusion
While the incidence of SJS/TEN is rare, the overall mortality rate of patients with this adverse effect is approximately 30%. It is important to identify symptoms and disease progression early, remove potential offending agents immediately, and provide optimal supportive care to promote recovery and reduce mortality. Quantifying additive risk of this rare adverse effect from use of concomitant medications associated with this reaction such as allopurinol, rituximab, and bendamustine remains a challenge.
It is important to recognize that tumor lysis syndrome is a potential serious adverse effect that must be closely monitored. If allopurinol is deemed necessary as tumor lysis prophylaxis in treatment regimens containing rituximab and bendamustine, it is probably rational to utilize as short of course as is clinically required with close monitoring. Consideration of avoidance of allopurinol in patients with low risk for tumor lysis syndrome is likely clinically appropriate.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.