
Abstract
Purpose
Denosumab is a crucial supportive care agent for patients with advanced cancers affecting the bone. Despite the importance of treatment, logistical and financial obstacles hinder the ability to maintain long-term adherence. This analysis was designed to provide preliminary data regarding the feasibility of extended denosumab dosing intervals.
Methods
This retrospective, case cohort study was conducted on patients receiving treatment with denosumab for malignancies with bone involvement. A total of 60 patients were identified for analysis and were divided into cohorts according to the average number of days between denosumab doses. The standard interval group was comprised of patients receiving treatment once every 27–30 days (n = 29), whereas the deviated interval group was comprised of patients with an interval of 31–56 days between injections (n = 31). The primary outcome was the percentage of patients developing a skeletal-related event. Secondary efficacy outcomes included rate of pathologic fracture, spinal cord compression, radiation therapy, surgery, and hypercalcemia.
Results
Patients in the deviated interval arm experienced significantly more skeletal-related events compared to the standard interval group (61% vs. 31%, respectively; p = 0.02). Secondary efficacy endpoints trended in favor of the standard therapy arm except for requirement for surgery (results were virtually equivalent) and hypercalcemia (no events in either group).
Conclusions
Non-adherence with the standard denosumab dosing schedule demonstrated an increased risk of experiencing a skeletal-related event. Preservation of denosumab dose density appears imperative to maintain efficacy and as such extending the dosing interval should be discouraged.
Background
Over 400,000 patients with cancer develop skeletal metastases annually in the USA. 1 Though the occurrence is greatest in breast and prostate cancers, patients with numerous other tumor types including thyroid, kidney, lung, and gastrointestinal tract cancers can be impacted. 2 In addition to pain and hypercalcemia of malignancy, skeletal metastases have the propensity to lead to more adverse consequences collectively referred to as a skeletal related event (SRE). This is defined as anyone of the following sequelae: pathologic fracture, spinal cord compression, requirement of radiation therapy due to pain or impending fracture, or surgery to the bone. 3 In addition to severe pain and a reduced quality of life, development and subsequent management of SREs results in increased health care costs.
In current clinical practice, zoledronic acid, an intravenous bisphosphonate, and denosumab, a subcutaneously administered monoclonal antibody which inhibits receptor activator of nuclear factor kappa-B ligand (RANKL) inhibitor, are utilized routinely to prevent or delay the development of SREs.3,4 In head-to-head clinical trials, denosumab and zoledronic acid have demonstrated similar efficacy and safety profiles. Denosumab has demonstrated superiority over zoledronic acid in breast and prostate cancer and non-inferiority in other solid tumor malignancies and multiple myeloma.5–7 Both agents, which are conventionally dosed every four weeks in this setting, can create significant logistical challenges when attempting to incorporate them along with concomitant cancer therapies, clinic appointments, lab testing, and imaging. 4
In the ZOOM trial, Amadori et al. demonstrated that increasing the interval between doses of zoledronic acid from every 4–12 weeks after completion of one year of the conventional monthly regimen resulted in preserved clinical efficacy in patients with breast cancer. 8 The concept of extended dosing intervals for bone targeting agents is compelling as it offers a means to increase patient convenience and provide significant financial savings. Denosumab, with a half-life approximately four times longer than zoledronic acid (25–28 days vs. 146 h), appears to be an ideal candidate for this approach.9,10 This study was designed to provide preliminary evidence regarding the feasibility of applying extended dosing intervals to denosumab therapy.
Methods
This retrospective, case cohort study was conducted at a cancer center affiliated with an academic medical center and was approved by a local investigational review board. Patients initiated on treatment with denosumab from 2012 to 2015 were divided according to the average time between denosumab administrations. Patients were included in the study if they were 18 years of age or older, had an active diagnosis of cancer, and received two or more doses of denosumab (120 mg per dose given subcutaneously). Patients were excluded if they received concurrent maintenance bisphosphonates or if there was insufficient data in the electronic medical record to determine outcomes. Patients were never deliberately assigned to receive extended frequency dosing; rather, deviations occurred due to unanticipated events including scheduling conflicts or patient non-adherence.
In order to establish comparable cohorts, patient groups were defined by identifying natural groupings of data within the research population (Figure 1). Out of a total of 122 unique patients receiving at least one dose of denosumab during the study period, 62 patients qualified for inclusion. Two of these patients who were eligible displayed extremely prolonged average treatment intervals (70 and 112 days) and were ultimately excluded from final analysis due to dissimilarity from the remainder of included patients. The standard interval group consisted of patients with average treatment intervals clustered around the customary dosing of once every 28 days and included a total 29 patients receiving treatments on average of once every 27–30 days. The deviated interval group was comprised of 31 patients with an injection frequency exceeding the standard interval cluster (range 31–56 days). For further analysis, the deviated interval group was further divided into a minor deviation (range 31–39 days; n = 23) and major deviation (range 41–56 days; n = 8) sub-groups.
Distribution of patients according to average number of days between denosumab treatments (each mark represents one patient) and selection of cohorts and sub-groups.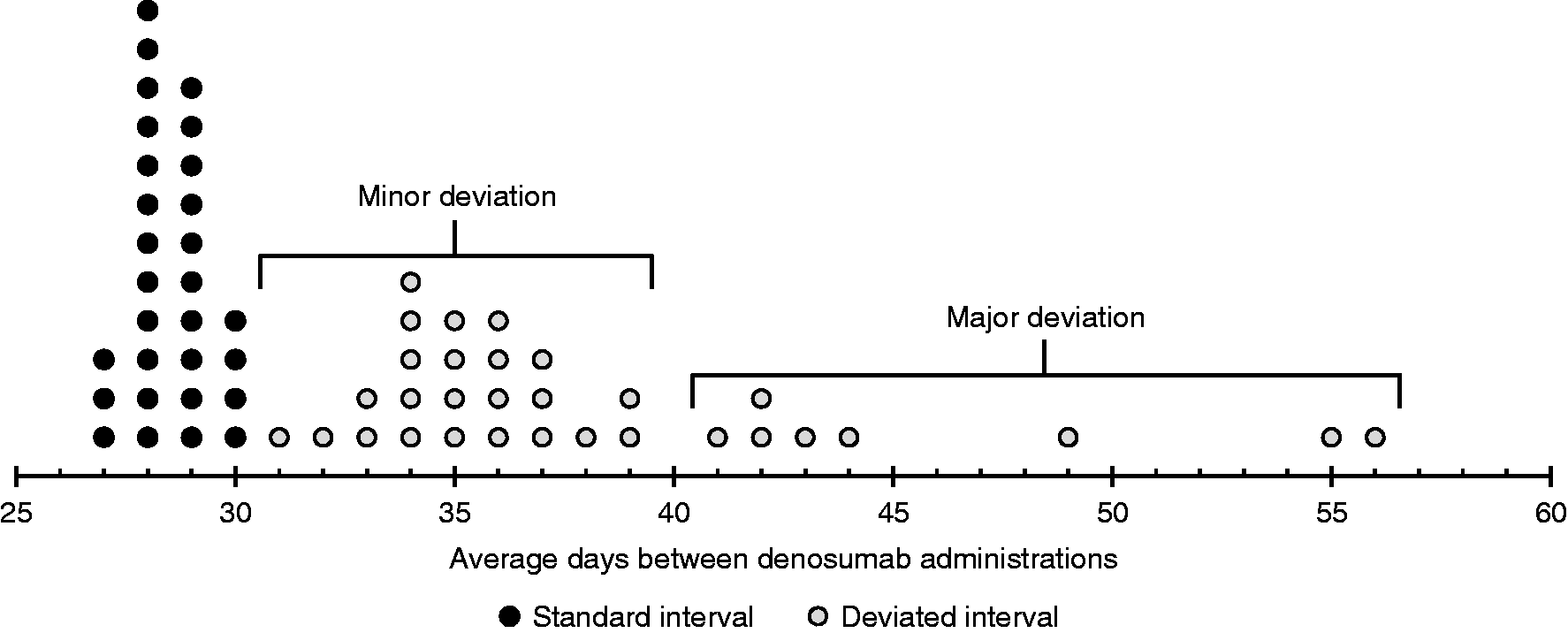
The primary outcome was the percentage of patients developing a skeletal-related event (SRE). For the purposes of this analysis, the definition of a SRE was modified to facilitate retrospective review. Specifically, an SRE was defined as (1) confirmed or suspected spinal cord compression, (2) fracture from any cause or severity, (3) radiation to the bone, or (4) surgery to the bone. Secondary outcomes included evaluating the difference in the percentage of patients that developed each individual component that defines an SRE and hypercalcemia (serum calcium > 13 mg/dL). Safety endpoints included the occurrence of osteonecrosis of the jaw and hypocalcemia (serum calcium < 6). Information was gathered from clinical notes and radiographic reports in the electronic medical record utilizing a search tool to identify key words related to the primary and secondary outcomes.
Patients were randomly selected from a list of all administrations of denosumab within the institution during the study period. While the initially targeted patient population for this study was a total of 100 patients, data collection ceased when a clear statistically significant difference in primary outcome was noted after a review of 62 total patients. Descriptive statistics were used to describe baseline characteristics. Categorical data were assessed using the Fischer’s exact test (two tailed).
Results
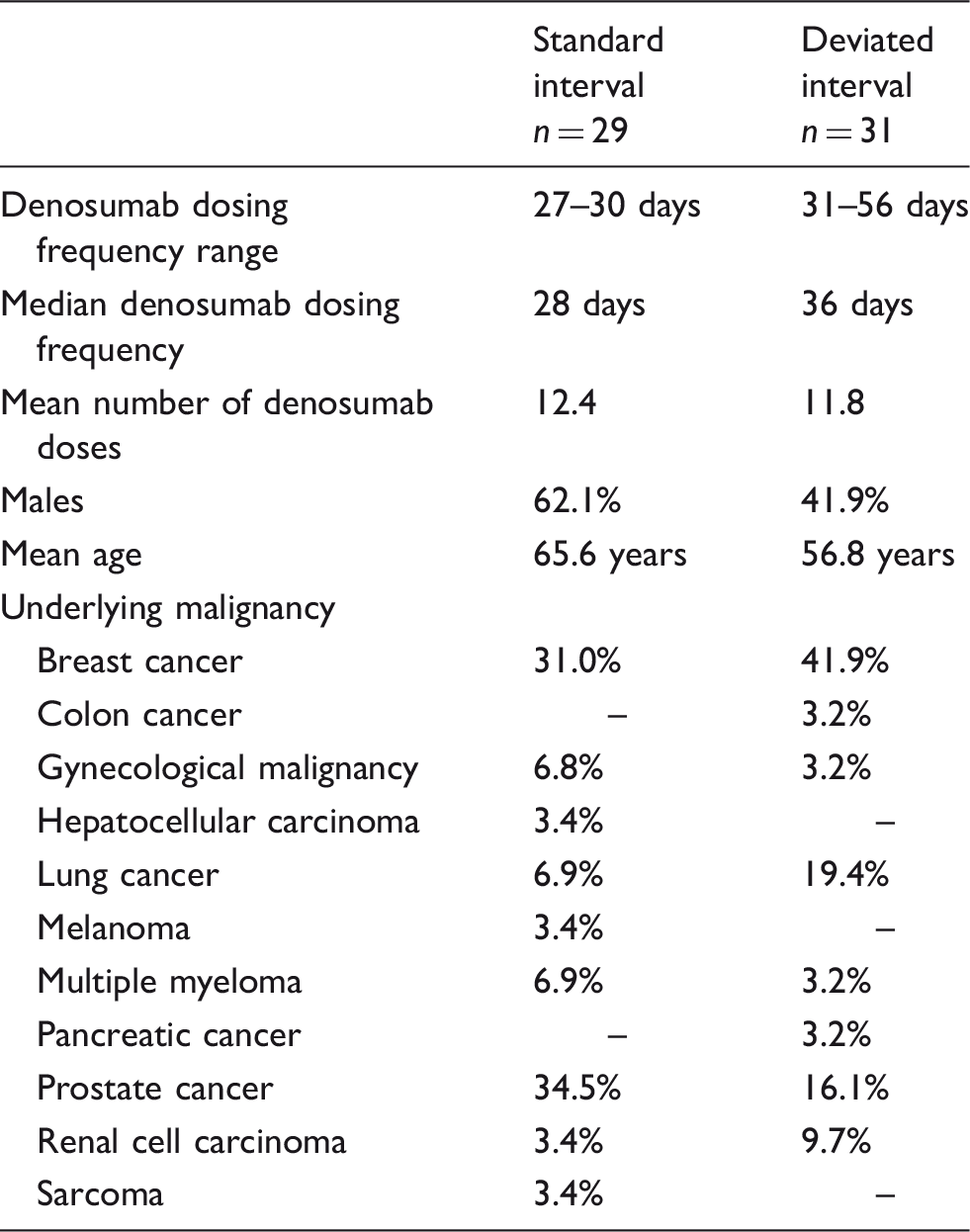
Demographic and clinical characteristics among patients in the standard and deviated interval groups.
Patients in the deviated interval cohort displayed a 61.3% incidence of SREs compared to 31.0% in the standard interval arm (p = 0.02). Review of the dose-deviated group indicated that the occurrence of SREs was not confined to patients with the most prolonged treatment intervals but rather well distributed throughout. Sub-group analysis demonstrated a numerically greater SRE frequency among the minor deviations compared to major deviation (65.2% vs 50.0%). When reviewing individual SRE, the deviated interval group displayed a trend toward a higher rate of events in all sub-groups except for requirement for surgery and hypercalcemia (Figure 2). Rate of surgery to the bone was virtually identical in each patient group and no patients in this study developed hypercalcemia.
Frequency of skeletal-related events among patients receiving standard and deviated dose frequency denosumab.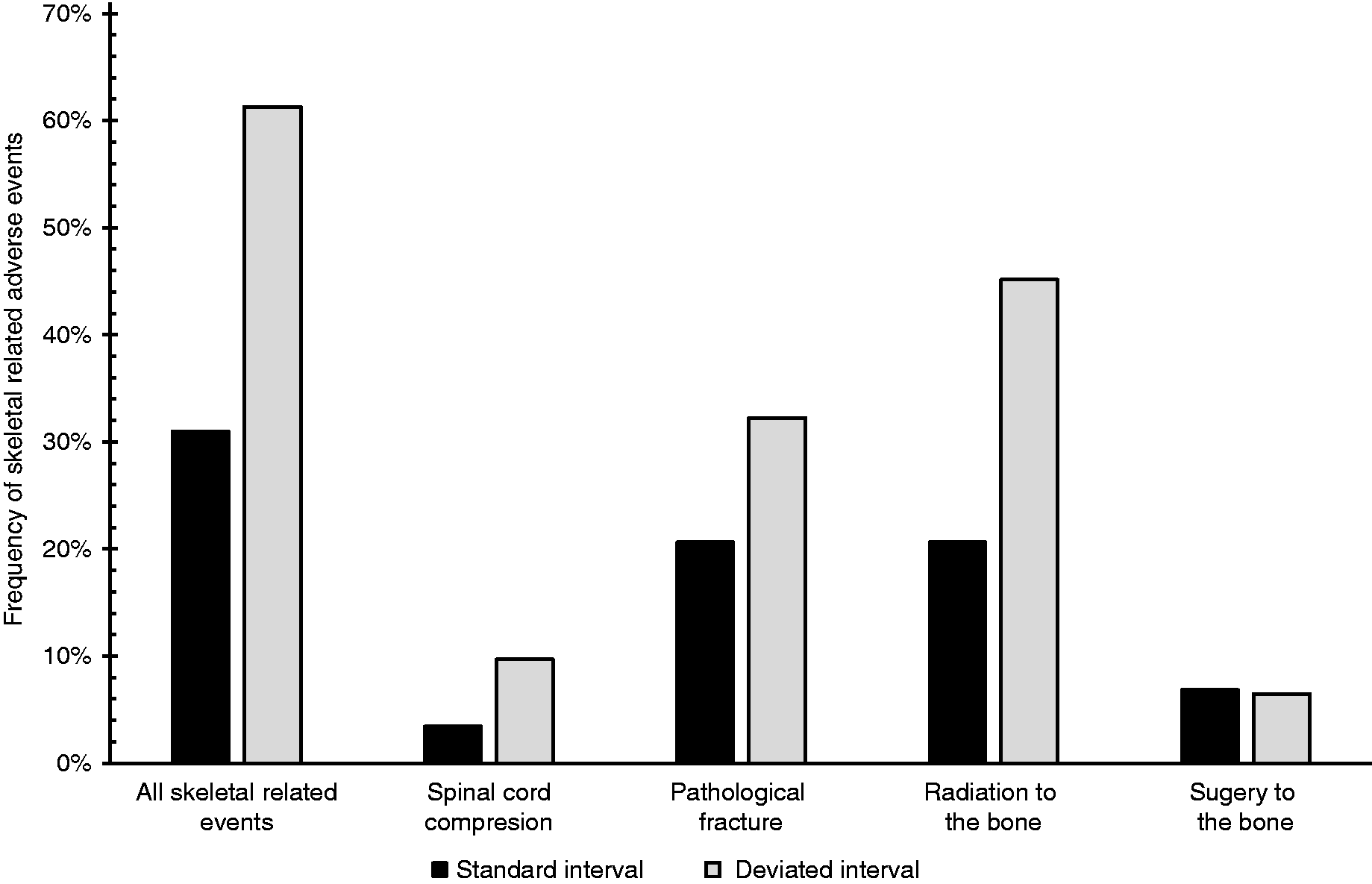
The rate of hypocalcemia was higher in the deviated interval group; however, this difference was not statistically significant (16.1% vs 6.9%, respectively). No patients in this study developed osteonecrosis of the jaw.
Discussion
The bone targeting medications denosumab and zoledronic acid are vital supportive care agents in patients with advanced malignancies affecting the bone. Despite the importance of treatment, logistical and financial obstacles hinder the ability to maintain long-term adherence. Although the efficacy of zoledronic acid is preserved in breast cancer patients with an extended dosing interval, the results of this preliminary analysis suggest that the same may not hold true for denosumab. 8
The findings from this study were rather unexpected particularly considering that denosumab demonstrates a substantially longer half-life in comparison to zoledronic acid.9,10 Given this favorable pharmacokinetic profile, it was postulated prior to undergoing this research that denosumab would be ideal for extended interval dosing. Two critical differences between the design of the ZOOM trial and the population studied in this analysis may in part explain the lack of demonstrable efficacy of extended interval dosing with denosumab. First, the ZOOM trial included a full year of monthly dosing prior to reducing dosing frequency. Second, the ZOOM study was restricted to breast cancer patients. It is certainly conceivable that efficacy of a less frequent dosing strategy may necessitate an initial period of conventional dosing and/or may be limited to certain cancer types. Unfortunately, the limits of the retrospective study design and sample size preclude assessment of alternative dosing regimens or the impact of tumor pathology.
The non-randomized methodology of patient selection and retrospective nature of this review present additional hindrance on the analysis of this study. Patients included in the deviated interval group were inherently non-compliant with bone targeting therapy. It is possible that these patients simultaneously lacked adherence to antineoplastic therapy and thus at least a portion of the difference between cohorts may have been a reflection of inadequate treatment. An imbalance between patient groups provides additional limitations of interpreting the outcomes. The standard interval group was highly represented by prostate cancer, which tends to progress in indolent fashion, compared to the deviated interval group which included higher percentages of the generally more aggressive breast and lung cancers. The extent to which this difference impacted outcomes is uncertain; however, this unbalance clearly could have favored the standard interval arm. A prospective randomized controlled trial would ultimately be necessary to eliminate the potential impact of these concerns.
The higher than expected incidence of SREs seen in both groups is likely a reflection of the retrospective nature of the study and the more inclusive definition of SREs for this analysis. Such an adaptation was necessary due to the dependence on progress notes and radiographic reports – which tend to have varying degrees of quality and clarity – to determine clinical outcomes.
This research successfully accomplished the intended purpose of generating preliminary data regarding the feasibility of extending the dosing interval of denosumab for prevention of SRE. Notwithstanding the smaller than anticipated sample size, a significant increase in SREs among patients receiving denosumab less often than the standard frequency was demonstrated. The identification of this difference with only a modest deviation beyond standard dosing is discouraging for the feasibility of extending denosumab dosing interval. It is, however, important to exercise caution in the interpretation of these results given the aforementioned limitations. It is not unreasonable to project that if the confounding variables are eliminated within the confines of a more robust study design, a different result may have been realized. Nonetheless, particularly given the absence of any contradictory data, it appears prudent at this time to make every reasonable effort to maintain standard denosumab treatment frequency in order to attain optimum benefits.
Conclusion
Non-adherence with the standard denosumab dosing schedule demonstrated an increased risk of experiencing an SRE. Preservation of denosumab dose density appears imperative to maintain efficacy and as such extending the dosing interval should be discouraged. For patients unable to comply with the monthly dosing regimen for denosumab, zoledronic acid may prove a prudent alternative.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Kettle is on a speaker board for Merck and Genentech and is an advisor for Pfizer, Sandoz, Amgen, and Genentech.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.