
Abstract
The programmed-death-1 inhibitors selectively block programmed-death-1 interaction with its receptor, which restores active T-cell response directed at tumor cells, inducing an anti-tumor effect. This nonspecific activation of the immune system can also lead to a wide spectrum of side effects. Nivolumab has been used effectively to prolong survival in patients with metastatic melanoma and is recommended as a category 1 agent for systemic therapy in metastatic or unresectable melanoma per the National Comprehensive Cancer Network guidelines. We present a case of a 64-year-old woman who began nivolumab therapy for metastatic melanoma. After six doses of nivolumab therapy, the patient experienced generalized hypopigmentation on her face, chest, back, arms, and lower extremities. Although vitiligo has been reported in as many as 10.7% of patients undergoing nivolumab therapy in some clinical trials, we believe this is the first case to describe the progression of nivolumab-induced vitiligo in a metastatic melanoma patient. This case provides significant insight into the onset, symptoms, development, and treatment options for patients experiencing vitiligo as a result of nivolumab therapy.
Introduction
It is estimated that 2%–5% of patients with melanoma present with distant metastatic disease. Patients who present with stage III disease have a five-year survival rate that ranges from 20% to 70%, depending on nodal tumor burden. For those who present with distant metastatic melanoma, long-term survival is less than 10%. While new approvals of immunotherapeutic and targeted agents have provided patients with more treatment options for the initial management of stage IV disease, many of these agents present unique limitations. 1
Targeted therapies for melanoma include BRAF inhibitors, MEK inhibitors, mechanistic target of rapamycin (mTOR) inhibitors, and immunomodulators such as cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) inhibitors and programmed death-1 (PD-1) inhibitors. Nivolumab, along with pembrolizumab, is a PD-1 inhibitor antibody that selectively blocks PD-1 interaction with its receptor which restores active T-cell response directed at tumor cells, inducing an anti-tumor effect.2,3 While nivolumab is designed to unleash the immune system against cancer cells, this nonspecific activation of the immune system can also lead to a wide spectrum of side effects. 4
Nivolumab is indicated as a single agent for patients with BRAF V600 wild-type unresectable or metastatic melanoma, as a single agent following disease progression with ipilimumab in metastatic melanoma patients with BRAF V600 mutation-positive melanoma, or in combination with ipilimumab in patients with BRAF V600 wild-type melanoma. 3 The National Comprehensive Cancer Network (NCCN) 1 published updated treatment guidelines Version 2.2016 for metastatic or unresectable melanoma that include nivolumab as a category 1 recommendation of patients with BRAF V600 wild-type melanoma. In a clinical trial by Larkin et al., 5 progression-free survival (PFS) was assessed in patients who received combination nivolumab plus ipilimumab, nivolumab alone, and ipilimumab alone. Patients experienced grade 3 or 4 adverse events in the combination group, nivolumab alone group, and ipilimumab alone group at a rate of approximately 55%, 16%, and 27%, respectively. Ipilimumab and combination ipilimumab/nivolumab have been associated with significant immune-mediated complications, such as pneumonitis, colitis, hepatitis, and immune-mediated dermatitis. 1 Nivolumab may also cause immune-mediated adverse reactions, though grades 3 and 4 toxicities with nivolumab are less common than with ipilimumab. Cutaneous adverse effects are among the most frequent toxicities seen in these targeted therapies, such as rash, pruritus, and vitiligo.3,4 The development of vitiligo has been seen in patients with no history of autoimmune disorders. 4
Vitiligo is an acquired disease characterized by blotchy depigmentation of the skin caused by a loss of melanocytes from the epidermis. While the exact mechanism of vitiligo is unknown, one theory proposes that the disease is autoimmune in nature and is caused from activation of the inflammatory cascade leading to stimulation of interleukins and the innate immune response. 6 Herein, we describe what we believe to be the first published case report of nivolumab-induced vitiligo.
Case report
A 64-year-old Nigerian woman presented to University Medical Center Brackenridge on 24 April 2012 with a recent diagnosis of malignant melanoma of the left foot. The patient underwent excision of the melanoma which demonstrated acral lentiginous-type melanoma with depth of invasion approximately 6.1 mm. Ulceration was present with no satellitosis. Lymphovascular invasion was also present. The patient underwent wide local excision with left inguinal lymph node dissection on 24 May 2012. The patient was found to have metastatic disease involving two out of two lymph nodes. After complete lymphadenectomy in which six lymph nodes were removed and found negative for disease, the patient did not demonstrate any further evidence of metastatic disease per imaging and pathology report. Adjuvant inguinal radiation was discussed; however, it was not offered due to low nodal burden. The patient declined adjuvant interferon therapy and was on periodic surveillance.
On 6 March 2014, the patient was recommended for biopsy due to hyperpigmentation surrounding the graft site, of which showed recurrent melanoma. Two weeks later, the patient presented to the clinic with anterior thigh nodules of approximately 2 × 2 × 0.9 cm. Patient underwent reexcision on 3 April 2014 as well as a biopsy of two lesions of the anterolateral thigh which were consistent with junctional nevi. Patient was recommended for adjuvant radiation of the left foot which was eventually completed on 21 October 2014.
One month later, the patient presented with multiple new subcutaneous lesions of the left lower extremity, which was found to be recurrent melanoma consistent with in-transit metastasis. BRAF mutation testing was negative for V600K mutations and computed tomography (CT) scan results were negative for systemic disease. The patient was referred to a tertiary center to discuss locoregional options; however, she was not a candidate for these.
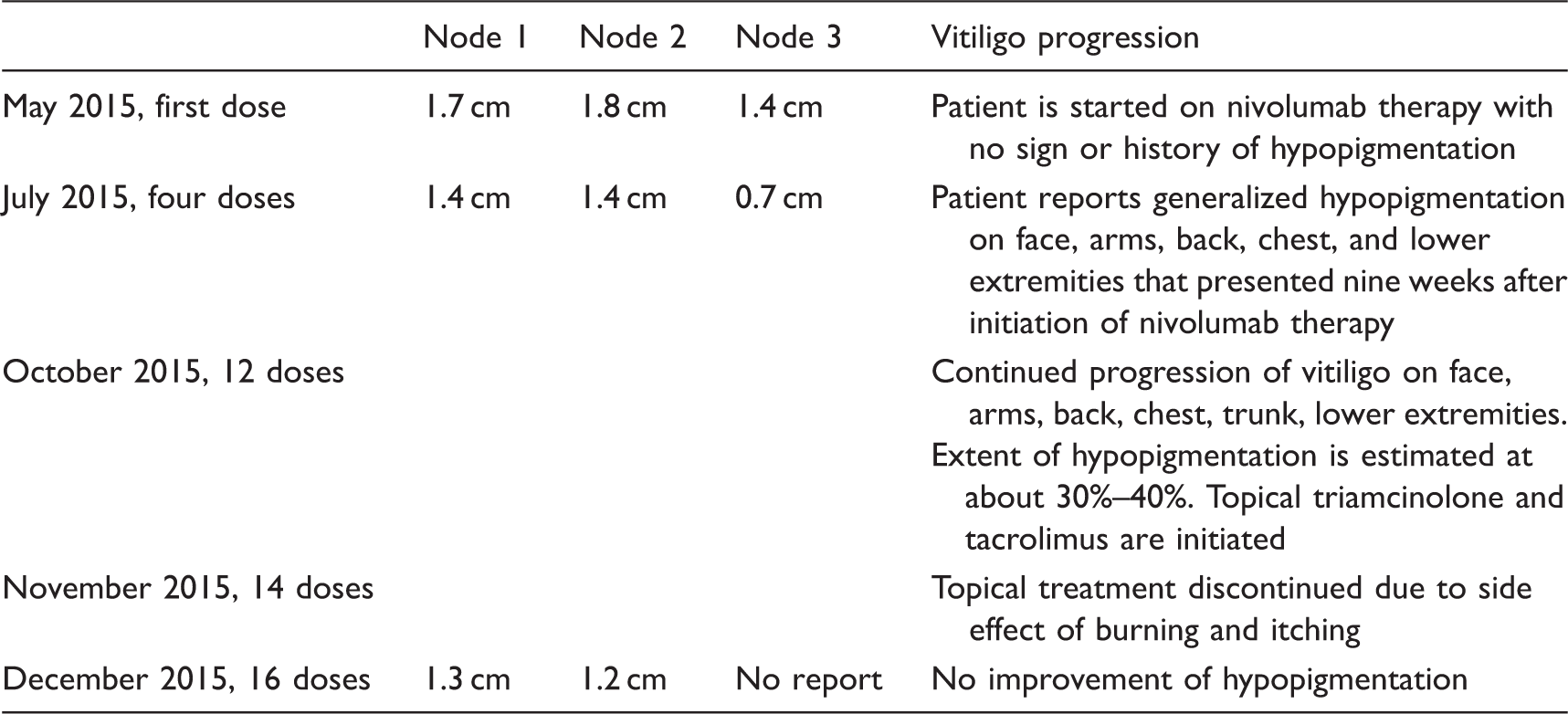
Nivolumab therapy was started in May 2015 at a dose of 3 mg/kg IV every two weeks. After four doses of nivolumab therapy, CT scans showed a reduction in size of three necrotic lymph nodes with no additional lymphadenopathy. After six doses (11 weeks) of nivolumab therapy, the patient presented to the clinic complaining of generalized hypopigmentation of the skin at multiple sites including the face, arms, back, chest, and lower extremities (Table 1). The patient reported observing the first hypopigmentation lesion on her right upper extremity two weeks prior, nine weeks after nivolumab initiation. Preceding the hypopigmentation, the patient reported no side effects other than a mild pruritus. The patient stated the lesions were not painful, though she reported some psychological discomfort. The lesions were completely flat without evidence of scale or excoriation. The vitiligo was categorized using NCI Common Terminology Criteria for Adverse Events as grade 2 due to extent of spread and psychological distress expressed by the patient. 7 The patient has no personal or family history of vitiligo, or any other autoimmune disorder. She takes no medications at home other than ibuprofen as needed and difluprednate eye drops. No new medications were initiated during nivolumab therapy.
Timeline comparing nodal response and vitiligo progression.

Vitiligo appearance after 12 doses of nivolumab.
Discussion
Vitiligo is an acquired dermatologic disease that has been associated with use in immunomodulatory agents, especially the PD-1 inhibitors nivolumab and pembrolizumab. 4 This adverse effect may be related to the mechanism of the drugs involving activation of T-cells. Because nivolumab restores active T-cell response, it is not surprising that it would be connected to vitiligo, which is likely associated with T-cell destruction of melanocytes. 6 Skin hypopigmentation is categorized as grade 1 or 2 depending on extent of disease and psychological impact. Vitiligo is categorized as grade 1 when covering less than 10% body surface area with no psychological impact. Grade 2 hypopigmentation is defined as depigmentation covering greater than 10% of the body surface area with symptoms of psychological impact. 7
In several clinical trials, nivolumab has been associated with vitiligo. In a phase 3 study that compared dacarbazine and nivolumab for overall survival (OS), incidence of vitiligo (grade 1 or 2) was 10.7% or 22 of 206 patients in the nivolumab arm (Table 2). 2 The grade of the vitiligo was reported as less than 3 which was determined using the National Cancer Institute Common Terminology Criteria for Adverse Events. Another study that focused on OS of patients treated with nivolumab found an association of 9.3%, or 10 patients who developed grade 1 or 2 vitiligo after nivolumab initiation. 8 No further details of the adverse reaction were provided by either study.
The patient presented in this case report displayed symptoms of vitiligo about nine weeks after initiating therapy with nivolumab, about three years after diagnosis of melanoma. Because of the patient’s good response to the therapy, after discussion with our patient, we opted to continue with the treatment despite the progressive hypopigmentation. Based on the adverse drug reaction probability scale of Naranjo et al., 9 this adverse reaction was given a score of 6, indicating a probable association between vitiligo and nivolumab.
Incidence of vitiligo in clinical trials.

Another possible cause of vitiligo in melanoma patients is melanoma-associated hypopigmentation (MAH) which has been observed in 2%–16% of melanoma patients either spontaneously or concurrently with treatment and has been observed for over 40 years.14,15 Melanoma patients develop vitiligo at about a 7- to 10-fold higher rate than the general population. 15 A study by Hartmann et al. studied 15 melanoma patients with hypopigmented areas to determine the relationship between the two diseases. In 3 of the 15 patients with melanoma, hypopigmentation appeared years prior to diagnosis of melanoma and was deemed not associated with the skin malignancy. For the remaining 12 patients, the hypopigmentation appeared on average 4.8 years after the initial diagnosis of melanoma. Three patients reported an association of hypopigmentation with interferon or chemotherapy. None of these patients had a family history of vitiligo and only one had a family history of autoimmune disease. Seventy-five percent of MAH patients had a bilateral symmetrical distribution consistent with classic vitiligo while 25% of patients presenting with asymmetrical distribution. MAH was less progressive than classic vitiligo for these patients. 14
A prospective observational cohort study was designed to study patients from 1980 to 2007 to determine if hypopigmentation is a positive prognostic factor in patients with melanoma. A total of 2954 melanoma patients were included in the study. Vitiligo occurred in 83 patients, or 2.8%. Twenty percent of the patients had vitiligo before melanoma diagnosis, 45.5% developed vitiligo after surgical excision of primary melanoma, 42.4% after locoregional metastases, and 12.1% after distant metastases. Vitiligo occurred after treatment with interferon, interleukin-2, or chemotherapy in 24.2% of patients, corresponding to 3% of all patients treated with immunotherapy. The study found that there was no survival benefit of vitiligo in patients with stage I or stage II melanoma. However, in patients with stage III, five-year survival was 65% in vitiligo patients versus 42.5% in patients without vitiligo, a significant difference. Stage IV melanoma patients also saw the positive effect, with OS of 14.4 versus 9.6 months. 15
The goal of treatment for vitiligo is to achieve repigmentation and to stabilize the disease. Treatment recommendation guidelines are intended for idiopathic vitiligo patients with no recommendations available for melanoma or treatment associated vitiligo. Supportive care measures include psychological support and counseling and utilizing sunscreen for lesions on exposed skin. Topical corticosteroids and calcineurin inhibitors, such as triamcinolone and tacrolimus, are recommended as first line treatment options.6,16 Topical calcineurin inhibitors are recommended for facial and neck lesions as an alternative to steroids. Second line options consist of phototherapy and systemic steroids. These treatment recommendations are thought to work by suppressing the immune system, opposing the effect of the targeted therapy used to promote an attack on the tumor. Therefore, it is not recommended to use systemic steroids to treat vitiligo that is associated with melanoma or chemotherapy.
Conclusion
Vitiligo is a known adverse event associated with nivolumab treatment based on previous trials, but further details are not available. Whether repigmentation will occur after discontinuation of the drug is yet to be determined. This case provides clinicians with a basis of what to expect in regards to onset, extent, and progression of nivolumab-induced vitiligo.
While vitiligo is commonly viewed as a benign disease, patients can often suffer from psychological distress, especially in dark-skinned individuals. 6 It is probable that nivolumab is responsible for the vitiligo seen in this patient based on the short duration of time between nivolumab initiation and hypopigmentation appearance in this case, as well as the rapid progression of hypopigmentation. The patient in this case presented with hypopigmentation on her right upper extremity approximately nine weeks after beginning nivolumab therapy. Within three months, the patient presents with hypopigmentation covering approximately 30%–40% of her body surface area. However, because the patient continues to have a good response to the drug, she will continue on nivolumab indefinitely. Additionally, vitiligo treatment with the topical agents may be considered again if patient requests and the patients assessed for improvement.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.