
Abstract
Primary myelofibrosis is characterized by bone marrow fibrosis, splenomegaly and presence of JAK-2 V617F mutation in more than 90% of patients. Ruxolitinib is a Janus kinase inhibitor used for the treatment of primary myelofibrosis. We describe herein a persistent foot ulcer development attributed to ruxolitinib therapy. We are unaware of any previous reports of this phenomenon in the scientific literature. A thorough examination of the lower extremities is perhaps necessary before initiating this oral agent. If ruxolitinib therapy cannot be safely discontinued, diligent wound care and a course of antibiotics are warranted.
Primary myelofibrosis is a myeloproliferative disorder characterized by bone marrow fibrosis and is often associated with palpable splenomegaly and JAK-2 V617F mutation. 1 Ruxolitinib is a Janus kinase (JAK) inhibitor approved by the United States Food and Drug Administration for the treatment of primary myelofibrosis and polycythemia vera. 2 We describe herein a persistent foot ulcer in a patient treated with ruxolitinib.
Case presentation
A 79-year-old man was seen as outpatient in May 2016 for a skin ulcer involving the medial aspect of the second left toe.
In May 2014, the patient presented with fatigue and a 15-lb weight loss over the previous 6 months. Physical examination revealed splenomegaly. Peripheral blood showed a modest thrombocytopenia. Testing on the peripheral blood for with JAK-2 V617F mutation was positive. A bone marrow biopsy showed reticulin grade 3 fibrosis. He was diagnosed with JAK-2 V617F mutation positive primary myelofibrosis. He was started on low-dose aspirin and followed as outpatient.
In June 2015, he developed increasing fatigue, weight loss, and early satiety. His spleen had increased in size as well. Therefore, he was started on ruxolitinib 15 mg tablet orally twice daily. In July 2015, he developed progressive fatigue, anemia (hemoglobin 8.3 g/dL; normal 13.5–16 g/dL), and worsening thrombocytopenia (platelet count 66,000/mcL; normal 150,000–450,000/mcL). This was attributed to ruxolitinib use in the context of chronic kidney disease with a baseline creatinine of 1.6 mg/dL (normal, <1.0 mg/dL). Therefore, the dose of ruxolitinib was reduced to 5 mg orally daily. His symptoms and laboratory data returned to the baseline over the next 8 weeks. The spleen decreased significantly in size by the end of September 2015. The hemoglobin and platelets improved to 13 g/dL and 130,000/mcL, respectively. Since then, he remained on ruxolitinib, while the primary myelofibrosis has been in remission since January 2016.
Medical history included benign prostatic hypertrophy, chronic kidney disease, gout, hypertension, and insomnia. The patient denied any allergies. His medications included ruxolitinib, allopurinol, amlodipine, finasteride, tamsulosin, and trazodone. Ruxolitinib was the most recent medication started on his list. He denied using any vitamin/mineral supplements or other complementary therapies. Family history was negative for hematologic or oncologic disorders. The patient was married and retired. He was a daily smoker who smoked 1 pack/day for 61 years and refused to quit despite frequent tobacco cessation counseling. He consumed one alcoholic beverage a day. He reported no contact with hazardous materials. On review of systems, the patient reported moderate fatigue and dyspnea on exertion. He denied any other symptoms.
On physical examination, the patient had a 1.5 × 1.0 cm ulcer on the medial side of the second left toe (Figure 1). It was 0.4 cm deep, with a pink wound bed without slough. The patient had pale skin and conjunctivae. Lung examination showed somewhat decreased breath sounds on auscultation. The spleen was non-palpable. The rest of his physical examination was unremarkable.
Ruxolitinib induced ulcer involving the medial aspect of the second left toe.
The patient followed up with his dermatologist. The wound cultures were negative for bacterial and fungal growth. Viral serologies were negative. Dermal brushing of the wound demonstrated no atypical cells. An X-ray of the foot and a subsequent bone scan were normal. Biopsy of the ulcer showed a thin layer of epidermal re-epithelialization and granulation tissue formation in the dermis consistent with an inflammatory reaction.
The patient was referred to a wound care specialist. He was started on cephalexin 500 mg orally four times per day for 14 days. He continued to follow with wound care, with a documented complete healing in August 2016. At the time of writing this report, the patient had been ulcer-free for 12 weeks. He continues ruxolitinib therapy, with no other significant toxic effects.
Discussion
In 2005, the JAK2 V617F mutation was identified as the most common abnormality in myeloproliferative disorders. 3 Further exploration showed that dysregulation of the JAK signaling pathway was involved in patients with myelofibrosis, regardless of V617F mutation. 4
Ruxolitinib selectively inhibits proliferation of JAK2 V617F driven cells in myelofibrosis. A phase 3 clinical trial demonstrated that ruxolitinib therapy, as compared to the best available therapy, was associated with marked and durable reductions in splenomegaly and disease-related symptoms. A total of 28% of the patients in the ruxolitinib group had at least a 35% reduction in spleen volume at week 48, as compared with 0% in the group receiving the best available therapy (P < 0.001); the corresponding percentages at week 24 were 32% and 0% (P < 0.001). 5 Common hematologic abnormalities of ruxolitinib included anemia and thrombocytopenia, which were managed with reduction in dose, stopping treatment, or transfusion. The most common nonhematologic adverse event was diarrhea.
The Naranjo adverse drug reaction (ADR) probability scale questionnaire.
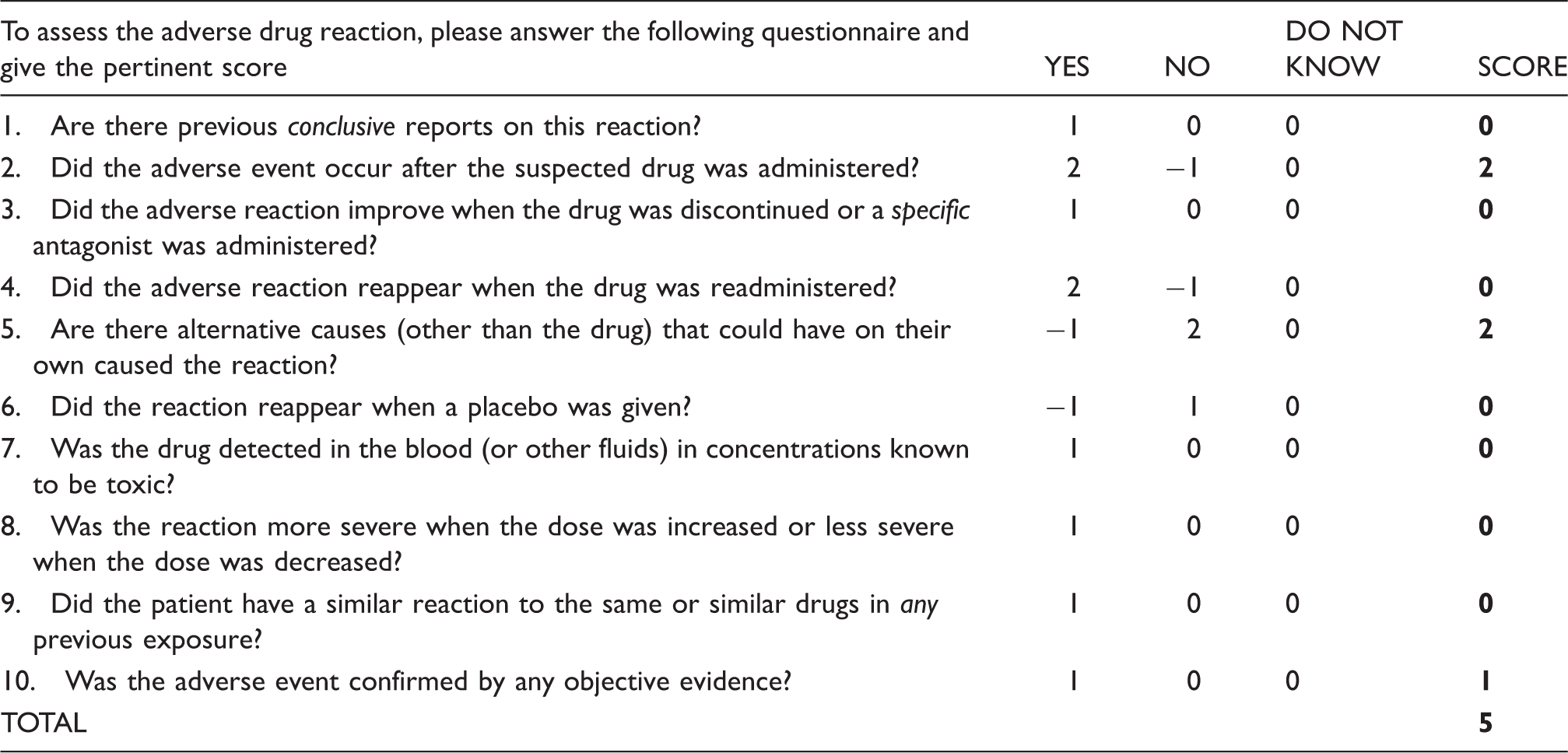
The Naranjo criteria classify the probability that an adverse event is related to drug therapy based on a list of weighted questions, which examine factors such as the temporal association of drug administration and event occurrence, alternative causes for the event, drug levels, dose–response relationships and previous patient experience with the medication. The ADR is assigned to a probability category from the total score as follows: definite if the overall score is 9 or greater, probable for a score of 5–8, possible for 1–4 and doubtful if the score is 0. The Naranjo criteria do not take into account drug–drug interactions. Drugs are evaluated individually for causality, and points are deducted if another factor may have resulted in the adverse event, thereby weakening the causal association.
In the original ruxolitinib trials, patients with leg ulcers were excluded because of concerns of infection, the rates of which are increased by this agent.2,5 This stresses the importance of reporting this adverse drug event, as the development of an ulcer while on ruxolitinib includes the possibility of infection and further complications. Infection was effectively eliminated from the list of etiologies in the patient. Fortunately, the ulcer resolved after a course of antibiotics and serial sessions of wound care. Remarkably, the lower extremity ulcer developed on a low dose of ruxolitinib, which had to be adjusted due to the patient’s chronic kidney disease, anemia and thrombocytopenia.
Interestingly, Shanmugam et al. 7 reported a patient with polycythemia vera treated with hydroxyurea who developed a chronic leg ulceration. They described healing of the ulcer after initiation of ruxolitinib. It should be noted that their patient’s leg ulcer healed in association with discontinuation of the hydroxyurea, which is consistent with management of hydroxyurea induced leg ulcers.8,9 Regardless of the outcome, we feel that it is important to report a probable ruxolitinib-induced foot ulcer as this observation merits further investigations.
In conclusion, as this is the first report of a foot ulcer probably caused by the therapy with ruxolitinib, we advocate caution in this regard. A thorough examination of the lower extremities is warranted before initiating this oral agent. If ruxolitinib therapy cannot be safely discontinued, wound care and a course of antibiotics are definitely in order.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.