
Abstract
Shortage of oncology drugs is a particularly complicated issue because there are usually limited therapeutic options. Moreover, oncology practice may employ medications for supportive indications which differ from their main usage. This means shortage of oncology drugs is not usually addressed by the major drug shortage guidelines. We have previously shown that, during a shortage crisis, it is possible to make a recommendation on the use of an expired drug supply based on a reasonable estimate of its safety and efficacy. Here, we would like to share further examples on how to deduce potential therapeutic alternatives based on pharmacokinetic and pharmacodynamic principles in the absence of direct clinical evidence in the literature.
Drug shortage is an emerging issue in oncology practice.1–7 Shortage of oncology drugs is particularly complicated because there are usually limited therapeutic options. Most practice guidelines do not advise on alternatives that may be considered during a supply shortage. Moreover, oncology practice may employ medications for supportive indications which differ from their main usage. This makes it challenging when developing therapeutic alternatives for these indications.
We have previously shown that, during a shortage crisis, it is possible to make a recommendation on the use of an expired supply of alemtuzumab based on a reasonable estimate of its safety and efficacy. 8 Here, we would like to share further examples on how to deduce potential therapeutic alternatives based on pharmacokinetic and pharmacodynamic principles in the absence of direct clinical evidence in the literature.
Shortage of intravenous ranitidine
Paclitaxel (TAXOL®) is a taxane chemotherapy agent widely used for the treatment of breast and ovarian cancers. Histamine type 2 (H2) antagonists such as ranitidine are an integral part of the pre-medication regimen in minimizing hypersensitivity reactions associated with paclitaxel. 9 Standard pre-medication regimens consist of ranitidine 50 mg and diphenhydramine 50 mg given intravenously 30 to 60 min before paclitaxel, plus oral dexamethasone administered 12 and 6 h before paclitaxel.
A Canadian shortage of intravenous ranitidine emerged in May 2012. Famotidine was chosen as an alternative because it is the only other intravenous H2-antagonist available in Canada and it has a similar profile in terms of toxicity and drug interactions. Also, it has been used successfully to prevent paclitaxel-related hypersensitivity reactions in patients with gynecological malignancies10,11 and is included as a treatment option for general drug reactions. 12 However, the sudden increase in demand for intravenous famotidine led to a subsequent shortage of this product. Since omission of H2-antagonist may expose the patient to potentially significant paclitaxel-related toxicity, there was a need for further alternatives.
Oral ranitidine was an obvious candidate but there had been no published literature (Medline, Embase) or in-house data from the manufacturer (Bristol Myers Squibb) on its use to prevent paclitaxel-related hypersensitivity reactions. However, this did not mean that there was no evidence to support a recommendation on the use of oral, in place of intravenous, ranitidine. Given that the prophylactic regimen consists of three drugs with different mechanisms of actions, slight dosing modification of one agent would probably have limited effects on the overall efficacy of the regimen.
The therapeutic level for anti-histaminic effect is unknown. However, the serum AUC with an intravenous dose of 50 mg was reported to be 1.22 mg/L/h.
13
Based on reported pharmacokinetic parameters,
13
the serum concentration at 30 min after dose administration can be calculated to be about 460 ng/mL:

A comparable serum concentration (440 ng/mL) 14 and AUC (1.88 mg/L/h) 13 can be achieved at 2 h after an oral dose of 150 mg. Therefore, such an oral regimen can be expected to be as effective as an intravenous regimen in preventing paclitaxel reactions.
Since patients were used to receive their intravenous ranitidine at the clinic, it was anticipated that some patients might forget to take their oral ranitidine before arriving for their paclitaxel therapy. If these patients take their oral ranitidine at the clinic just before paclitaxel, their serum concentration would likely be low since it takes about 2 h to reach the peak concentration after an oral dose. For example, by extrapolating the graphical results from a pharmacokinetics study, 13 the serum concentration is estimated to be only 236 ng/mL at 1 h after an oral dose of 150 mg.
One solution is to increase the dose to 300 mg which would lead to an estimated serum concentration of 472 ng/mL after 1 h. This serum level would be comparable to that seen with intravenous 50 mg after 30 min or oral 150 mg after 2 h. Since this higher dose is already used and well tolerated for gastric ulcer management, 14 it is reasonable to recommend oral ranitidine 300 mg to be given about 1 h before paclitaxel, for patients who have forgotten to take their ranitidine before arriving at the clinic.
Based on these pharmacokinetic principles, patients receiving paclitaxel at the BC Cancer Agency centres across the province were recommended to take oral ranitidine 150 mg 2 h prior to paclitaxel administration, or 300 mg 1 h prior if they had neglected to take the dose before arriving at the clinic. This recommendation was implemented for the duration of the intravenous ranitidine drug shortage which lasted for 5 months. A retrospective study of outcomes from this recommendation has not been done. This is mainly because there was no easy documentation database to accurately identify the incidence of hypersensitivity reaction with paclitaxel. In addition, the incidence would be so low that there would not be enough patients treated with oral ranitidine to perform a proper comparison with sufficient power.
Shortage of intramuscular vitamin B12 (cyanocobalamin)
Pemetrexed (ALIMTA®) is an antifolate chemotherapy agent commonly used for the treatment of non-small cell lung cancer and malignant mesothelioma. It is associated with significant myelosuppression which can be countered with supplementation of vitamin B12 and folic acid. With routine supplementation, the incidence of grades 3 and 4 febrile neutropenia can be reduced from 9% to 1% without compromising the effectiveness of pemetrexed. 15 Standard vitamin B12 supplementation consists of 1000 mcg intramuscular injection every nine weeks, starting one week before pemetrexed therapy and continuing until three weeks after the last pemetrexed dose.
A Canadian shortage of vitamin B12 intramuscular injectable emerged in October 2013. Oral vitamin B12 was considered as an alternative because it is often used for the treatment of vitamin B12 deficiency. However, the ALIMTA® monograph states that intramuscular vitamin B12 should not be substituted with an oral formulation. 15 The manufacturer (Eli Lilly) does not specify the exact reason for this, except that oral formulation has not been studied for this indication. In addition, we also did not identify any published literature (Medline, Embase) or in-house data from the manufacturer on the use of oral vitamin B12 to prevent pemetrexed-related toxicity. Nevertheless, there are few options for patients who need pemetrexed therapy while avoiding a high incidence of toxicities, particularly with malignant mesothelioma. Therefore, these patients would require an alternative to intramuscular vitamin B12 to prevent pemetrexed-related toxicity.
The serum vitamin B12 concentration associated with preventing pemetrexed toxicities is unknown.16–18 Also, the serum vitamin B12 concentration associated with standard supplementation (1000 mcg intramuscularly every 9 weeks) has not been reported.16–18 Clinical studies have used the reverse surrogate markers for vitamin B12 and folate deficiency, such that pemetrexed toxicities are associated with elevated levels of total plasma homocysteine and methylmalonic acid. 17 Patients were more likely to experience severe toxicity with a baseline homocysteine level > 11.5 µmol/L (odds ratio of 3.1) compared to patients with normal baseline level. Similarly, patients with methylmalonic acid > 119 nanomol/L also experienced more toxicity compared to those within the reference range of 119.0–219.3 nanomol/L (odds ratio of 3.3). Toxicities are minimized when patients are supplemented with the standard intramuscular vitamin B12 regimen, 19 with homocysteine level declining from a mean baseline of 8.3 µmol/L to 6.9 µmol/L after the first three cycles of pemetrexed therapy. 16 Therefore, an oral vitamin B12 regimen can be expected to be as effective if it can achieve a similar reduction in homocysteine levels.
There are numerous randomized comparisons of intramuscular vs. oral vitamin B12 for the management of vitamin B12 deficiency,2–8 but not in the prevention of pemetrexed toxicities. After one month of therapy, none of these regimens are associated with the 6.9 µmol/L homocysteine level associated with reduction in toxicities. Also, the serum levels of homocysteine20–24 and vitamin B1220–26 seems to change non-linearly with the vitamin B12 doses, probably depending on the extent of baseline deficiency. Finally, the recommended intramuscular regimen for pemetrexed toxicities has an unusual dosing schedule (every nine weeks), which makes direct conversion to an oral dose challenging.
Therefore, there is no simple way to estimate an equivalent oral to intramuscular dose of vitamin B12 in the prevention of pemetrexed toxicities. Since pemetrexed toxicities are related to temporary vitamin B12 insufficiency, any effective oral dosing for vitamin B12 deficiency should be adequate in minimizing pemetrexed toxicities. Since the clinical effect of pemetrexed depends on its antifolate activity, excessive vitamin B12 may theoretically negate the cytotoxic activity of pemetrexed. Hence, the lowest oral effective dose for vitamin B12 deficiency (250 mcg/day) 27 was chosen. To be prudent, patients supplemented with oral vitamin B12 were monitored more closely for myelosuppression. Post-implementation data were not formally collected, but informal feedback from oncologists who prescribe pemetrexed and who had patients on oral vitamin B12 during the shortage suggests that this was as well tolerated and an effective option.
Discussion
Evidence-based practice has been the accepted standard in drug therapeutics over the past two decades. 28 Until recently, we have been fortunate to be able to make most therapeutic decisions based on at least some direct clinical evidence (e.g. phase II studies, case reports). However, frequent drug shortages in the recent years have presented us with the challenge of identifying acceptable therapeutic alternatives in the absence of such evidence.
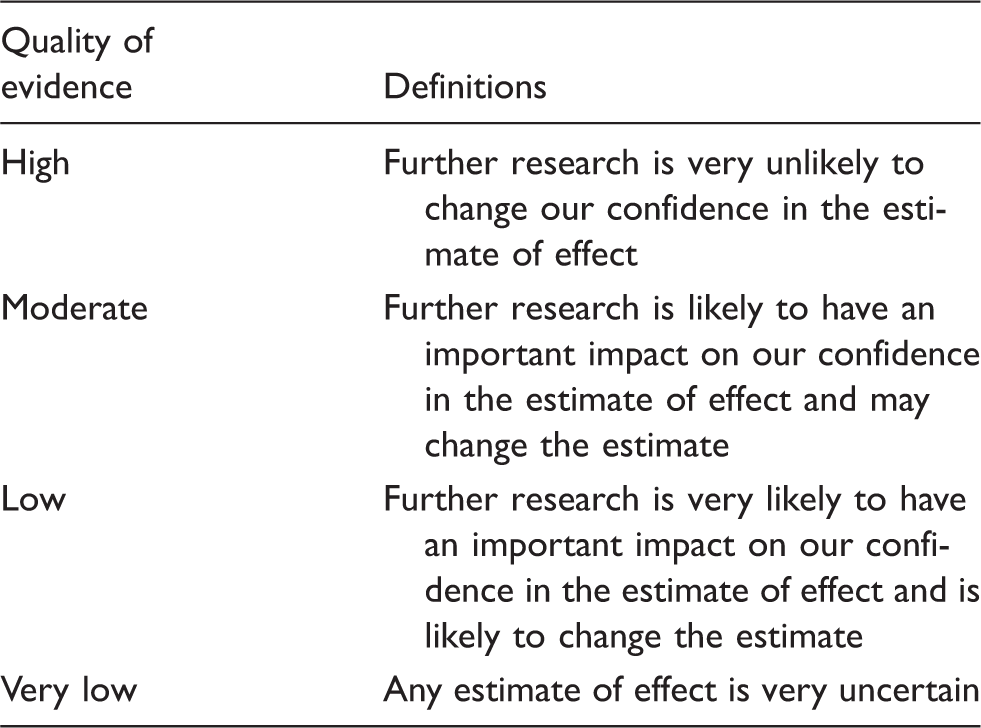
Quality of evidence and definitions.
Randomized clinical studies are still the gold standard, and when drug shortages resolve, our practice is to revert to standard options as soon as they become available on the market. An interesting area of controversy is whether or not continued use of oral ranitidine and oral vitamin B12 is acceptable when parenteral products are now available. One may argue that because of the lack of any reported clinical outcome data, it is not possible to accurately assess the effectiveness of these therapeutic options. However, it should be noted that approval of generic drugs is routinely based on bioequivalence through pharmacokinetic data, usually without further clinical studies to establish effectiveness.31–33
In summary, the lack of direct clinical evidence in the literature does not mean that a recommendation cannot be made when addressing essential drug shortages. Nor does it mean that we would need to rely solely on subjective, individual experience. The conscientious, explicit, and judicious use of the next best external evidence 29 can still support high-quality decision-making.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.