
Abstract
Background
To prevent occupational exposure of hospital staff to cytostatics, a mandatory national guideline describing a set of safety measures was issued in the Netherlands in 2004. The guideline includes, among other directives, obligatory annual wipe testing to assess the efficacy of the local cleaning protocol. Full implementation of this guideline was executed in all Dutch hospital pharmacies over the next couple of years.
Objective
We aimed to investigate the effect of the national guideline on contamination levels, and specifically on the phenomenon of carry-over of traces of antineoplastic drugs through contact with surfaces, since this is a potential route of exposure.
Methods
From a database including wipe sample results of 9 hospitals over 10 years, we extracted all sampled locations in the compounding areas as well as in adjacent or bypass rooms and locks. We considered only the locations outside safety cabinets or isolators, to examine the containment of contamination and to address possible routes of how a contamination can migrate through the preparation and distribution areas. The dataset consisted of 2647 wipe samples.
Results
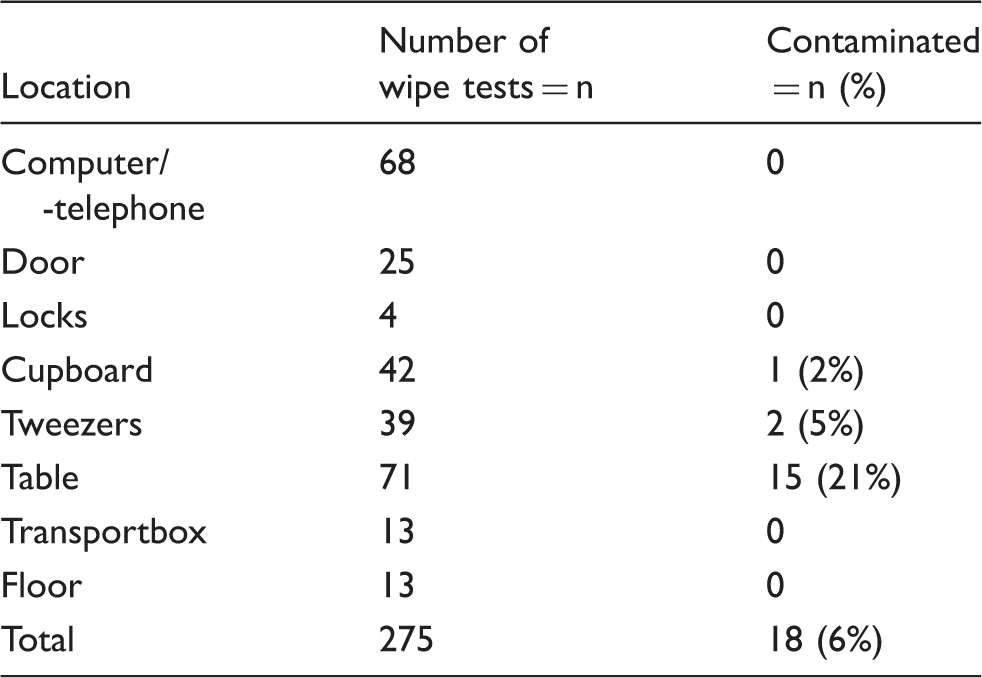
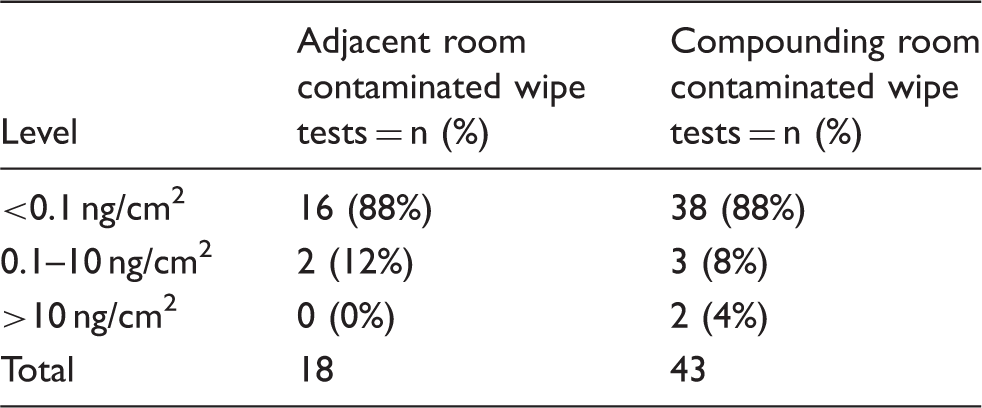
In adjacent rooms, 18 out of 275 wipe samples were contaminated (6%). Inside the compounding room, the extracted locations away from the safety workbench showed a positive percentage for contamination of 13% (39 out of 297). When stratifying the data to sample year, it was shown that contaminations outside the preparation room were no longer detectable after 2008.
Conclusion
With this study, we show that implementation of a set of guidelines on safety measures can prevent spreading of cytostatic traces from the compounding area in hospital pharmacies.
Introduction
Occupational exposure to cytostatics has been shown to cause adverse health effects in hospital staff. The first reports of possible harm from long-term exposure in health care workers stem from the 1970s.1,2 Since then, multiple studies have proven toxic effects on reproduction,3–6 and although carcinogenicity has never been demonstrated undisputedly by epidemiological studies, repeated identification of mutagenic activity in urine of health care workers7,8 as well as observed DNA damage in blood and other cells of hospital staff9,10 makes them suspect for oncogenicity as well. Exposure can occur through four distinct pathways: via oral ingestion, ocular exposure, inhalation or through skin contact. The first two of these routes are easily manageable by wearing adequate protective clothing and implementing hygienic measures during work routine. Inhalation can be minimised by working in a biological safety cabinet or isolator and by using (semi-)closed transfer systems instead of needles. This leaves the dermal route, which is generally considered to be the major exposure pathway. This assumption has been substantiated by the demonstration of high levels of contamination on gloves worn during preparation and administration of cytostatic drugs11–13 as well as by studies demonstrating the ability of cytotoxic drugs to permeate gloves. 14 Monitoring the potential for skin contact can be performed by taking wipe samples of exposed surfaces.
The exact relationship between occupational exposure to small levels of cytostatics and harmful effects is very difficult to quantify. Moreover, the extrapolation of certain levels of surface contamination to harmful effects in humans is even harder, because different cytostatic drugs have different physical properties, so skin permeation will vary, as will the potential of these drugs to evaporate from or be swiped of surfaces of different materials. Studies into the relationship between surface contamination levels and internal exposure have provided very conflicting results.15–17 Hence, with the current scientific knowledge, it is not possible to set a threshold level of exposure that will certainly cause no adverse effects. Therefore, employers should aim for the lowest level of contamination that is reasonably achievable (ALARA principle). 18
To standardize the different efforts put in reducing the exposure to antineoplastic agents, a Dutch national guideline was issued in 2004,
19
describing mandatory safety measures for the handling of cytostatics in hospitals. For the hospital pharmacy, these guidelines included: (a) the use of a separate, dedicated room to compound cytostatics with entry through a lock (b) recirculation of air from the compounding room should be zero % (c) preparation must be performed in a safety cabinet or isolator with negative air pressure (d) use of (semi)closed needle-free drug transfer systems (two types of devices are allowed under this regulation: closed-system transfer devices or spikes, which are vented, needle-free devices) the use of fully protective clothing including footwear, which should be changed at least daily (f) unpacking of cytostatic vials should take place in a dedicated area with hand protection (g) before transport compounded cytostatics should be packaged in a double layer of protective shields (h) use of a daily cleaning protocol with a dedicated set of cleaning equipment (i) cleaning must start from the cleanest spot working towards the dirtiest spot (j) performance of annual wipe tests to check the efficacy of the cleaning protocol. Implementation of these guidelines in all hospital pharmacies took place in the following years.
20
Concurrently, another national guideline was developed on safe compounding of hazardous substances, the GMP-H4.
21
This guideline includes directions on premises, equipment and procedures not only for cytotoxics, but also for radiopharmaceuticals and other CMR drugs. Because of these strict regulations, the cytostatic compounding areas in Dutch hospitals are now all outlined in a very similar fashion, a schematic representation of which is given in Figure 1.
Schematic representation of a cytostatics compounding area.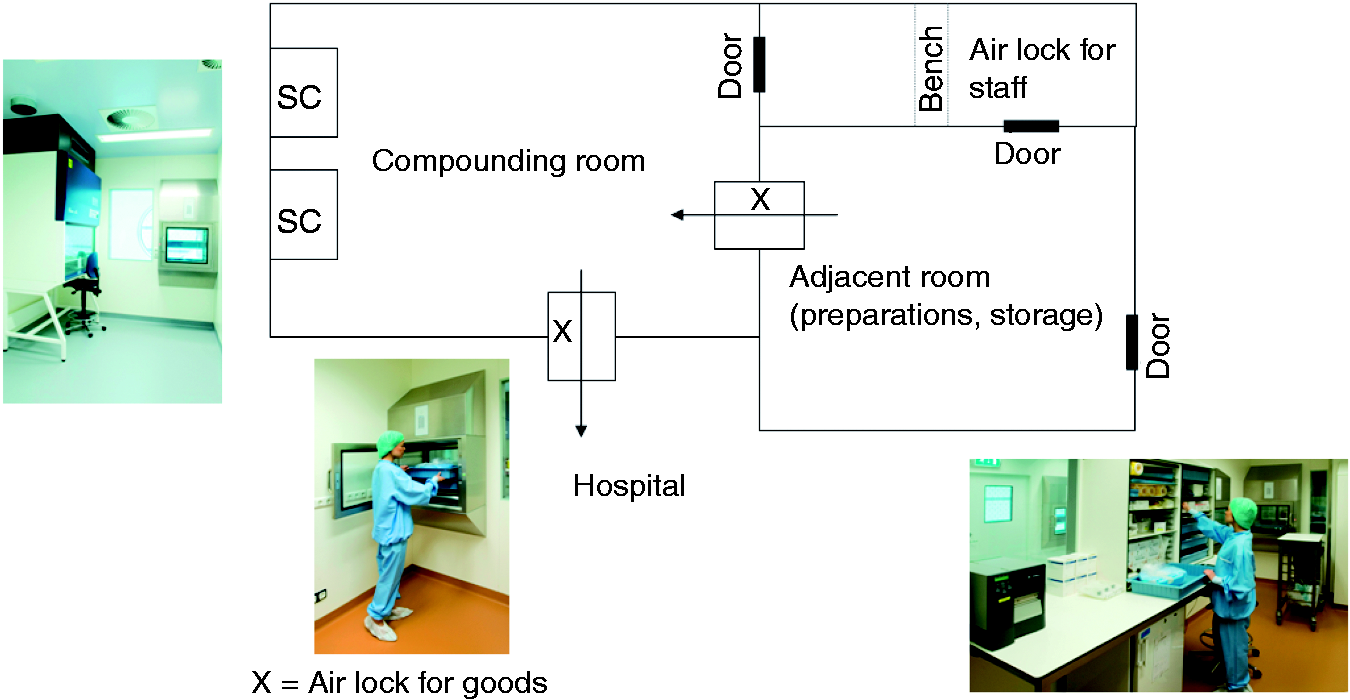
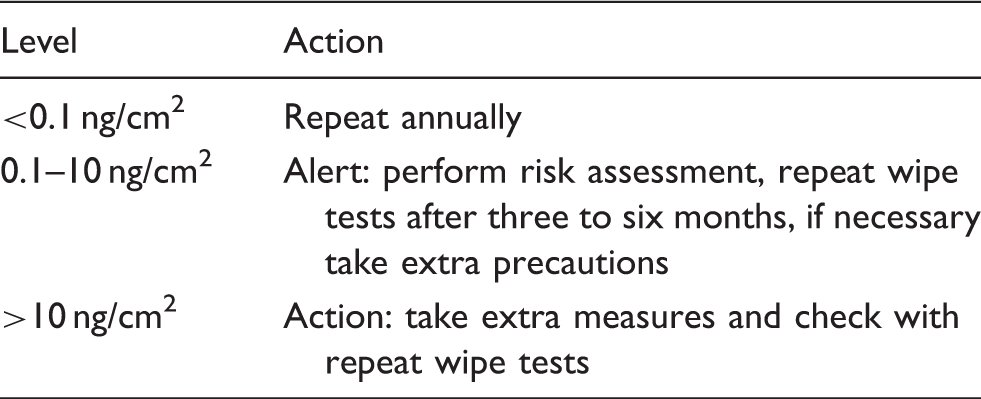
National consensus on alert and action levels for cytostatics wipes test results. 22
The pharmacy staff in the cytostatics compounding area is wearing highly protective clothing. In theory, however, it is possible that traces of cytostatics are transferred to areas outside of the compounding room and then spread to parts of the hospital or the hospital pharmacy where the staff is less protected, for example to storage areas or non-oncology wards. Contamination of surfaces or staff that are not in direct contact with chemotherapy has been described previously, for example contamination of transport boxes,26,27 corridors, 28 cleaning stations, and utility rooms. 29 In addition, hand sample wipes of staff working in storage areas, transport and administrative offices in both pharmacies as well as hospital wards have been found to be contaminated with antineoplastic drugs. 29 Such transfer of cytotoxic contamination could occur if traces of cytostatics stick to movable goods or gloves/footwear of compounding staff. To investigate this phenomenon, that is called carry-over, we performed a retrospective analysis of wipe test results with a specific focus on locations outside the production area.
Materials and methods
A dataset of wipe-tests from nine Dutch hospitals with results from the years 2001 to 2011 was developed and reviewed. All hospitals provided their results voluntarily.
The participating hospitals were representative of the Dutch hospital population: one tertiary cancer center was included as well as three university hospitals, four large teaching hospitals and one regional hospital. Wipe-sampling was performed after cleaning on a preferred surface of 10×10 cm. For non-flat locations such as door handles, the surface was estimated by the local hospital pharmacist. The choice of location of wipe sampling was left to the individual hospitals. All pharmacies used spikes as compounding devices. Cleaning in all hospital pharmacies was performed daily, by trained cleaning staff with a detergent followed by disinfection by either alcohol or sodium hypochloride solution. Training of the cleaning staff encompassed both clean room knowledge as well as hazardous substance knowledge. Cleaning was performed in the direction from the cleanest spot to the most dirty spot with dedicated cleaning materials for the cytostatic compounding area.
Measured cytostatics were 5-fluorouracil, iphosphamide, cyclophosphamide, methotrexate and platinum-derivatives. All measurements were made using validated laboratory chromatography methods (or atomic absorption spectrometry in the case of platinum wipe tests). The analysis of 5-fluorouracil, cyclophosphamide and iphosphamide was performed with gas chromatography coupled to mass spectroscopy (5890 series II GC, 5971 A MSD, Hewlett Packard). Samples were pre-treated on an ultrasonic bath for 90 min with 45 ml of sodiumhydroxide (0.03 M) per wipe sample. Subsequently, extraction was performed with 5 ml of ethylacetate, and derivatisation was executed with trifluoroacetic acid (50 µl per 50 µl of extract). Separation was performed with an HP-5 column (12 m, 0.22 mm internal diameter, 0.33 µm film). Samples were injected by splitless injection at a temperature of 225℃) The carrier gas was helium (0.8 ml/min) and the temperature over the column had a fixed gradient: 1 min 100℃, 10℃/min up to 220℃ followed by 20℃/min up to 290℃, (total runtime of 16.5 min). Detection took place at 280℃ with an electron ionisation detector by selected ion monitoring. Identification was performed with masses of 150, 212 and 307 and 309. All substances were of reagent grade. The analytical method was developed and validated in the TweeSteden Hospital in Tilburg. The measurements of the platinum samples and the methotrexate samples were performed as published previously.26,30
The lower levels of quantification were: 0.01 ng/cm2 for iphosphamide, 0.0013 ng/cm2 for cyclophosphamide, 0.01 ng/cm2 for 5-fluorouracil, 0.06 ng/cm2 for methotrexate and 0.25 ng/cm2 for platinum.
In total, a number of 2647 wipe test results were included in the dataset. Results were stratified according to location, severity (according to the national consensus alert and action levels, Table 1) and year. With reference to carry-over, we analysed all wipe sample locations outside the work benches in an attempt to map how contaminations can spread from the compounding area to other locations.
Results
Contamination in adjacent (preparatory or ante) rooms.
Contamination in compounding rooms.
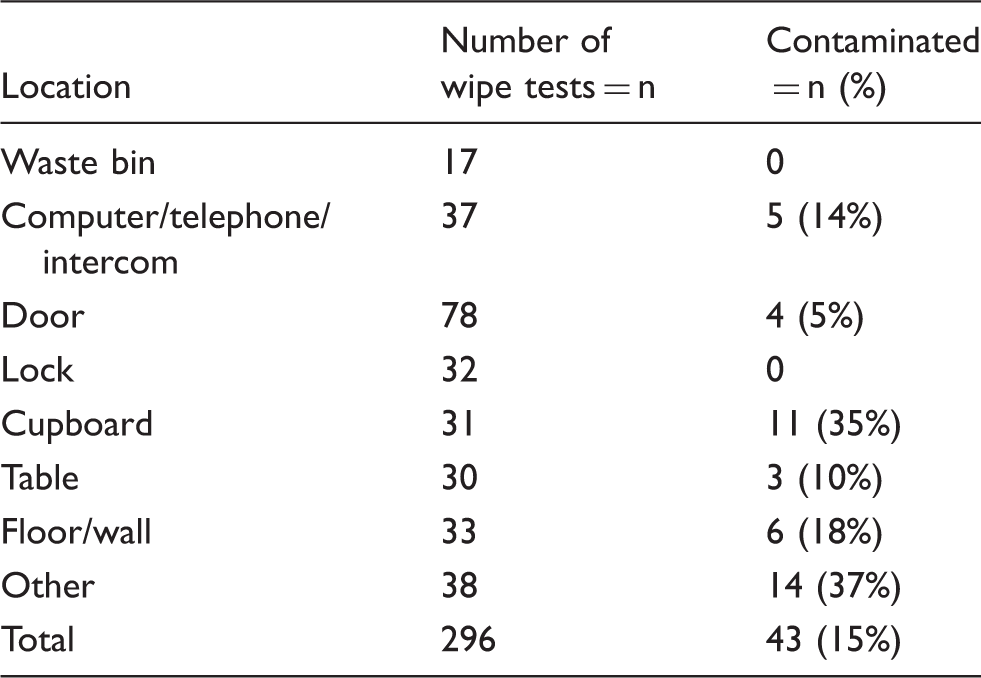
Note: Only locations outside the safety workbench or isolator are included.
Severity of observed contamination.
Contamination in adjacent (or preparatory) rooms by year.
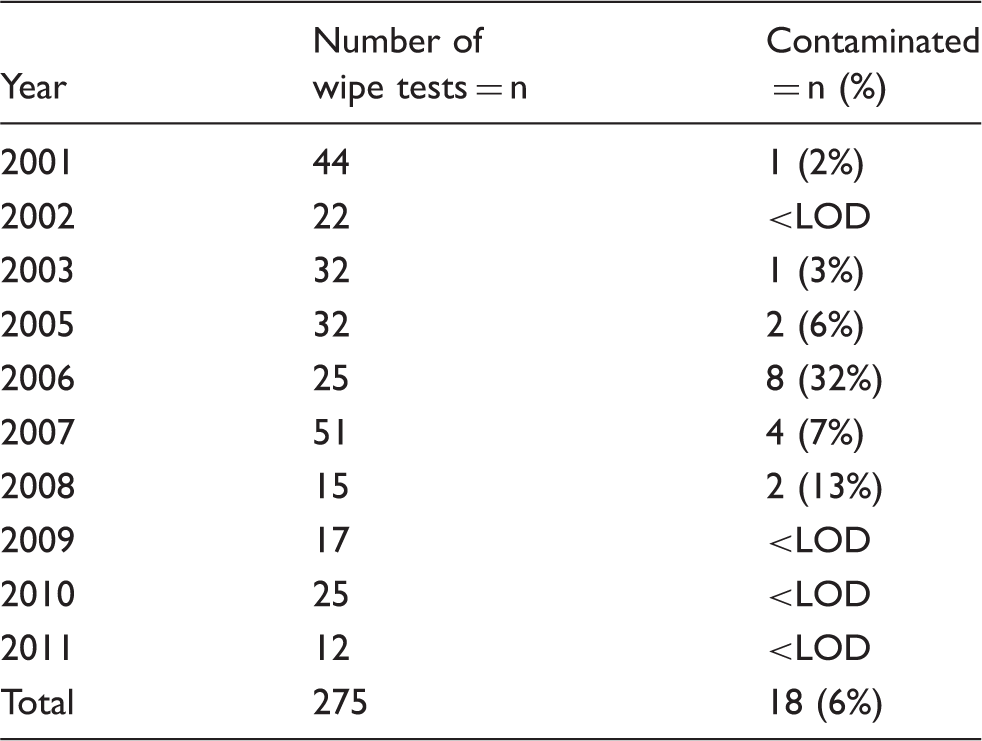
LOD: lower limit of detection.
Discussion
Occupational exposure of health care workers to cytotoxic agents remains a matter of concern. As long as no definite cut-off values for safe levels of exposure are established, employers should strive to keep exposure as low as reasonably achievable (ALARA principle). For staff handling cytotoxic drugs, strict guidelines on personal protection and working principles have been established both in Europe as well as in North-America.18,31 Previous studies have shown that traces of cytotoxics can migrate through health care institutions, which could lead to exposure of employees who are not directly involved in drug preparation or administration.27,32–35 This poses a potential hazard, for these employees are generally less protected by protective clothing. Hence, it is pivotal to contain cytotoxic contamination to the direct sources and prevent spreading.
The findings of our study support the conclusion that, provided that the present strict working procedures are maintained, contamination of cytostatics can be contained to the production areas. 20 This is a positive outcome for working conditions in Dutch Hospital pharmacies. However, some weaknesses in the methodology should be taken into consideration. Firstly, participation of hospitals was voluntary. Hence, it is possible that hospital pharmacies not adhering as strictly to the guidelines, chose not to participate. In addition, only five cytostatics were tested. It is conceivable that other cytostatics were not contained to the production area. However, the panel of cytostatics is representative of the most commonly prepared drugs and has been used as model drugs extensively in other studies.32,36,37 Furthermore, wipe sampling was performed by individual staff members from the participating hospitals, so variability in wipe sampling efficacy could have occurred. Each hospital did follow the wipe sampling protocol though, which is a part of the national guideline. As each hospital took its own wipe-samples, we could not establish the wipe sample efficiency, and hence had to presume 100% recovery. This has been done in previous studies as well, but it is possible that the actual drug amounts are underestimated by the reported values. 33
Since a complete set of guidelines was issued at once in 2004, 19 it is not possible to distinguish which individual measure contributed most to the observed decline in carry-over. Here, our results conflict with a previous study from the Czech Republic, where introduction of novel measures to reduce contamination was shown to have limited effect in the hospital pharmacy. However, implementation of cleaning from the cleanest areas in the direction of the most contaminated area (the safety cabinet or isolator) – as is done in the Netherlands – might have had a small effect in the Czech study as well, as some reduction in contamination of floors and refrigerators was noted. 37 Finally, our data set only included wipe-samples taken after cleaning. This is in line with the national guideline, which only requires wipe sampling to asses the effectiveness of cleaning. Hence, spreading of cytotoxics could have occurred during preparation. However, persistence of such surface contamination seems highly unlikely, as we found no positive samples in all years after 2008 outside of the preparation room, and the number of different sampling locations was quite large.
The present study is the first to evaluate wipe samples over a long period of time in a panel of representative hospitals. To our knowledge, this is the first large scale investigation of the efficacy of containment of cytostatics to the dedicated cytotoxic compounding rooms. The decrease in positive wipe samples after 2004 is striking, especially since the turnover of cytostatics increased. Previous studies have shown conflicting results on this issue: a Swedish and a German study both suggested a correlation between contamination levels and drug throughput,27,28 whereas reports from Italy, the Czech republic and Germany failed to establish such a relationship.34,38,39 The present Dutch results confirm that it is possible to handle increasing amounts of cytostatics without increasing the level of surface contamination.
The phenomenon of containment has been addressed in previous studies. Two consecutive Canadian trials found surface contamination on locations outside of the compounding room, including on surfaces that hospital staff touches with bare hands. 33 In addition, positive wipe samples of employees not directly involved in chemotherapy preparation or administration were repeatedly identified. 29 A similar trend of positive wipe samples in areas in the pharmacy but further away from the compounding site was reported in a trial in three US cancer hospitals. 32 It should be noted that the lay-out of the hospital pharmacies differs in Northern America from Europe. In the above-mentioned studies, the cytostatics were not always prepared in isolated preparation rooms, and transport was not performed in dedicated chemo transfer boxes. This could be an explanation for the difference between these results and ours. The fact that contamination in the compounding room is higher than in adjacent areas is in line with previous publications from the Czech republic, 34 but contrary to both a Portuguese and a German report, where the anterooms used for storage and checking of drugs showed many positive wipe samples.27,35 Possibly, cleaning of anterooms or preparatory rooms in these countries is less intensified than in the cleanroom, thereby allowing contamination, for example from the outside of vials, to persist.
A limitation to our study is that it only included the hospital pharmacies. Carry-over of cytostatics to other areas of the hospital could also occur from the oncology wards or outpatient clinics. These areas have shown higher levels of contamination when compared to the pharmacies in multiple reports.28,29,32 Hence, future studies on containment or carry-over should focus on clinical departments of the hospital and could also be expanded to measuring carry-over effects before cleaning.
Conclusions
In the present survey, we demonstrate that it is possible to prevent carry-over of cytostatic contamination by implementing national guidelines. Four years after the working guidelines were issued, cytostatic contamination outside of preparation rooms in the pharmacy was abolished.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article