
Abstract
Ipilimumab, monoclonal antibody against cytotoxic T-lymphocyte antigen-4 and, radiotherapy are commonly used to treat unresectable and metastatic melanoma. As a result of upregulation of immune system with ipilimumab, many immune-related adverse effects, such as dermatitis, colitis, hepatitis, and hypophysitis, have been previously reported in literature. Typically, these effects are treated with high-dose steroids and mostly heal up. Here, we report a case who was receiving radiotherapy due to metastatic malignant melanoma with atypical generalized rash, which was enlarged with concurrent ipilimumab treatment.
Introduction
Ipilimumab has increased the median overall survival in patients with unresectable and metastatic malignant melanoma and it was approved by U.S. Food and Drug Administration in 2011. 1 Ipilimumab is a monoclonal antibody to cytotoxic T-lymphocyte antigen-4 (CTLA-4) that increases the immune response to tumor by increasing T cell activation and proliferation. 2 Activation of T cells causes the immune-related adverse events (irAEs) such as dermatitis, enterocolitis, hepatitis, and hypophisitis. The most commonly seen dermatological adverse events are rash, pruritus, vitiligo, and alopecia. Stevens–Johnson syndrome, toxic epidermal necrolysis, full-thickness dermal ulceration are rare adverse events. 3
The application of ipilimumab and radiotherapy together in malignant melanoma patients increases the immune response.4,5 Radiation dermatitis is a potential adverse effect of external beam radiotherapy. Risk of clinical radiation injury is dependent on dosage and location. Typically it appears two to three weeks after the start of radiotherapy. Generally, most of the acute radiation dermatitis resolves spontaneously in two to three weeks after the apperance. 6
Here, we report a case who was receiving radiotherapy due to metastatic malignant melanoma with atypical generalized rash that was enlarged with concurrent ipilimumab treatment.
Case
A 53-year-old previously healthy woman was admitted with right axillary mass in November 2012. Mammography and, breast and, axillary ultrasonography revealed right axillary 60 × 41 mm fixed solid mass. The histopathological and immunhistochemical analysis of tru-cut biopsy revealed malignant melanoma metastases. In (18) F-fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT), there were no primary or metastatic area except right axillary hypermetabolic mass (Standard Uptake Value (SUV) max: 24.40). Dermatological examination was normal. In addition to the excision of mass, right axillary lymph node dissections were performed in December 2012.
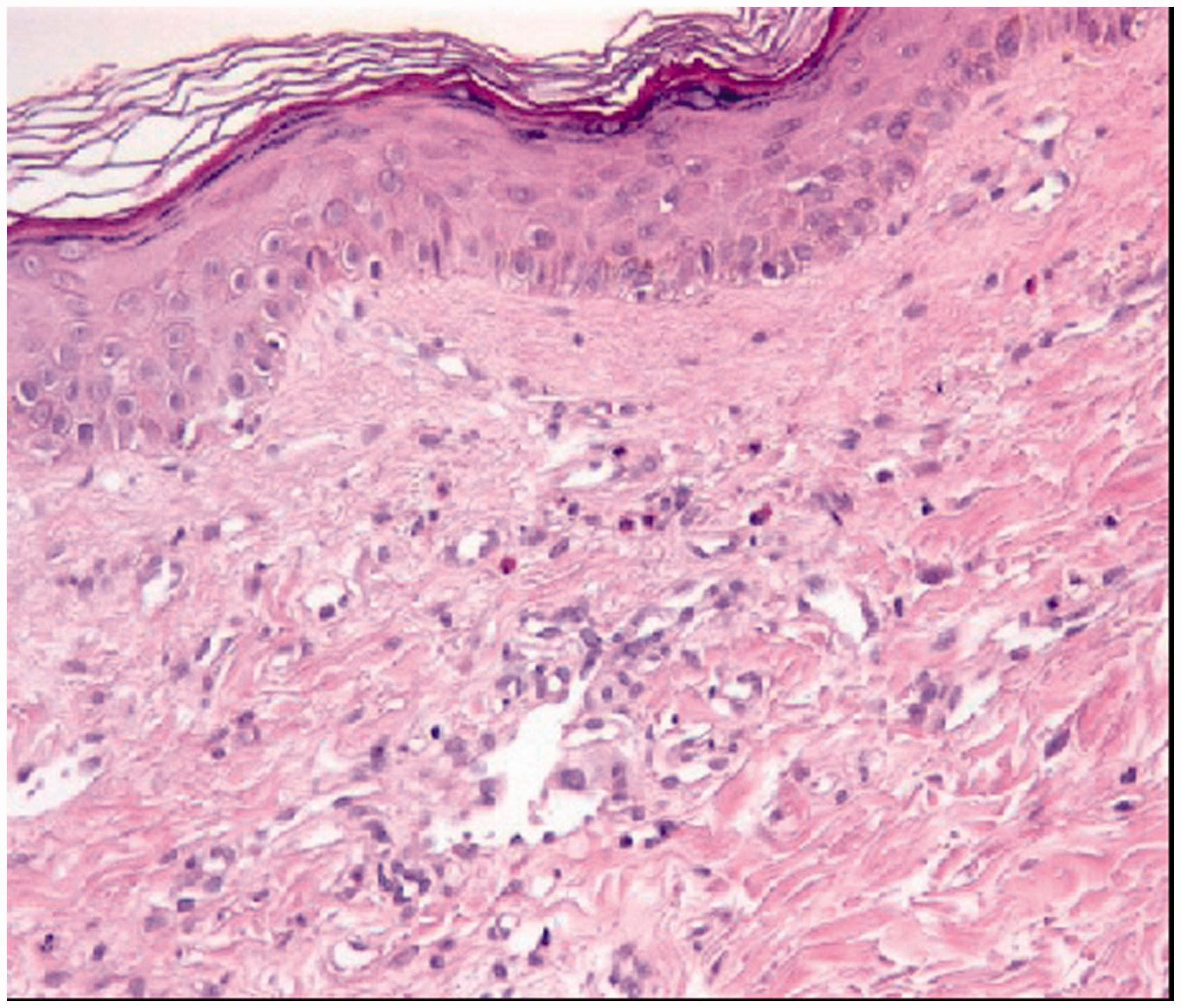
In January 2013, adjuvant high-dose interferon-alpha (IFN-α) induction therapy (20 million units (MIU)/m2, five days/week for four weeks intravenous infusion, maintenance treatment; 10 MIU/m2, sc (subcutan), three days a week) was started. During the 10th month of IFN-alpha therapy, local relapse was proven by biopsy. IFN-alpha was stopped and Vemurafenib 960 mg/day treatment was started in this patient who was BRAF V600E mutation-positive. During the fourth month of Vemurafenib therapy, PET-CT showed progression in right axillary region, subcutaneous soft tissue, and bone. Vemurafenib was interrupted and ipilimumab (3 mg/kg/three weeks) was started. After the second cycle, palliative radiotherapy (RT) to right axillary mass was started. After four days from starting of RT, generalized hyperemia, palpable rashes separated by sharp boundaries appeared on involved and noninvolved areas especially axillary, chest, and dorsal regions (Figure 1). Radiotherapy was completed in 10 days. Total 3000 cGy radiation therapy was given with Intensity-Modulated Radiation Therapy (IMRT) technique. Rash was nonitchy. The patient did not experience fever, eosinophilia in peripheral blood. Patient did not use any medications other than fentanyl and proton pump inhibitors. Because of the involvement of outer of radiation field, in order to investigate the possible causes such as radiodermatitis and drug reaction related to ipilimumab, skin biopsy was performed. Biopsy revealed perivascular eosinophilic mononuclear inflammatory cell infiltration in the dermis with melanin pigment increase in the basal layer (Figure 2). Microscopic features were not compatible with radiodermatitis. Maculopapular rash due to ipilimumab was diagnosed and, 1 mg/kg oral methylprednisolone was started. The patient responded dramatically to corticosteroid therapy and lesions were significantly reduced on day 3 (Figure 3).
At the time of treatment with radiotherapy concurrent ipilimumab. Pathologic imaging. After steroid treatment.

Discussion
CTLA-4 is expressed on the surface of both cluster of differentiation (CD) 4+ and CD8 + T cells. T cell activation is controlled by positive and negative signals. CTLA-4 is co-receptor inhibitor, and has very low basal expression; the expression increases following T cell activation and is responsible for limiting immune response. 7 Blockage of CTLA-4 with ipilimumab enhances antitumor immune response. In patients with unresectable or metastatic melanoma, ipilimumab is administered 3 mg/kg/three weeks for four cycles and this treatment may cause autoimmune-like adverse effects in patients receiving it. The most frequent associated adverse events are immune dermatitis, hepatitis, colitis, hypophysitis, and uveitis.8,9 The frequency of irAEs is dose dependent. 10
The ipilimumab-related skin lesions usually consist of discrete, erythematous, pruritic, minimally scaly papules that are generally localized to the trunk and extremities. The palms and soles are usually spared off, face and head involvement are rarely seen. Maculopapular rash is seen in 47–68% of patients receiving ipilimumab. The rash usually occurs early in the course of treatment with ipilimumab, in the first three to four weeks; also it can occur earlier or after completion of therapy. The rash may worsen after each ipilimumab dose. A significant increase in peripheral eosinophilia has been observed in patients who develop rash. 11 Histologically, a superficial, perivascular CD4+ predominant T-cell infiltrate with eosinophilic infiltration in the papillary dermis, rare dyskeratotic cells, and mild epidermal spongiosis may be present. These events likely represent a skin-targeted T-cell activation as a result of CTLA-4 inhibition. The rash is usually well tolerated and self-limited, which resolves within two to three months. Treatment consists of topical corticosteroids or urea-containing creams and antihistamines for the morbilliform eruption. 12 Grade-3 rashes can be treated by withholding a scheduled dose of ipilimumab and by initiation of oral corticosteroids starting at a dose of 1 mg/kg prednisone once daily. Grade-4 skin toxicity is very rare but toxic epidermal necrolysis and Stevens–Johnson syndrome have been reported. 13 In such cases, oral corticosteroids such as prednisolone, should be promptly initiated at a dose of 1–2 mg/kg with a slow taper. Furthermore, ipilimumab should be permanently discontinued. Radiotherapy remains an interesting treatment modality for patients with metastatic melanoma. The value of adjuvant radiotherapy following lymph node dissection has long remained uncertain. Recent studies showed that adjuvant radiotherapy following nodal dissection in patients with locally advanced melanoma is associated with improved regional disease control; however, survival benefit has not yet been proven.14,15
The disease has been shown to regress in the regions except from irradiated locations in malignant melanoma patients treated with irradiation. Thus, radiotherapy in melanoma patients to modulate the immune system is supported.16,17 It is observed that ipilimumab used together with radiation therapy enhances the immune response. Synergy between radiation and the immune system is seen in experimental models.18,19 Recently, ipilimumab and radiotherapy treatment is described as having strengthened antimelanoma immunity in a few patients, which coincided with tumor regression.4,20 Based on these findings, radiotherapy has great potential in inducing antitumor immunity. However, when immunotherapy such as IFN and radiotherapy is used in combination, radiation-induced skin adverse effects are reported at higher rates in previous studies.21,22
In a retrospective study performed in Memorial Sloan–Kettering Cancer Center, 29 patients who underwent 33 courses of nonbrain radiotherapy between their first and last dose of ipilimumab were analyzed. The median doses of ipilimumab and radiotherapy in this study were 10 mg/kg and 30 Gy. Ninety-eight days after administration of ipilimumab at a dose of 3 mg/kg and 64 days after receiving radiotherapy, grade 3 maculopapular rashes were formed in a patient. The frequency of irAEs was not significantly different compared with previous studies of ipilimumab alone. In this study, radiation therapy did not appear to compromise the efficacy of ipilimumab. 23 During the second and third administration of ipilimumab, the patient presented in this report received nonbrain radiotherapy. Grade 3 rash was formed both in and outside of radiotherapy field 10 days after administration of ipilimumab and four days after the onset of radiotherapy.
As a result, this is the first report proving the increase in skin toxicity secondary to radiotherapy when ipilimumab is used in combination with radiotherapy. Therefore, these patients may be followed closely during therapy. In addition, further research and reports will be necessary to determine whether combining radiotherapy and immunotherapy is associated with AEs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.