
Abstract
Objectives
To use a mobile air decontamination unit (MADU) for a microbial destruction and decreased particle burden making a cleanroom controlled environment in a Centralized Chemotherapy Preparation Unit (CCPU). Good manufacturing practices (GMP) in France specify that the ambient air in the vicinity of a class III biosafety cabinet (isolator) complies with air cleanliness ISO 8 level in CCPU. This guideline has a significant impact because implementing a dedicated air handling unit (AHU) brings some engineering constraints and generates substantial additional costs.
Methods
Authors have previously studied some technical and economical aspects to evaluate the feasibility of the MADU option.
Results
Using a MADU was the chosen option. Qualification of the CCPU showed that results were in compliance with the French GMP. After one year of use, the efficiency of the MADU was confirmed. According to these results, using a MADU constitutes a beneficial option for CCPU previously equipped with an isolator when compared to renovation work involving a standard built-in AHU.
Introduction
Upgrade to compliance impacts
Chemotherapy drug preparation in hospital environments is a high-risk process. Sterile cytotoxic preparations using aseptic techniques must be performed in a grade A environment (ISO class 5) within a class II or III biosafety cabinet. 1 Class III biosafety cabinets (isolators) involve a physical barrier between the protected internal work space and the surrounding environment as opposed to lower grade ones. Therefore, no specific air cleanliness compliance was specified for the ambient room around isolators before 2007 in France. Indeed, since the official publication of the French Good Manufacturing Practice (GMP) in December 2007 as “Bonnes Pratiques de Préparation”, new recommendations must be taken into account for Centralized Chemotherapy Preparation Units (CCPU). French GMP reiterates that the compounding process for sterile and hazardous products requires a grade A environment in the preparation area. In addition, French GMP clarify that for a positive pressure isolator, the immediate environment requires a class D (ISO 8) level. This guideline has a significant impact for CCPUs previously equipped with isolators (in our case, a positive pressure isolator (IPC 2000, Sieve®, France)) because positive pressure isolators are widely used in France and most of them were placed into uncontrolled rooms.
Implementing a dedicated air handling unit (AHU) brings some engineering constraints and generates substantial additional costs. In particular, for renovation work, this requires an air duct network extension involving the dismantling of temporary ceilings which due to massive dust generation impacts on the continuity of usual activity which may need to be reorganized, or temporarily transferred to a remote location for around two weeks.
Air quality before upgrade to compliance
According to the quality management system of the CCPU, an independent laboratory (APTE, Pompey, France) had performed twice-yearly particulate and microbial air quality controls in the surrounding environment of the isolator. Thus, these controls had revealed that the airborne contamination were already close to the class D (ISO 8) specification without dedicated air treatment system. In fact, APTE had measured e.g. 1,297,668 particles >0.5 µm per m3; 3137 particles >0.5 µm per m3 and 150 Colony forming unit per plate, while limits for class D are: 3,500,000 particles >0.5 µm per m3; 20,000 particles >5 µm per m3 and 200 Colony forming unit per m3. We can explain these results by a complete set of precautionary measures undertaken to reduce the contamination risk (room set-up, smooth surfaces, specific personnel outfit, hand-hygiene, etc.). However, the absence of an air decontamination system still implied that there were no efficient measures to compensate a potential alteration of the ambient air quality.
The mobile air decontamination unit
A mobile air decontamination unit (MADU) is a medical device designed to reduce the risk of infection for immune-suppressed patients by decreasing particle and microbial burden. This type of equipment is henceforth commonly used in this medical application.2–5 Among the MADU placed on the market, for the Department of Medical Oncology, the hospital selected the Plasmair™ system (Airinspace SE, Montigny-le-Btx, France). This electro-medical equipment has been qualified as class I medical device (EU) and is US FDA registered as class II medical device (510(k) number K070722). It is based on a proprietary technology that combines HEPA-grade filtration (>99.97% on particles of diameter ≥0.3 µm) with cold-plasma-induced microbial destruction. This choice was based on a evidence-based performance and perspective over several years of use since its market introduction in 2004,6,7 a strong distribution in healthcare environments and facilitated purchase process with its registration with the French central purchasing body UGAP.
Methods
Targets and feasibility
Considerations for potential use of this device for the CCPU to upgrade the area to compliance originate both in the decontamination capacities of the unit (1log reduction with unfavorable conditions) with respect to the performance targets and the support brought to the project in 2010 by the regional oncology network (Oncolor) and the regional healthcare agency (ARS Lorraine) which coordinated the regulation file.
The regional healthcare agency guidelines recommended for this renovation not only a Class D around the isolator, but over to create a pressure difference between adjacent rooms with at least 10 Pa (0.00145 psi) pressure differential between the preparation room and the personnel access anteroom and 10 Pa between this anteroom and the surrounding administrative area (see Figure 1). As a reminder, GMP specify that these compliance targets only apply to CCPUs equipped with class II biosafety cabinets but could be extended to units equipped with isolators.
Centralized chemotherapy preparation unit (CCPU) and aeraulics plan.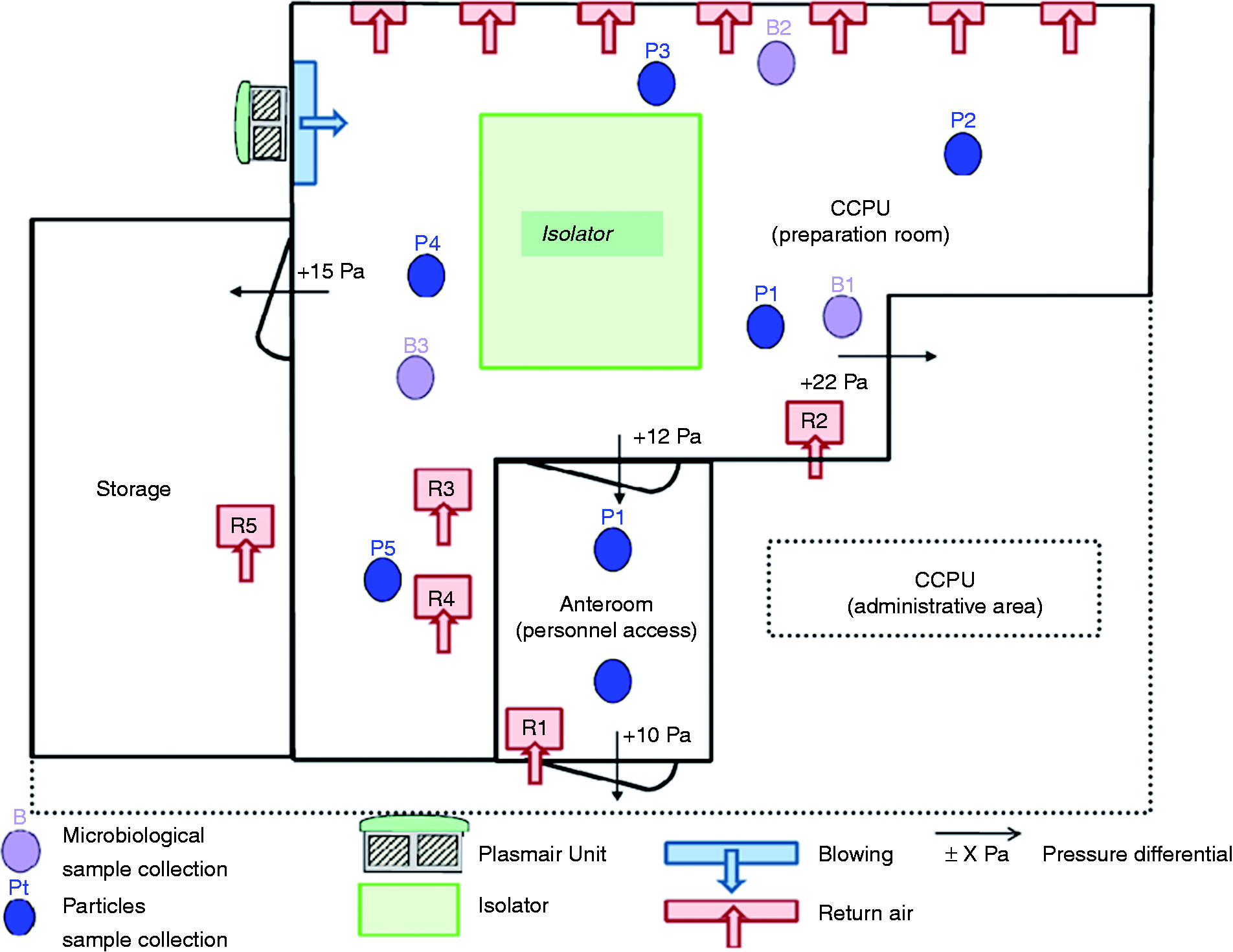
We have studied some technical and economical aspects to evaluate the feasibility of the MADU option. MADU should not only ensure a class D environment, but also generate a positive pressure by blowing, which involved a MADU placed outside the preparation room. The cost-effectiveness of this option as opposed to conventional AHU set-ups should be taken in count. Finally, efficiency of a MADU should be confirmed by an operational qualification of the CCPU and by air quality monitoring. Specifically, the hospital ordered a “qualification of the centralized chemotherapy production unit equipped with a Plasmair unit T2006”. Provision of services included these measurements: airborne particulate classification, air decontamination (particulate) kinetics in the anteroom, particulate and microbial contamination levels, air flow rates in the CCPU (intakes and returns), air change rates and pressure differentials.
Results
Technical aspects
Preliminary simulation studies carried out by Airinspace SE for the CCPU upgrade predicted that MADU Plasmair™ T2006 model installed in an adjacent area was able to supply sufficient airflow rate (2000 m3/h capacity) with regard to the room’s volume (preparation room: 117 m3) to be treated in terms of air quality and pressure differential targets (Figure 1). These projections took into account an airflow lowering due to an eventual lack of adequate seals at the room’s interfaces. MADU could be technically placed outside the preparation room with use of an adaptation ducting system to channel the airflow inward the CCPU (see Figure 1).
Economical aspects
The MADU option provisional cost was 23.600 USD (including value added tax) for purchase, set-up of the unit and operational qualification. In addition to that cost, 12.400 USD were necessary to enforce air tightness of the room with construction of two anterooms plus few adjustments (protective compartmentalization of the MADU outside the CCPU, air duct, diffusion grilles, and pressure sensors). Estimated total cost directly relating to the MADU option was 31.300 USD. Yearly preventive maintenance forecast was 1.800 USD.
As for the conventional AHU option, 70.000 USD were quoted for the specific configuration of our hospital’s CCPU including the AHU set-up and extension of the air duct network. Maintenance costs were not assessed for this option.
Although the AHU option’s cost was estimated and was not supported by actual construction work, the MADU option appeared cost-effective and beneficial.
Qualification
Operational qualification: results.
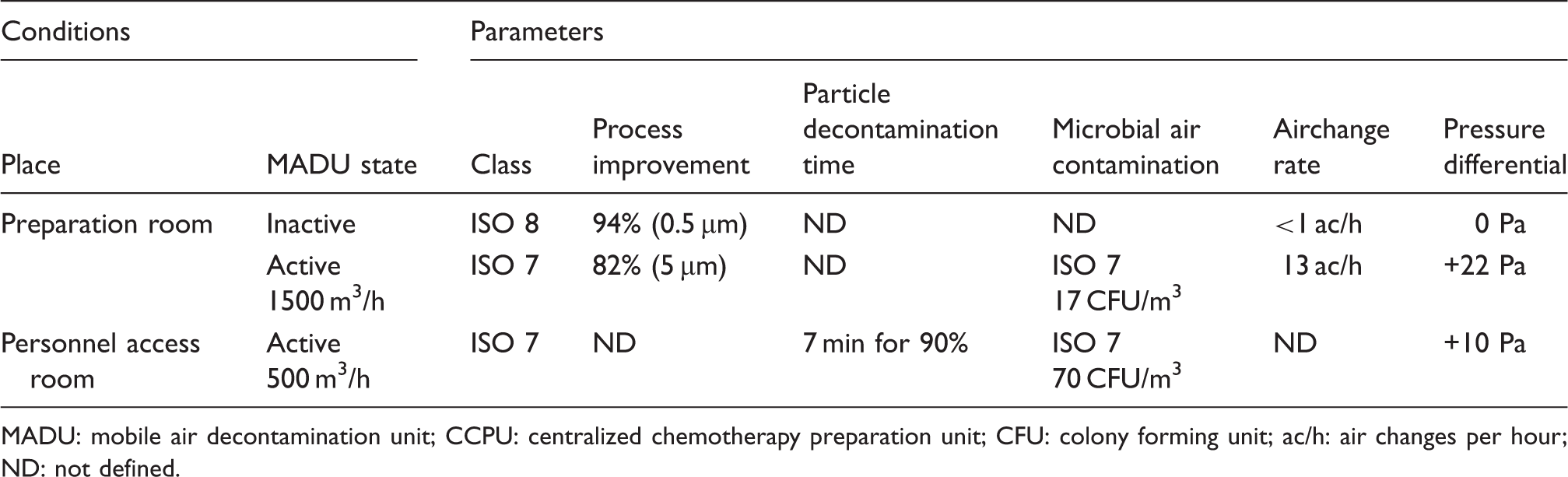
MADU: mobile air decontamination unit; CCPU: centralized chemotherapy preparation unit; CFU: colony forming unit; ac/h: air changes per hour; ND: not defined.
Airborne particulate classification was in the preparation room Class D with Plasmair® “Off” and Class C with Plasmair® “On”, Class C in the anteroom (personnel access room) with Plasmair® “on”. Air decontamination kinetics was realized in the anteroom: abatement of the airborne contamination by a factor of 10 was achieved within 7 min. Microbial air contamination measured by impaction was lower than 200 CFU/m3 (Class C) both in the preparation room and in the anteroom. Air flow rates were 1500 m3/h for intakes and between 2.2 and 3.8 m3/h for returns (see Figure 1). The number of air changes per hour was 13 ACH in the preparation room. Positive pressure differentials were 22 Pa (0.00319 psi) between preparation room and administrative area, 12 Pa (0.00174 psi) between preparation room and anteroom, 15 Pa (0.00218 psi) between preparation room and storage room, 10 Pa (0.00145 psi) between anteroom and administrative area.
Discussion
Impacts of the works
The MADU option presented the advantages of keeping to a minimum construction work that could have impacted the air quality as it was mostly carried out outside the area. Construction was planned over three non-consecutive half-days. Chemotherapy activities were dispatched between adjacent days in accordance with the medical staff in order to prevent any significant impact on the patients’ care. According to the internal procedures of the CCPU, reconstitution activity using a fully closed-system device (Tevadaptor®, BBraun laboratories) was temporarily considered as a precautionary measure for the construction duration in the event that some patients would have not be planned outside the works period. A closed-system device minimizes the risk of contamination during the drug reconstitution step. Indeed, in this system, specific devices are previously connected to vials, syringes and infusion bags to limit the contact between air and hazardous drug.
Qualification
Operational qualification carried out after the construction phase demonstrated full compliance of the system to particulate, microbial and pressure differential performance targets for each distinct area8–11 (Figure 1, Table 1). Particulate and microbial contamination levels were significantly improved. Indeed, class C (ISO 7) had been obtained, whereas class D (ISO 8) was initially required. Particle decontamination time obtained was 7 min, whereas 20 min was sufficient according to guidelines. 8 Thirteen air changes per hour contribute to the pressure differential and to the air decontamination kinetics.
Subsequent adjustments
Minor adjustments were made upon installation with the MADU. Notably, air vent returns and supplies were redesigned to reduce the inlet airflow from 1200 to 1050 m3/h with a pressure differential unchanged. Air quality was re-tested after this adjustment by the independent laboratory (APTE) to ensure that the benefit was still maintained in terms of microbial and particle decontamination and in terms of pressure differential. This airflow decrease has reduced residual airspeeds originally felt as disturbing by the unit’s staff.
Balance after one year
The MADU performances complies with initial expectations overall. Air quality controls carried out by an independent institution confirm the efficacy of the process. However, we were surprised by an additional cost of 1.200 USD per year in the maintenance budget due to a significantly reduced lifetime of the filters (this inconvenience does not affect significantly the choice of the MADU option). Indeed, replacement frequency of the pre-filter stage had to be increased fourfold with regard to the standard yearly replacement included in the maintenance plan. In the future, we cannot exclude that other filters could also be altered eventually and the lifetime of the filters hence requiring rigorous maintenance. In fact, we can explain this excessive clogging of the filter elements by the operating mode. In our case, to ensure a positive pressure in the preparation room according to French guidelines, MADU is placed outside this room and continually runs with non-purified air, whereas MADU are usually placed in the room to treat with air progressively purified (recycled air).
Limitations
Although implementing the MADU was finally technically easy in terms of works, this project initially required a significant expertise. Indeed, technological and economical feasibility were dependent on CCPU’s specific environment. In our own case, according to the management board of the hospital, this estimation was in favour of the MADU option. Even though solely major parameters have been taken into account, other parameters could be considered as negligible to influence the choice of the less costly option. However, costs for implementing a conventional AHU depends of each CCPU.
According to French GMP and French authorities, our compounding room is in a positive pressure environment. GMP specifies that rules about work areas for the sterile drugs must also be applied for sterile hazardous drugs. Protection of products, staff and environment must be ensured by a quality system policy. A sterility of products with no dissemination must be ensured. In addition, French GMP recommends that CCPU is negatively pressured compared to external environment in order to block a potential hazardous particle spread (principle of isolation). To ensure a positive pressure in the compounding room and a negative pressure around the CCPU requires an additional space, which is possible solely for a new CCPU construction, not for a renovation purpose. Finally, using a MADU is well adapted for upgrading the area to air quality compliance in a preparation room in a context of renovation but does not meet this principle of isolation, contrary to a new building.
In other countries, if a negative pressure in the preparation room is acceptable, MADU could be favorably placed also in this room in a recycling mode. Not only this would limit clogging of the filter elements, but also this could have a beneficial effect on potential chemical contaminants because of the technology “cold plasma” used in Plasmair® system. The impact of this chemical decontamination action could be qualitatively and quantitatively explored.
Conclusion
Based on our experience, the MADU option is economically and technologically beneficial when compared to conventional AHU implementation in a CCPU equipped with an isolator for upgrading the area to air quality compliance in terms of microbial and particle burden. The unit allows supply of fresh decontaminated air even under unfavorable conditions.
Implementing a MADU requires initially a significant expertise but is technically easy in the works step with minor impact on the chemotherapy drugs preparation activity during set-up. For these reasons, MADU option is interesting in a context of renovation.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.