
Abstract
The most common metastatic sites of colorectal cancer are liver, lung, peritoneum and lymph nodes. Metastasis of colorectal carcinoma to palatine tonsil is rarely seen. To our knowledge, only 11 patients were documented in English literature. Atypical metastases can sometimes lead to misdiagnosis. Precise diagnosis of atypical metastases requires a careful physical examination, good imaging method and comprehensive pathological evaluation. Here, we report a case of rectal adenocarcinoma presented with palatine tonsil metastasis.
Introduction
Metastatic malignancies of the palatine tonsil are rarely seen and the most common malignancies of palatine tonsil are lymphomas and squamous cell carcinomas. 1 Metastatic tumors of tonsillar palatine account for only 0.8% of all tonsillar malignancies. 1 The most common primary malignancies spread to palatine tonsil are lung, breast, renal cancers, and malign melanoma.2–5 In the English literature, metastases of colorectal cancer to palatine tonsil were reported only in 11 cases. 6 Herein, we report a case of rectal adenocarcinoma who presented with palatine tonsil metastasis.
Case report
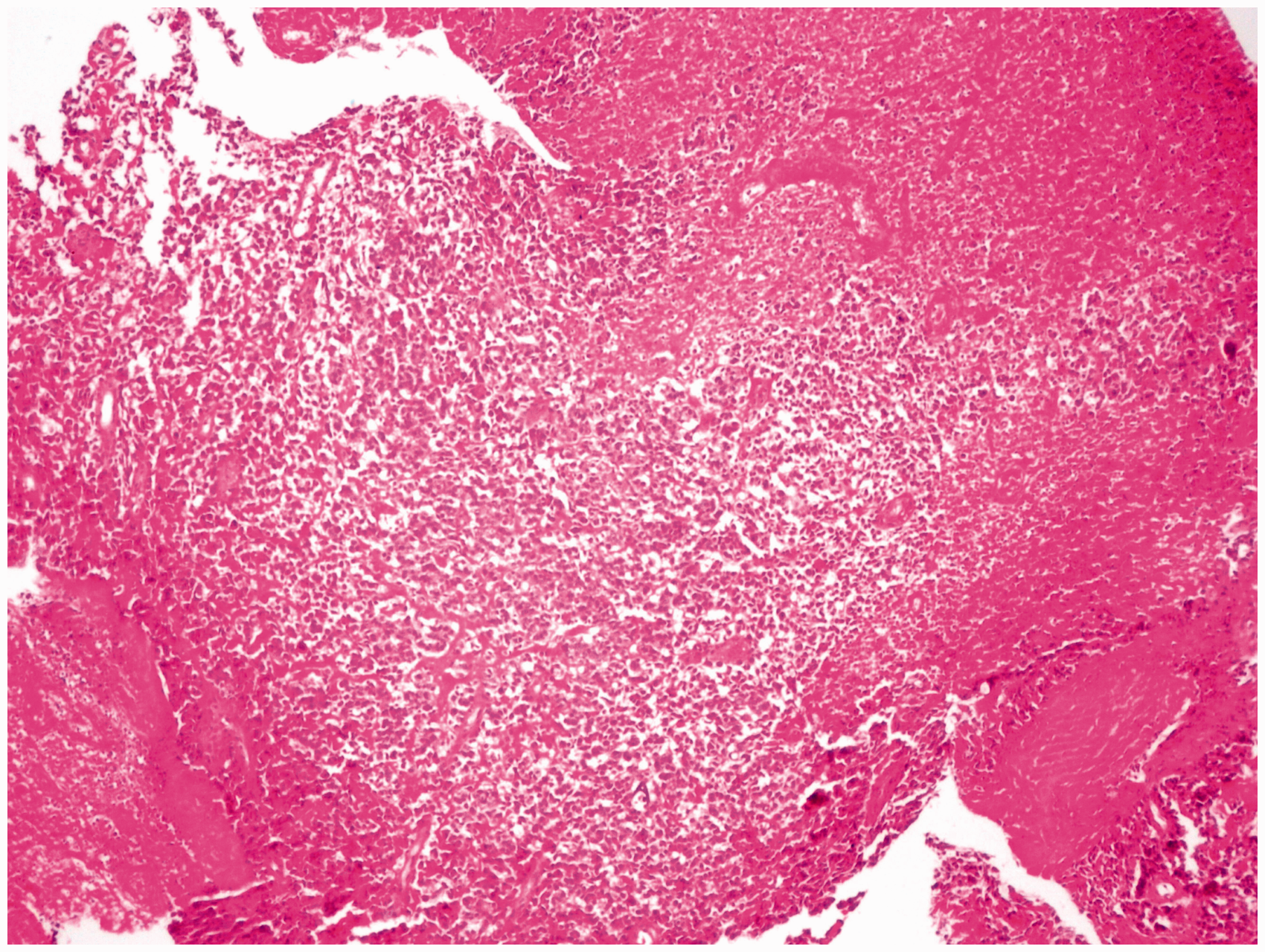
A 45-year-old Syrian woman with complaints of constipation, suprapubic pain and a painful mass on the left palatine tonsil persisting for two months was admitted to our clinic. On physical examination, an ulceronecrotic mass of 4 cm diameter was observed on left palatine tonsil (Figure 1). At digital examination, there was a mass on the rectum located at 3 cm from the anal verge. There was no significant finding on family history. Her medical history was unremarkable. She was a non-smoker with had no history of alcohol abuse. A colonoscopy examination was performed and an ulcerated-vegetative and necrotic tumor located at 3 cm from the anal verge was found. Tumor was almost occluding the lumen of the rectum and was 4 cm in length. Biopsy revealed poorly differentiated adenocarcinoma of the rectum. Diagnosis of rectum adenocarcinoma was established and examination of thorax computed tomography (CT) and abdomen magnetic resonance imaging (MRI) was requested for staging. Serum CA 19-9 level was normal as 25.37 U/ml (N < 37), and serum carcinoembryonic antigen (CEA) level was elevated as 69.67 ng/ml (N < 2.5). Thorax CT was normal. Abdomen MRI showed a 1.4 cm metastatic mass in the segment 2 of the liver, thickening of rectal wall and parailiac multiple lymph nodes in 1.5 cm diameter. A biopsy of tonsillar mass was made and showed metastasis of poorly differentiated adenocarcinoma of colorectal origin (Figure 2). Immunohistochemical characteristics of the metastatic tumor were positive for cytokeratin 20 (CK 20) and intestinal specific transcription factor (CDX2) and negative for cytokeratin 7 (CK7). A positron emission tomography (PET/CT) scanning was planned. Enhanced [18F] fluoro-2-deoxy-D-glucose (
18
F-FDG) uptake in rectum wall, parailiac lymph nodes, hepatic mass and left palatine tonsil palatine was observed. Chemotherapy regimen of XELOX (oxaliplatine 130 mg/m2 bolus infusion on day 1 and capecitabine 1500 mg/m2/daily on days 1–14 every three weeks) was started. After the first cycle of XELOX, nearly 30% reduction on the tonsillar tumor size was observed. Radiotherapy for pain palliation on the primary tumor site was applied and a colostomy was performed. After four cycles of XELOX the disease progressed and FOLFIRI regimen (irinotecan 180 mg/m2 IV over 90 min, leucovorin 400 mg/m2 IV over 2 h, 5 fluorouracil 400 mg/m2 IV bolus infusion and 5 fluorouracil 2400 mg/m2 IV 46-h infusion every two weeks) was started. After two cycles of FOLFIRI, multiple papulonodular lesions were observed on the perineal region. Biopsies of these lesions confirmed the metastasis of rectal adenocarcinoma. Decision of disease progression was made and chemotherapy was stopped. Performance status of the patient deteriorated rapidly. Eight months after diagnosis, the patient died due to disease progression.
Image of the ulcerated-vegetative mass on left palatine tonsil. Microscopic appearance of the mass on left palatine tonsil showing solid, non-gland form, and atypical epithelial cells with necro-inflammatory exudate (Hematoxylin and Eosin, ×40).
Discussion
Metastasis of colorectal cancer to palatine tonsil is extremely rare. 6 This is the 12th reported case of colorectal cancer with tonsillar metastasis in English Literature. The presented case was clearly defined with physical finding, proper imaging methods and pathological features. In our case, immunohistochemical staining of tonsillar metastasis was positive for pan-cytokeratin, CK 20 and CDX2 but negative for common leucocyte antigen (CLA) and CK 7. Generally, colorectal cancers are positive for CK20 and CDX2 and negative for CK7. 7
Atypical metastases are interesting because the physiopathology of these rare coincidences cannot be explained clearly in the majority of cases. Some hypotheses were suggested to explain the metastatic spread of cancers to tonsils. Retrograde cervical lymphatic spread through the thoracic duct and hematogenous transmission through the systemic arterial vasculature or the paravertebral (Batson) plexus are the most prominent. 6 Also, traumatic procedure seeding the tumor to tonsils has been reported. 8
Clinocopathologic characteristics of patients with tonsillar metastasis from colorectal cancer.
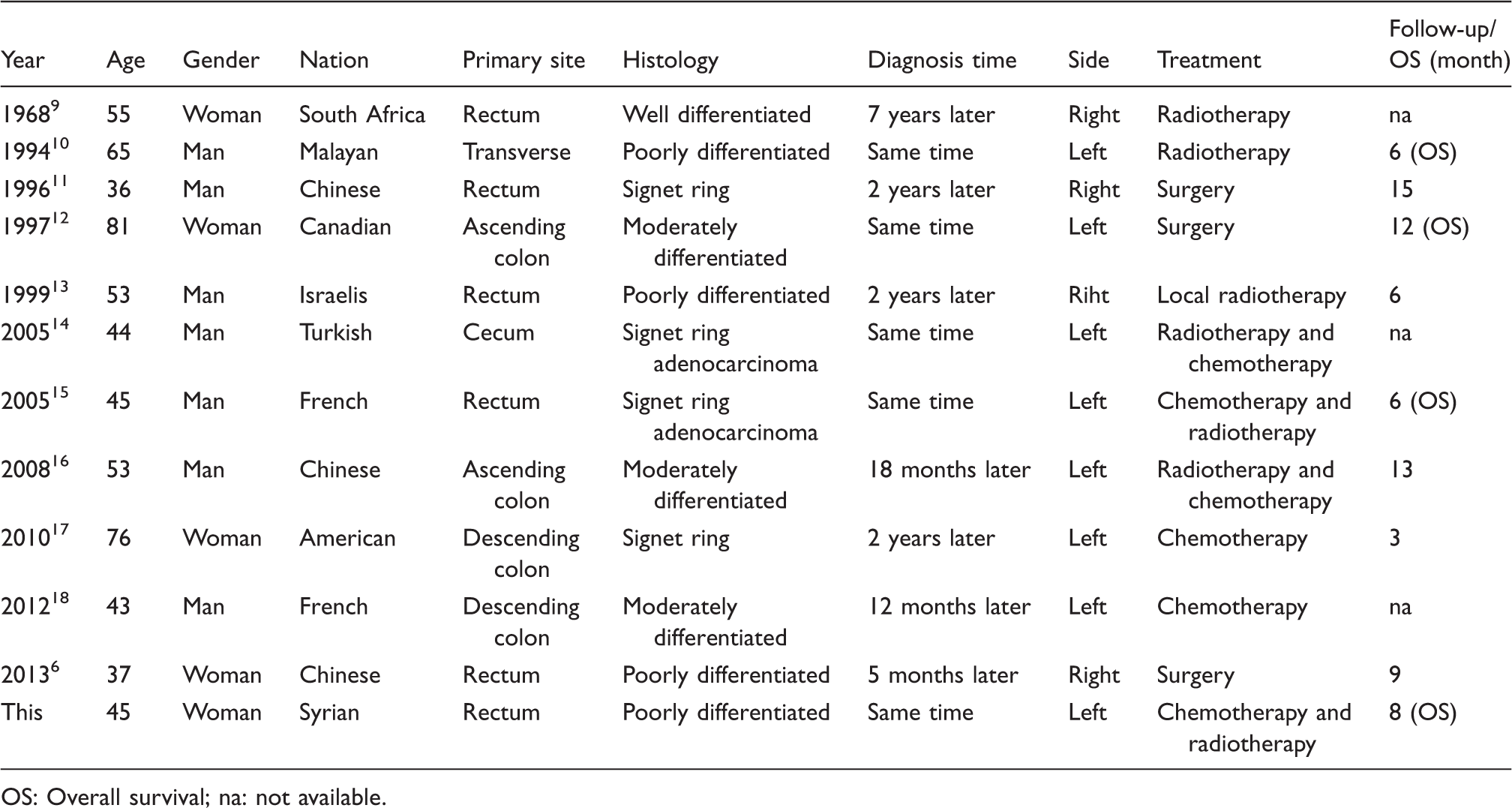
OS: Overall survival; na: not available.
If a patient with colorectal cancer complains of a mass on palatine tonsil on physical examination, metastasis of colorectal cancer to tonsil should be kept in mind. In such conditions, a through physical examination, good imaging methods and pathologic examination are necessary for a precise diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.