
Abstract
Background
Lung cancer patients have a high risk for drug–drug interactions, as they use numerous types of concomitant medicines including antineoplastic agents, cancer treatment co-medication, and medicines aimed at several types of comorbidities.
Objective
The primary objective of this study is to determine the incidence and the clinical relevance of the drug–drug interactions between antineoplastic agents and regular medication used by lung cancer patients. Secondary objectives are (i) to determine the effectiveness of the medication review by the hospital pharmacists concerned, (ii) to establish which patients are most at risk of drug–drug interactions and (iii) to determine whether physicians comply with advice given by hospital pharmacists.
Setting
This prospective study was undertaken in a Dutch hospital pharmacy, at Onze Lieve Vrouwe Gasthuis (OLVG), Amsterdam.
Methods
All lung cancer patients receiving one or more cytotoxic agents during the period 21 June 2010 till 2 December 2014 at OLVG were included. The medication list of the patients was obtained electronically from the community pharmacy and checked for interactions by a hospital pharmacist. Interactions that required intervention according to the national database were the only ones taken into account. Interventions were recorded in the patients’ electronic charts. All medication reviews were cross-checked and analyzed by an independent pharmacist at the end of the study period.
Main outcome measure
Prevalence and clinical relevance of drug–drug interactions between antineoplastic agents and other types of medication in lung cancer patients.
Results
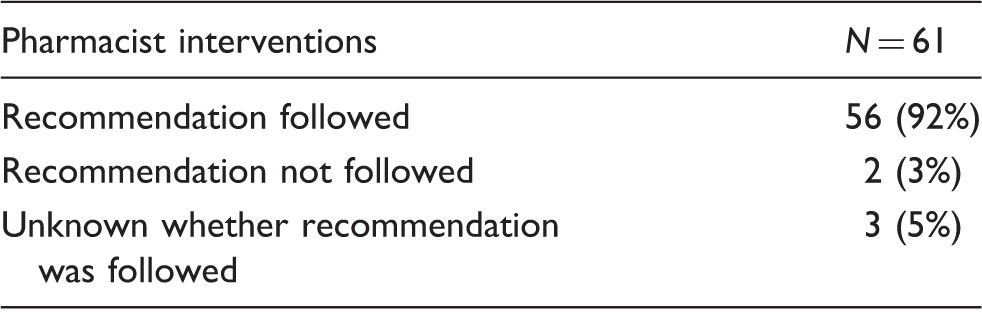
A total of 298 lung cancer patients were included in this study. In 53 patients (18%), a total of 73 interactions with potential clinical relevance were found. The most frequent interaction was between cytostatics and coumarins while the most relevant one was between cisplatin and furosemide. According to statistical analysis, gender as well as the number of drugs prescribed were significant predictors for drug–drug interactions. Eighty-four percent of the interactions were discovered by pharmacists during daily routine. In 92% of the cases, the pulmonary physicians complied with the advice of the pharmacist.
Conclusion
Eighteen percent of lung cancer patients treated with cytotoxic therapy had one or more relevant drug–drug interactions. This study shows that medication surveillance by a hospital pharmacist is necessary to prevent possible negative drug–drug interactions. Further research should focus on the clinical outcome of the interactions as well as on interactions between cytostatics and alternative medicines and/or over-the-counter medicines.
Introduction
Chemotherapy is the most commonly used therapy for lung cancer. This kind of therapy usually consists of combinations of different cytotoxic agents. In addition to chemotherapy, patients often use other drugs to treat comorbid conditions, cancer-related symptoms, or chemotherapy-induced toxicity. The combination of these different drugs has a high potential for drug-drug interactions.1–4
Drug–drug interactions may cause prolonged hospitalization, depending on the nature of the drug–drug interaction, which may even be life threatening. Timely recognition and intervention may hence prevent serious drug-related health damage. According to a large Dutch study on hospital admissions related to medication use, 5.6% of hospital admissions is drug-related and 46% of these could have been prevented.3,5
Quite a number of researchers pointed at drug–drug interactions between cytotoxics and other drugs. However, as yet no studies on this subject specifically concerning lung cancer patients have been reported. The study of Bulsink et al. and Voll et al. excluded lung cancer patients either because of their poor prognosis (15% of the observed population had lung cancer) or because the hospital lung ward used a different administrative program. In other studies lung cancer patients were included but only in small numbers; Lopez-Martin et al. (n = 17; 23%), Van Leeuwen et al. (n = 23; 8%). The previous studies into the medical or general oncology population have shown interactions between antineoplastic agents and coumarin derivatives, antiepileptics, triazole derivatives, proton pump inhibitors, antiretroviral drugs, antibiotics, and folic acid. The average rate for drug–drug interactions in previous studies with anti-cancer drugs lies between 4% and 40%.1,4,6,7 Lopez-Martin et al. 8 not only focused on drug–drug interactions but also on the role of the pharmacist and, if interactions were discovered, whether recommendations made by him were followed, which appeared to be the case in 94% of the cases. We aimed to investigate whether the recommendations and findings of studies on drug–drug interactions in medical oncology patients also apply to lung cancer patients.
Our study is the first prospective study to focus specifically on lung cancer patients.
Aim of the study
The primary aim of this study was to determine the incidence of drug–drug interactions between community-dispensed drugs and cytostatics in lung cancer patients that necessitated an intervention.
Secondary objectives were to determine the effectiveness of the drug screening by a hospital pharmacist, to establish which subpopulation of patients is most at risk for drug-drug interactions and to examine whether doctors comply with recommendations given by hospital pharmacists.
Methods
Study design
The study protocol was approved of by the medical-ethical commission (MEC) of Onze Lieve Vrouwe Gasthuis (OLVG). This prospective study was undertaken in the OLVG in Amsterdam in the Netherlands. The OLVG is a large teaching hospital (550 beds), which treats about 70 lung patients with chemotherapy annually.
We performed a review of each included patients’ actual medication chart, using the medication dispensing history delivered electronically by the community pharmacy, to identify possible interactions with chemotherapeutic agents before starting the first round of a specific type of chemotherapy. If the patient received a second cycle of chemotherapy, he was included again. The patients’ medication was prospectively screened by five different hospital pharmacists in daily routine, and again reviewed for interactions, after completion of the trial period, by an independent research pharmacist. The latter screening was performed to determine the efficacy of the pharmacists’ prospective screenings and also, by checking the medical history of the patients, to establish the extent to which physicians complied with recommendations given by pharmacists. As soon as a drug–drug interaction was detected the hospital pharmacist consulted the attending physician by phone and documented his advice in the patients’ file.
Only interactions which required intervention by the pharmacist were included in this study. All interactions that did not require an intervention were excluded. To detect and assess the potential drug–drug interactions the following sources were searched: PubMed, Micromedex, the Flockhart P450 table as well as several Dutch databases for medication surveillance.9–12
Collecting data
The collected data included the medication history; sex; date of birth; age; start of chemotherapy; antineoplastic agents; type of lung cancer or lung fibrosis and the prevalence of interactions. The number of medications for each patient was calculated by adding up all different medications except for the antineoplastic drugs. If a patient used more than one dosage forms of the same drug it was counted only once.
The data were collected from the patients’ electronic charts and transferred to an Excel file. This Excel file was used to assess the interactions and classify them according to severity.
Classification of the drug interactions
Classification of the interactions according to Koninklijke Nederlandse Maatschappij ter bevordering der Pharmacie (KNMP). 13
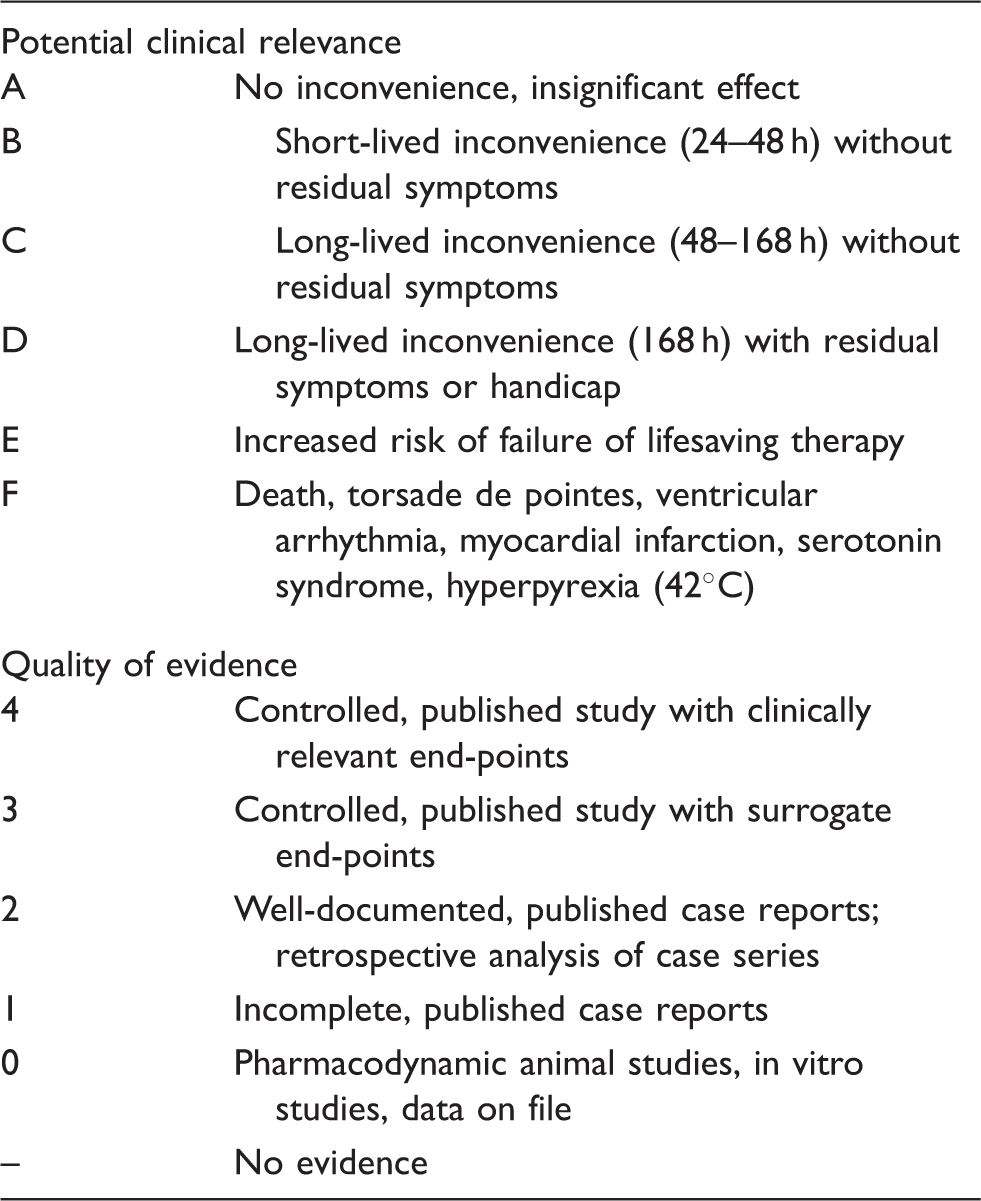
The potential clinical relevance is derived from the Common Toxicity Criteria for Adverse Events (CTCAE) of National Cancer Institute. Grades B–F correspond with toxicity classifications 1–5. 14
Patients
Inclusion criteria for this study were treatment with cytotoxic therapy for lung cancer, mesothelioma, thymic carcinoma, or lung fibrosis, administered in the hospital, in the period from 21 June 2010 to 2 December 2014. These patients could be in- or outpatients. Patients receiving oral therapy for lung cancer administered outside the hospital were not included as their compliance could not be monitored and because oral chemotherapy is not dispensed by the hospital pharmacy.
Patients had to be >18 years. The patients were enrolled if an actual drug list could be reviewed.
Statistical analysis
The data were processed using Microsoft Excel 2010.
On drug–drug interactions in lung oncology no data were available on which to base our sample size. A sample of 300 patients was considered feasible. Patients were included in this study until this number was reached. Descriptive statistics (median (25–75%)) and frequency analysis (number (%)) were applied to describe the whole study sample with regard to patient characteristics (such as sex, age, prescribed drugs, lung cancer type, and treatment intention), types and classifications of drug interactions.
The Mann–Whitney U-test and the Pearson chi-square test were used to identify which subpopulation of patients was most at risk for drug–drug interactions. The dependent variable was occurrence of an interaction while the explanatory variables were age, sex, lung cancer type, treatment intention, and the number of drugs. Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 22.0. (Armonk, NY: IBM Corp.,). If the p-value was less than 0.05, the test result was considered statistically significant.
Results
Patient characteristics
For this study a total of 300 patients were found eligible. Two patients, however, did not have their community pharmacies working with the generally used electronic database, hence no active medication list could be accessed. Therefore they had to be excluded from the study.
Patient characteristics and the amount of potential clinically significant interactions (CSI) by characteristic.
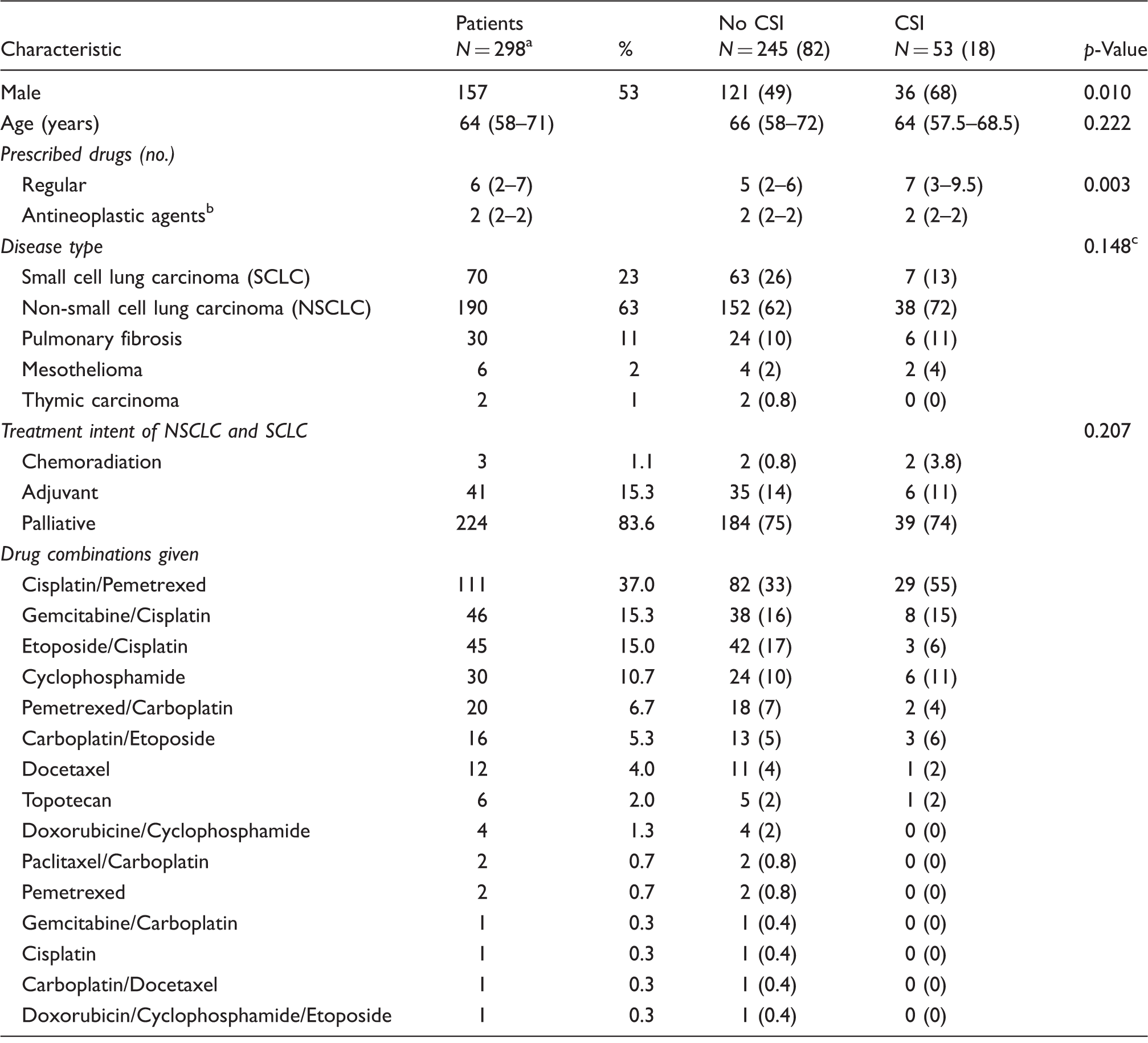
All variables in this table are described as number (%) or median (25–75%).
Two patients were excluded, because it was not possible to get their medication list.
In most cases, two antineoplastic agents were given; in the case of lung fibrosis always one agent was given.
p-Value was calculated separately for cases of small cell lung carcinoma, non-small cell lung carcinoma and for a combined group of other types of lung diseases.
Medication surveillance
Number of recommendations by pharmacists followed by physicians.
There was a total of 73 interactions in 53 patients, of which 12 were not detected by the pharmacists.
Possible interactions found
The identified drug–drug interactions between cytotoxic agents and other drugs.

There were more potential interactions with metformin, but only when an action was required this interaction was taken into account. All metformin patients with an estimated glomerular filtration rate (eGFR) higher than 60 were excluded, as patients with a higher eGFR have a smaller risk of developing a significant renal failure.
Table 4 shows that coumarin derivates in combination with antineoplastic agents accounted for the most frequently observed interaction with a classification 1D (36%). Interactions between NSAIDs and cisplatin (32%) (classification of the interaction: -/D) and methotrexate with antineoplastic agents (10%) (classification of the interaction: -/E) were also observed regularly.
Potential risk factors
Gender was associated with an increased risk of drug–drug interaction. Female patients had a significantly smaller chance to have an interaction than male patients (p = 0.010). The number of concomitantly used drugs was also a significant predictor for drug–drug interactions with chemotherapy (p = 0.003). The occurrence of drug–drug interactions was not dependent on age, lung cancer type or intention-to-treat. Table 2 shows the p-values of the variables.
Discussion
This study demonstrates that drug–drug interactions frequently occur in lung cancer patients. It also demonstrates the importance of a thorough medication review by a clinical pharmacist to detect drug–drug interactions and to propose interventions for their management.
The hospital pharmacy of OLVG found 73 relevant drug-drug interactions in 298 lung cancer patients between regular medication and antineoplastic agents (a total of 2000 drugs). In this study only clinically relevant interactions (mainly levels D and E, with the potential of long lived negative health effects), which required an intervention were included. The recommendations made by pharmacists on management of the drug–drug interactions included dose adjustments, drug discontinuation, the monitoring of estimated glomerular filtration rate (eGFR)/ international normalized ratio (INR) levels, therapeutic drug monitoring, or drug substitution.
There was a high degree of compliance by the attending physicians after the need for treatment modification was communicated. The fact that hospital pharmacists are member of the multidisciplinary oncology team may have contributed to this high rate of compliance. In addition, the advice on the management of the observed interactions was given in a concise and directly applicable manner. For example, for the interaction between valproic acid and cisplatin, not only was the possible outcome (risk of lower AUC for valproic acid) communicated, but also the appropriate action (measure baseline valproic acid serum level one week before start of treatment and repeat 1–2 weeks after start, if serum levels decreased, the pharmacist would suggest a dose adjustment and a schedule for repeat serum level measurements). This study confirms the importance of thorough reviewing for drug–drug interactions.
Another strong point of this study lies in the fact that this is the first study with only lung cancer patients. Furthermore, drug–drug interactions were only included if they required intervention.
Yet, this study also has some limitations to be taken into account. Patients were not asked if they were using any kind of complementary or alternative medicines, such as St. John’s Wort, milk thistle or Panax gingseng, which are known to interact with cytotoxics. Patients seldom know that complementary and alternative medicines may influence their chemotherapy, which makes it especially important to ask them.23,24
Furthermore, the prospective screening method was not 100% effective, as the independent analysis of all data showed that hospital pharmacists still missed 16% of the possible drug–drug interactions. In addition, the study was conducted in a single general hospital hence the extrapolation effect to other general or teaching hospitals is not certain.
Finally, the interaction screening was performed only once at the start of chemotherapy. New drugs that were started during chemotherapy were missed, because the hospital software does not automatically inform the community pharmacy of the cancer diagnosis and treatment of the patient. Hence the communication between hospital and community pharmacies needs to be improved. In addition, the clinical outcome of most interactions could not be measured, as the hospital pharmacists intervened and changed medication of the included patients. Clinical outcome measures could therefore not be considered.
In this study we focused on patients receiving intravenous chemotherapy, hence targeted therapy with epidermal growth factor receptor inhibitors, such as erlotinib and gefitinib, generally used at home, were not included.
Other studies reported values for the amount of drug–drug interactions which could be considered comparative, taking into account that our study only included interactions which required intervention. In addition, the most frequent drug–drug interactions seen in this study, between coumarins, methotrexate, and NSAID’s, were also seen in other studies into drug–drug interactions with antineoplastic agents. These antineoplastic agents were not used specifically to treat lung cancer.1,4,6,7 The high rate of compliance with pharmacists' recommendations was also seen in earlier studies, Lopez-Martin et al., 8 for example, found that the advice was followed in 94% of the cases in comparison with 92% in this study.
Conclusion
Drug–drug interactions with antineoplastic agents are common in lung cancer patients. Most interactions are with coumarins and NSAIDs. Clinically relevant interactions should be appropriately dealt with. It is therefore of utmost importance to remain vigilant in detecting these interactions as soon as possible.
Further research should focus on possible effects of the clinical outcome of drug–drug interactions as well as on interactions between complementary or alternative medicines and cytostatics.
Footnotes
Acknowledgements
We thank LM Dijksman, research coordinator at OLVG, for her help with the statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.