
Abstract
Background
The traditional model of community pharmacy has changed, with patients, caregivers and consumers having access to many cognitive services other than the traditional dispensing and supply of medicines. In December 2009, a population-based colorectal cancer screening program started in Barcelona, introducing the community pharmacist and the professional expertise of the pharmacist into the organisational model.
Aim
To evaluate the program implementation process in the pharmacies, identify barriers and facilitators, and know the opinion of the professionals involved in the colorectal cancer screening program in Catalonia (Spain).
Methods
Cross-sectional study of the pharmacies that participated in the first round of the program during the first and second trimester of 2010 in Barcelona. A validated questionnaire was used to analyse several functional aspects in the implementation process. Qualitative aspects about the opinion of the pharmacist were studied. A descriptive and bivariate analysis was performed.
Results
All the pharmacies involved in the program (n = 74) participated in the study. The majority of the sample population was composed of women (70.3%), mean age 44.9 years, and most of them (74%) had attended a specific training session. Pharmacists considered their participation in the program to be an added value to their professional role and a way to increase consumer’s confidence on this kind of services. The average time to provide the service was estimated to be less than 10 minutes per consumer. Only three (4.1%) pharmacists considered that the program involved a lot of extra work in the daily activities of the pharmacy. The level of satisfaction of the pharmacists was very high.
Conclusions
Community pharmacies can be a successful alternative and great resource to implement a population cancer screening program. This functional model can improve the accessibility and participation rates on target population. The level of motivation of the community pharmacist, the specific training program and the perception to give a better care for their patients can be an enabler.
Introduction
The traditional model of community pharmacy has changed in the recent years. New health policies focused on solving health problems in proximity centres, and achieving more effectiveness and efficiency to provide health services have led to new visions and models in the European Union, United States, Canada, Australia and New Zealand.1–5 These new models imply that patients, caregivers and consumers have now access to many cognitive services in the community pharmacy, besides the traditional dispensing and supply of medicines. Recently, the Royal Pharmaceutical Society 6 urged the different levels of care and health workers to work with pharmacists and use their professional expertise in health promotion and disease prevention activities.
Significant accessibility (high presence in urban areas, proximity, and long opening hours), territorial balance and the level of confidence of the population allow pharmacists to work more closely with patients and consumers. Community pharmacies can have a key role in population-based screening programs or in those targeting populations with risk behaviors and/or profiles. 7 However, the implementation of expanded roles has been slow. 8
Colorectal cancer is the third most incident cancer in male and the second in women worldwide, and it represents the fifth cause of cancer-related death. 9 Randomised trials have shown the efficacy of screening to detect colorectal cancer in early stages and to reduce mortality. Based on this evidence, European Union recommended to its member states the implementation of colorectal cancer screening programs using faecal occult blood test among women and men from 50 to 74 years of age. 10
In December 2009, the Colorectal Cancer Early Detection Screening Program (PDPCCR) was launched in Barcelona (Catalonia, Spain). It is a population-based program based on biennial fecal immunochemical testing (FIT) with colonoscopy for positive cases. The PDPCCR included the community pharmacist into the organisational model, in a voluntary basis. 11
In order to evaluate the program implementation process in the pharmacies, know the opinion and satisfaction of the professionals involved in program development and identify barriers and facilitators, we conducted a survey among pharmacies involved in the program.
Material and methods
A cross-sectional, descriptive study of the first 74 pharmacies that participated in the first round of PDPCCR during the first and second trimester of 2010 was conducted in Barcelona. The target population to be included in the PDPCCR during the study period was 47,224 people.
Screening program operation and pharmacies involvement
The PDPCCR targets all men and women from 50 to 69 years of age in Barcelona. The FIT, performed biennially, is distributed and collected through community pharmacies.
An invitation letter accompanied with an informative leaflet about the PPDCCR and a list of the nearest pharmacies participating in the program was sent to the target population. The role of the pharmacist was to advise, motivate and explain potential participants how to perform the test properly. At the same time, they performed a triage activity to detect subjects at high risk (with previous colon or rectum cancer, polyps, inflammatory bowel disease or a family history of colon and rectum cancer) who should be excluded of the program. Pharmacists provided the FIT to participants and reminded them to return it in a term of 15 days and, at most, 3 days after the sample collection. When the participants returned the FIT, pharmacists checked that it was returned in the specified period, collected it and sent it to the reference laboratory. An electronic online software was specifically designed to ensure the traceability of samples collected to the central laboratory. 11 At least one pharmacists of each pharmacy was trained to do these tasks in a standardized live briefing lasting 2 hours, where they were also provided with all the specific material of the PDPCCR (FITs, posters, leaflets, identifying stickers, schemes and a guide for professionals, etc.).
Survey
Data about pharmacists (age, sex, professional category, attendance to briefing) and pharmacies (basic health area they belonged to, number of workers, opening hours, number of pharmacists that attended the briefing and/or took part in the program) were collected. Only one pharmacist from each pharmacy, fulfilling the inclusion criteria (being a graduate in Pharmacy, and had participated in the PDPCCR), could participate in the study.
A questionnaire was developed by members of the PROCOLON Research Group for the purpose of determining the different procedural aspects of the implementation of the PDPCCR in the pharmacies, as well as the opinion and assessment of the pharmacists. The questionnaire consisted of 26 questions with a Likert or categorical-type response of five options (see supplementary file), dealing with the following aspects:
– Attitude of the professionals in taking part in health promotion programs. – Workload and level of distortion caused by their participation in the PDPCCR. – Detection of barriers for the implementation of the PDPCCR in pharmacies, particularly logistic and communicative aspects between healthcare levels. – Quality and suitability of the briefing and the materials received to carry out the program. – Level of satisfaction with the program, willingness to continue participating in it and identification of the possible motivating elements.
A pilot test of the questionnaire was carried out on a sample of 10 professionals in order to evaluate its reliability, internal consistency, logical sequence and legibility of the questionnaire.
The Official College of Pharmacists of Barcelona provided data on pharmacies under a commitment of confidentiality and agreed with its Legal Advisor based on the Data Protection Law.
Statistical analysis
Mean and standard deviation were used to describe quantitative variables and valid percentages for the qualitative ones.
Variables corresponding to the Likert’s-type items in the questionnaire were re-categorised: the two positive responses were grouped on a category, and the two negative ones on another, avoiding the intermediate option, which included responses like “Not evaluable”, “I am not sure” and “Indifferent”. The association between qualitative variables was analysed using the Chi-square or Fisher exact test. Appropriate Student’s t test and Pearson correlation were used for the quantitative variables. A p value < 0.05 was considered to be statistically significant.
All the analyses were performed using the program SPSS v18.
Results
Characteristics of the study population (N = 74).
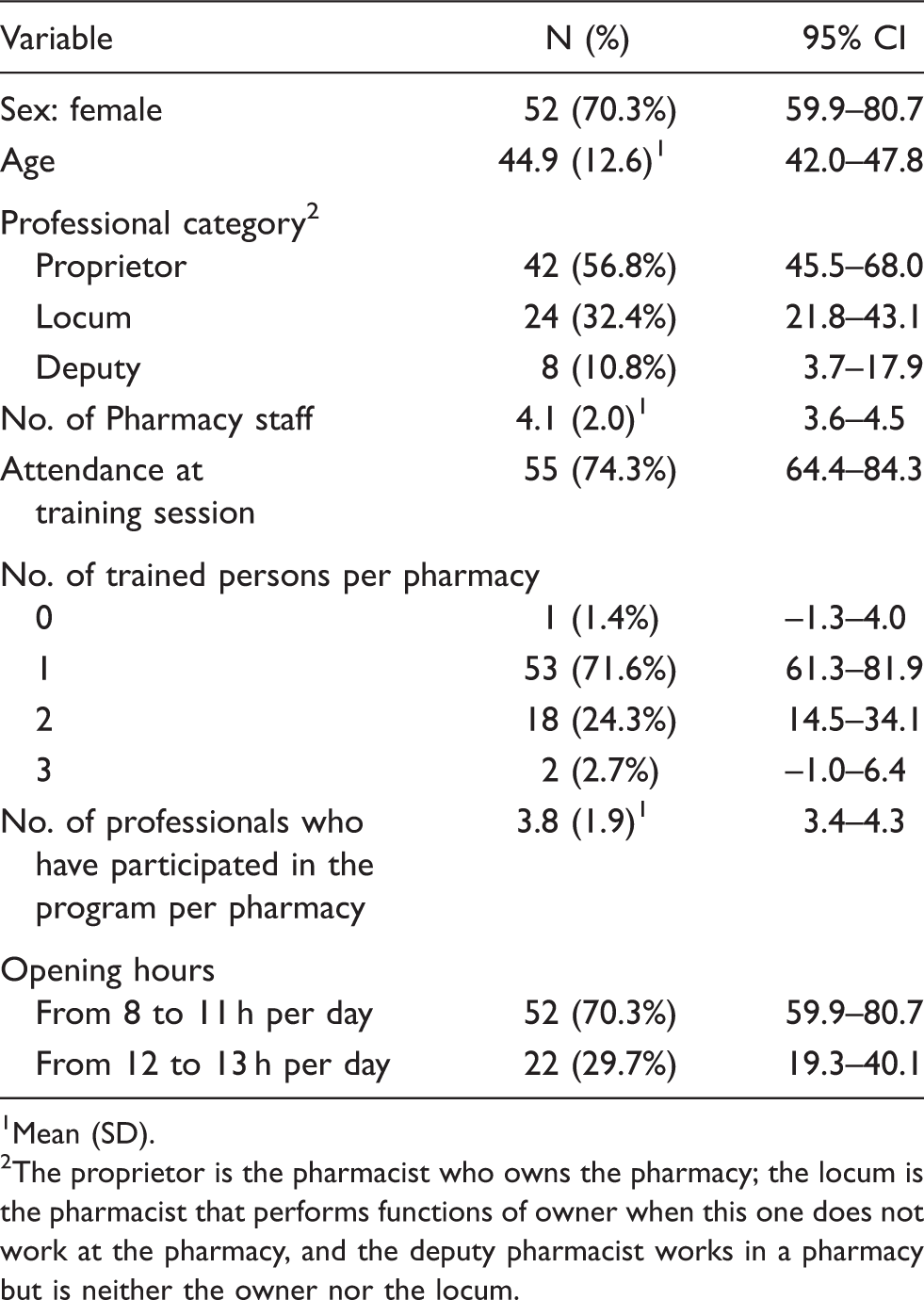
Mean (SD).
The proprietor is the pharmacist who owns the pharmacy; the locum is the pharmacist that performs functions of owner when this one does not work at the pharmacy, and the deputy pharmacist works in a pharmacy but is neither the owner nor the locum.
Almost all the respondents think that the participation of pharmacists in the PPDCCR is important or very important and that it adds value to their professional practice. Seventy-eight per cent considered that it had increased the positive perception of the users on the role of pharmacies and pharmacists.
Bivariate analysis of the factors associated to the level of effort involved in participating in the PDPCCR.
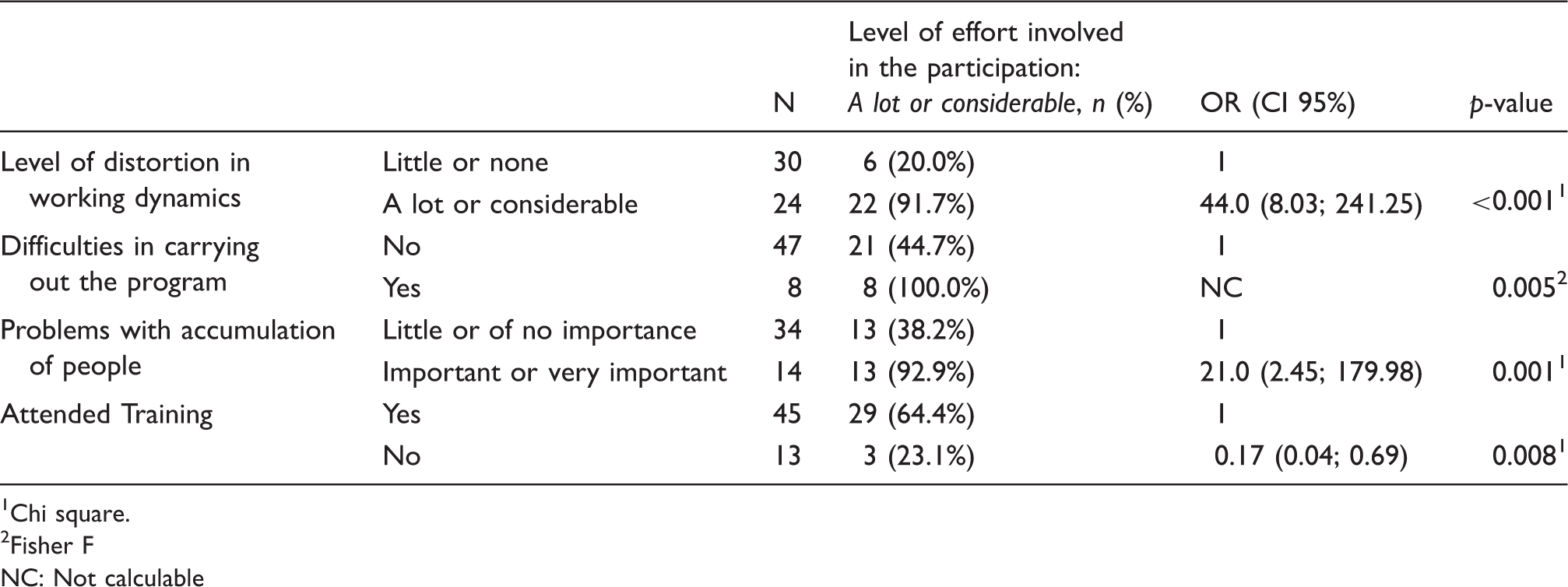
Chi square.
Fisher F
NC: Not calculable
Bivariate analysis of factors associated with the fact of assigning a specific person to the PDPCCR.
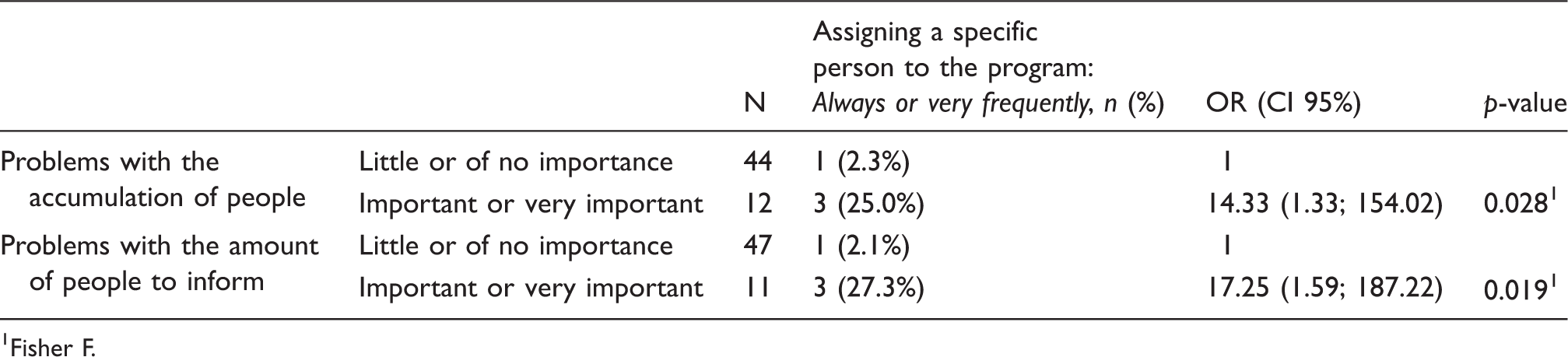
Fisher F.
The pharmacists, in more than 90% of cases, considered that the specific briefing program and the supplementary materials were great resources to develop their role.
Bivariate analysis of the factors associated with the level of satisfaction of having participated in the PDPCCR.
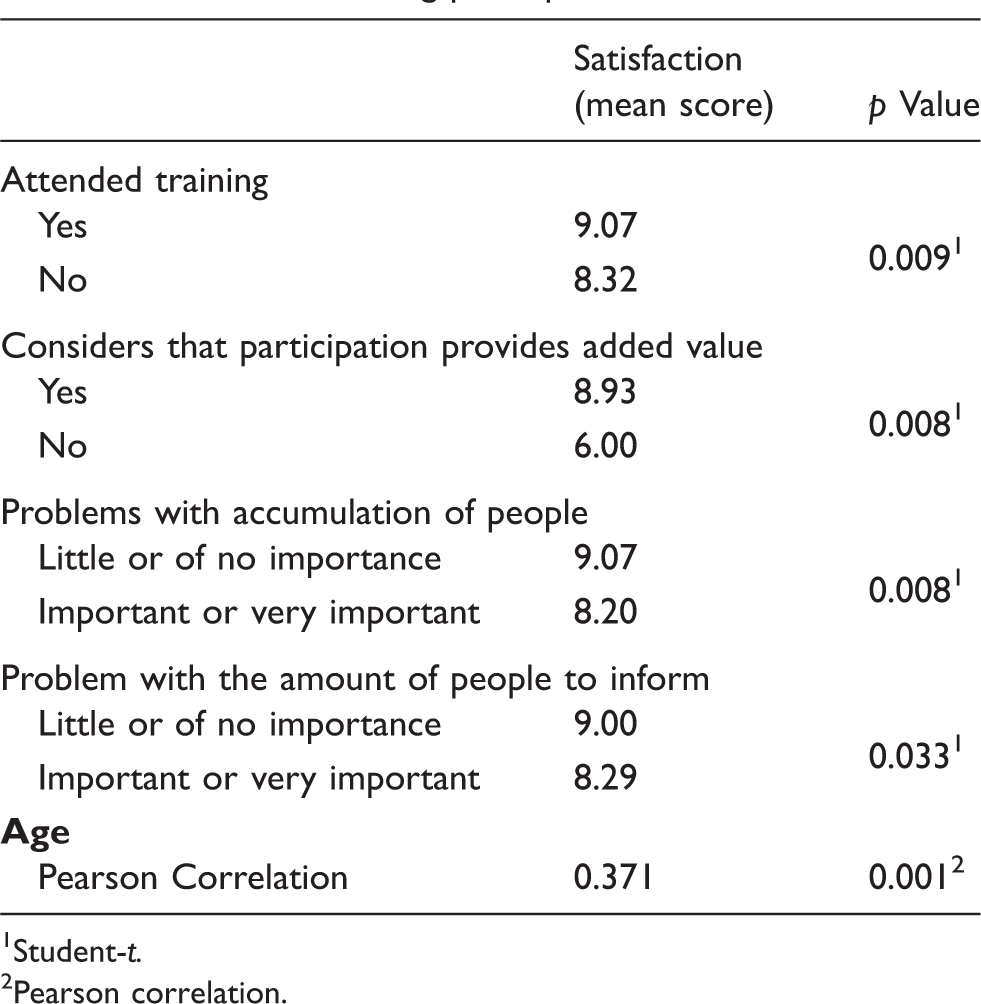
Student-t.
Pearson correlation.
Discussion
The good preparation and the willingness of the pharmacists to participate in screening programs together with the high frequentation by the target population make them an ideal option to implement population-based and at-risk-targeted screening programs. Several studies have demonstrated the viability of using pharmacies for the introduction of secondary prevention activities.7,12 In most of these studies, the main activities carried out by pharmacists were health promotion and disease prevention activities, such as identifying risk factors, providing information, encouraging uptake etc.13,14
The high level of satisfaction and the wide acceptance of the program by the pharmacists observed in our study are probably based on their perception of added value to their professional role and the increasing positive perception of the users on pharmacists as health professionals, associated to a moderate workload. Their participation favours an integrated healthcare and is perceived as a positive experience by the users, 15 increasing their satisfaction on the role of the pharmacists and community pharmacies. However, the workloads also play a fundamental role, since the main task of the pharmacists is to dispense medicines. Thus, they should have enough time to exercise the role of expert advisor in health promotion and disease prevention activities. 13
For the optimal collaboration of pharmacists, it is recommended to develop training activities that enable them to acquire the necessary knowledge to implement the program.7,16–18 In our study, the attendance at the briefing, which was very positively assessed, was significantly associated with the satisfaction of having participated in the program.
Pharmacists positively valued some elements for implementing the program. Firstly, many of them pointed the importance of receiving feedback on the program results in their area of influence. Knowing participation, positivity and detection rates enables them to assess the utility of the program and to use this information in subsequent rounds. 19 Another positive aspect is obtaining a better public recognition of their professional work, a factor that has also been evaluated in other studies as an enabler of the professional change in the pharmacy.20,21 Pharmacists, despite considering preventive activities as very important, prioritise activities associated with the dispensing of medicines, since their payment system is based on this. Therefore, it is desirable to formally and specifically hire these activities, 22 since maintaining these voluntary services threatens the continuity and success of the program. 21
The aspects that cause difficulties and distortion when implementing the program are the time allocated, the amount of customers in the pharmacy that had to be informed and needed their queries answered and the accumulation of people in the pharmacies. These three elements are intertwined, since the fact that people are not sufficiently informed significantly increases the time to attend to them and, in turn, more people accumulate. The origin of the problem is the great amount of people attending the pharmacies, as the PDPCCR is a population-based program, combined with a need to ask, as the population has limited information on chronic processes when there is a low risk perception. 23 On the other hand, the lack of time is considered as one of the most important barriers to implementing new services in community pharmacies, an issue shared with other healthcare levels. 20 These barriers demand sometimes to have more human resources and, thus, an increase in costs. In our study, despite many of those interviewed considered that participation in the program involved a considerable effort and distortion, more than half of them considered that it had not affected the operating dynamics of the pharmacy.
The study has some limitations. Firstly, it was conducted in the city of Barcelona, and may not be extrapolated to other geographic areas. Other limitations are the small sample size and the voluntary participation of the pharmacies in the program, which could lead to a bias towards a greater interest by the pharmacists and, therefore, a higher proportion of more positive/satisfactory responses to the questionnaire. In addition, the study was conducted early in the implementation of a broader program, so perceptions and attitudes may evolve as the program continues.
Conclusions
To involve community pharmacies on prevention activities can be a way of increasing public uptake and helps in implementing a population-based, organized screening program for colorectal cancer, to the extent that it favours accessibility to this kind of program. The overall level of professional satisfaction was high, despite the effort required to participate. The main elements that make it easier are motivation and training of pharmacists using a briefing program to improve their knowledge, and the perception of attending satisfactorily to their reference population. On the other hand, the timely accumulation of consumers, the time spent giving information to the potential participants as well as the absence of a specific remuneration can be some barriers to its optimum implementation.
Footnotes
Authors’ contributions
R Guayta designed the study; M Santolaya conducted the questionnaires and transcribed them to database and made a first analysis. M Aldea, J Grau and R Guayta carried out the interpretation of the results and the first versions of the article. All the authors helped in the critical review of the manuscript and have approved the final draft.
Author note
PROCOLON is the research group of the Barcelona’s Colorectal Cancer Screening Program, and currently consists of the following members:
Cristina Álvarez, Montserrat Andreu, Josep M Augé, Francesc Balaguer, Mercè Barau, Xavier Bessa, Felipe Bory, Andrea Burón, Antoni Castells, Xavier Castells, Mercè Comas, Rosa Costa, Ricard Courtier, Míriam Cuatrecasas, Josep M Dedeu, Maria Estrada, Imma Garrell, Jaume Grau, Rafael Guayta, Cristina Hernández, Mar Iglesias, María López-Cerón, Francesc Macià, Leticia Moreira, M Francisca Murciano, Pilar Gascón, Gemma Navarro, Teresa Ocaña, Pilar Rius, Maria Pellisé, Mercè Pintanel, Mercè Piracés, Sandra Polbach, Àngels Pozo, Anna Reig, Cristina Rodríguez, Maria Sala, Agustín Seoane, Anna Serradesanferm, Judith Sivilla and Antoni Trilla.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.