
Abstract
Objective
To review the literature discussing QT prolongation associated with the use of tamoxifen in order to evaluate the clinical significance.
Data sources
A search of PubMed (1946 to 2017), MEDLINE (1946 to 2017) and EMBASE (1947 to 2017) was performed using a combination of the following search terms: tamoxifen, estrogen antagonist, selective estrogen receptor modulator, QT prolongation, QT interval, long QT syndrome and torsades de pointes. All searches were limited to human subjects. Reference lists of the literature found were also reviewed but did not reveal any further articles.
Study selection
Articles reviewed were relating to humans only and included clinical trials and case reports that mentioned QT prolongation in association with the use of tamoxifen.
Data synthesis
It can be common for patients on tamoxifen to also be on a number of different medications being used to treat comorbid medical conditions. Such combinations of medications increase the potential risk for drug interactions, such as drug-induced QT prolongation. Tamoxifen is often flagged by tertiary drug information sources as a drug with indeterminate effects on the QT interval. However, the risk may be elevated when combined with other QT-prolonging agents. A total of five publications were identified, including two phase I clinical trials and three case reports, which discussed the association between tamoxifen and QT prolongation.
Conclusions
Tertiary drug information sources identify tamoxifen as an agent that may cause QT prolongation when used in combination with other QT-prolonging agents. However, based on the limited number of published reports found, it would suggest that the use of tamoxifen concurrently with other agents known to prolong the QT interval is likely to be of low risk for causing a clinically significant QT-prolonging event, especially at a dose of 20 mg daily.
Background
Tamoxifen, an estrogen receptor antagonist, is commonly prescribed for breast cancer patients with estrogen and/or progesterone receptor-positive disease. 1 While tamoxifen is most frequently utilized in breast cancer at a dose of 20 mg daily, it has also shown efficacy in the treatment of brain tumours, melanoma, soft tissue sarcomas, endometrial cancer and pancreatic cancer, at varying doses.2,3 The duration of therapy when used in breast cancer typically continues for a minimum of five years. 1 However, many physicians are now opting to use tamoxifen for 10 years of adjuvant treatment, after results of the ATLAS trial demonstrated that 10 years of therapy provided further reduction in breast cancer recurrence and mortality compared to five years of therapy. 4 Given the long duration of treatment, it is not uncommon for patients to be placed on a number of medications to treat comorbid medical conditions while they are on tamoxifen. As the number of drugs that a patient is taking increases, clinicians should be increasingly concerned about the potential for drug interactions. One interaction of particular interest is drug-induced QT prolongation, which is documented as a potential side effect of many drugs and drug combinations. Many clinicians are bombarded on a daily basis with drug interactions that are flagged as potentially leading to QT prolongation, which can often make it difficult to distinguish which identified interactions are truly clinically relevant. Tertiary drug information sources, such as Lexi-Comp® and Micromedex®, identify tamoxifen as an agent that has uncertain effects on the QT interval, but that it may cause prolongation when used with other QT-prolonging agents.5,6
The risk of developing a prolonged QT interval is elevated in female patients and also increases with age. Other risk factors include low potassium (<3.5 mEq/L), heart failure or previous myocardial infarction, history of bradycardia and the use of multiple QT-prolonging drugs concurrently.7,8 The QT interval of a patient can vary according to heart rate. Thus, in order to be able to compare QT intervals, the corrected QT interval (QTc) is often used instead. 9 The American Heart Association and the American College of Cardiology Foundation define a prolonged QTc as > 470 ms for males and >480 ms for females. However, they do note that some software systems used to measure electrocardiograms (ECGs) identify interval prolongation at a lower threshold of a QTc interval > 440 ms in men and > 460 ms in females. 10
A literature review was performed in hopes of better defining the extent and clinical significance of QT prolongation associated with tamoxifen use.
Literature review
Summary of literature.
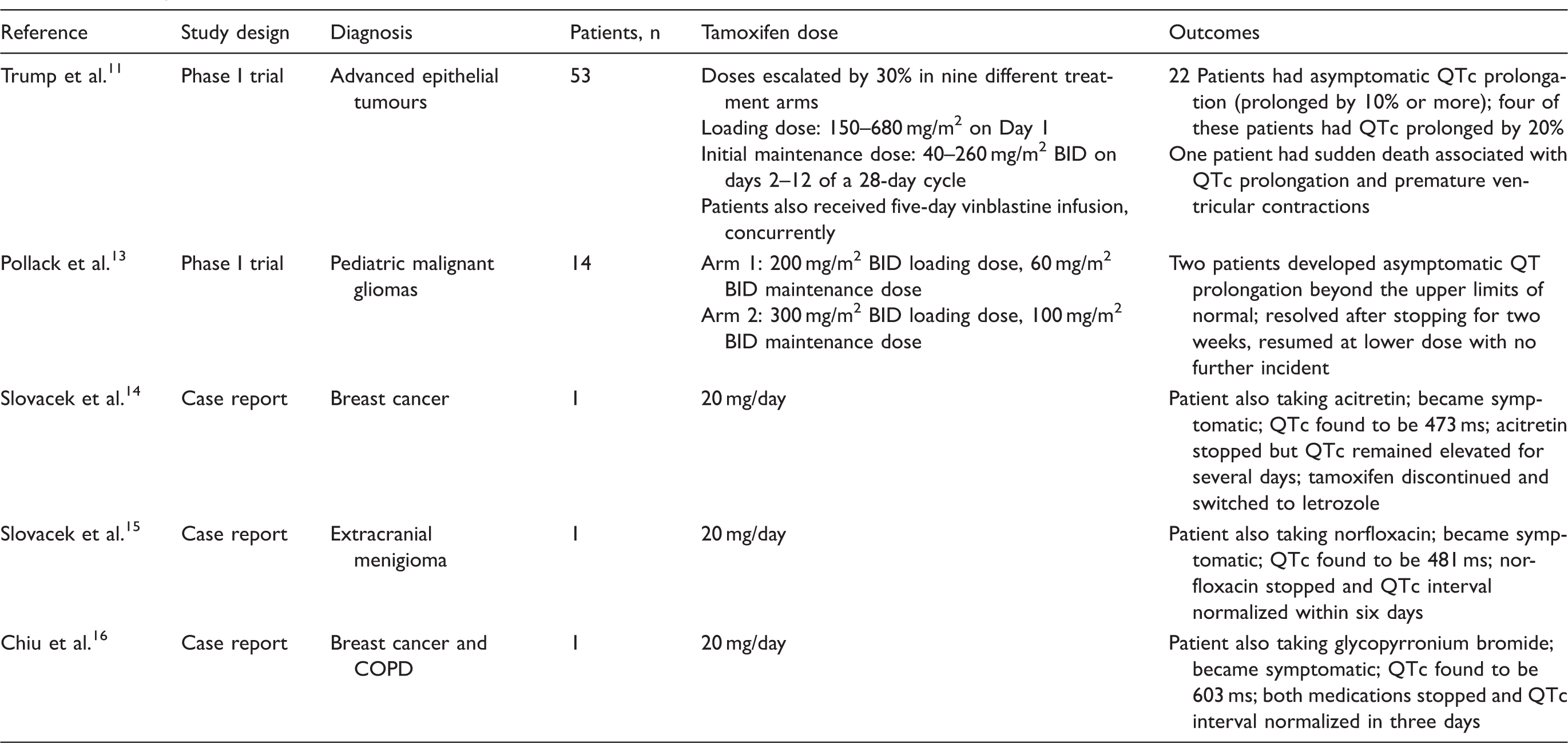
COPD: chronic obstructive pulmonary disease; QTc: corrected QT interval; BID: twice daily.
Trump et al. 11 published a phase I trial investigating the use of high-dose tamoxifen in combination with vinblastine in the treatment of advanced epithelial tumours. In this article, the authors discuss the potential for tamoxifen to prolong the QT interval. 11 A total of 53 patients were included in the study. Patients were separated into one of nine different dose escalation treatment arms. The starting dose of tamoxifen, which was administered to group one, was a loading dose of 150 mg/m2 on day 1 followed by a maintenance dose of 40 mg/m2 given twice daily on days 2–13 of a 28-day cycle. Each of the subsequent groups received tamoxifen at a dose that had been increased by 30% above the previous group, with a maximum allowable loading dose of tamoxifen 680 mg/m2 and a maximum allowable maintenance dose of 260 mg/m2 twice daily. Patients were evaluated to establish the maximum tolerated dose, which was defined as the dose that caused grade 3 toxicity, according to the National Cancer Institute Common Toxicity Criteria, in more than two of six patients in a dosing group. Patients also received a five-day continuous infusion of vinblastine 1.5 mg/m2 on days 9–13. Of note, while vinblastine has been implicated in causing myocardial ischemia, it has not been shown to cause QT prolongation. 12 During the course of therapy, one patient who was treated with 80 mg/m2 of tamoxifen twice daily died suddenly after receiving 10 days of treatment. The investigators retrospectively reviewed the patient’s ECG that was performed on day 8, which showed a prolonged QT interval and premature ventricular contractions. After this incident, all patients subsequently enrolled in the study had an ECG performed prior to starting therapy, which was repeated again on day 8 of treatment. Of the 43 patients who had baseline and day 8 ECGs performed, 22 of the patients had an asymptomatic prolongation of the QTc interval by 10% or more, in which four of the patients had their QTc interval increase by 20%. However, none of these incidents developed into clinically significant events. There was no record of concomitant medications used during the trial that may have increased the risk of QT prolongation. 11
The second phase I study that reported a relationship between tamoxifen and QT prolongation was published by Pollack et al. 13 and investigated the use of high-dose tamoxifen in children with treatment refractory malignant gliomas. A total of 14 children aged 3–18 were treated with tamoxifen in two different treatment arms. The first treatment arm received a loading dose of 200 mg/m2 twice daily on day 1, followed by a maintenance dose of 60 mg/m2 twice daily. The second treatment arm received a loading dose of 300 mg/m2 twice daily on day 1 followed by a maintenance dose of 100 mg/m2 twice daily. Based on the reports of QT prolongation with high-dose tamoxifen noted by Trump et al., a baseline ECG was obtained in all patients prior to starting therapy, and repeated at weeks 1, 4 and 12. Two of the patients taking 100 mg/m2 of tamoxifen had an asymptomatic prolongation of the QT interval beyond the upper limits of normal. As a result, the two patients stopped taking tamoxifen for two weeks and then resumed treatment at a lower dose level with no further incident. The data on any other medications administered during the trial was unavailable. 13
Slovacek et al.14,15 published two case reports out of the Czech Republic linking tamoxifen and QT prolongation. The first case report involved a 56-year-old female patient with estrogen/progesterone receptor-positive, HER-2-negative breast cancer. 14 She underwent a partial mastectomy and then received adjuvant tamoxifen 20 mg daily with concurrent radiation therapy. During treatment with tamoxifen, the patient was placed on oral acitretin 30 mg daily for the duration of radiation, to prevent skin reactions associated with her previous diagnosis of Darier’s disease. Acitretin is not known to be associated with QT prolongation; however, it does inhibit CYP 3A4, an enzyme used to metabolize tamoxifen. After three weeks of therapy with tamoxifen and acitretin, the patient developed sudden fatigue, dizziness, orthostatic hypotension and pressure behind the sternum. Results of an ECG demonstrated prolongation of the QT interval (QTc, 473 ms). Electrolytes and thyroid-stimulating hormone (TSH) were all within normal range and all myocardial enzymes were negative. Vitamin A serum levels were measured to rule out toxicity associated with acitretin and despite levels being normal, acitretin therapy was stopped. The following day after discontinuing acitretin, the patient’s symptoms resolved; however, the QT interval remained elevated for approximately three weeks (QTc, 459 ms). As a result, the patient discontinued tamoxifen and started letrozole 2.5 mg daily, and acitretin therapy was substituted with triamcinolone and dexamethasone used locally. The patient had no further recurrence of symptoms and her ECG normalized. 14
The second case report by Slovacek et al. involved an 83-year-old female patient being treated with tamoxifen 20 mg daily for an extracranial meningioma. 15 At the time of tamoxifen treatment, the patient was also completing a seven-day course of norfloxacin 400 mg twice daily for a urinary tract infection. After three days of using the two medications concurrently, the patient developed pressure behind her sternum and orthostatic hypotension. The ECG showed a prolonged QT interval (QTc, 481 ms). Once again, electrolytes and TSH were within normal range and all myocardial enzymes were negative. The patient was instructed to stop taking the norfloxacin, due to the potential for it to increase the QT interval. Her QT interval normalized within six days of discontinuing the norfloxacin. She remained on tamoxifen with no further incident. 15
Finally, Chiu et al. 16 published a case report which involved a 78-year-old female with a history of breast cancer and moderate chronic obstructive pulmonary disease (COPD), who presented to the emergency department. The patient’s medical history included invasive ductal carcinoma of the breast for which she underwent a total mastectomy and had been on tamoxifen 20 mg daily for nine months. She had also been taking glycopyrronium bromide 50 µg inhalation once daily for COPD for three months. In addition, the patient had received an intravenous vitamin infusion from a naturopathic clinic. The day after the infusion, the patient developed symptoms of dizziness, syncope and hypotension leading her to the emergency department. Once there, her symptoms resolved after receiving hydration. Further clinical investigations revealed that her electrolytes and TSH were normal; however, her QTc interval was elevated at 603 ms. The tamoxifen and glycopyrronium bromide were both stopped on admission as a result. By day 3 of hospital admission, the patient’s QTc interval had decreased to 442 ms and the patient was discharged. The investigators concluded that the cause of interval prolongation was likely due to the glycopyrronium bromide rather than the tamoxifen as the patient’s QTc interval normalized in a time frame consistent with the half-life of glycopyrronium (13–57 h) as compared to tamoxifen (8–14 days), and they attributed the syncope to orthostatic hypotension. 16
Discussion
Anti-estrogenic drugs have not generally been thought to cause a prolonged QT interval. In other drugs that prolong the QT interval, blockage of the human ether-a-go-go-related potassium ion channel (hERG K) has been shown to be critical in the development of interval prolongation. 17 The mechanism by which tamoxifen prolongs the QT interval has been studied in several different animal models in vitro. In the frog model, it was found that the use of tamoxifen has the potential to inhibit the hERG K channel; however, it appears to have less proarrhythmic potential compared to other hERG K channel inhibitors. 17 In the rabbit myocyte model, it was shown that more than 80% of the potassium channels are blocked when tamoxifen is used at therapeutic concentrations. However, the investigators found that this blockage had no effect on the action potential in rabbit cells. They hypothesized that this occurred because tamoxifen also blocked the L-type calcium channels, which leads to a shortening of the action potential. Therefore, by blocking the potassium channels, which prolongs the action potential, and the calcium channels, which shortens the action potential, the effects counteracted one another. 18 Tamoxifen has also been studied in rat models and was shown to inhibit potassium channels leading to prolonged action potentials contributing to the effects on the QT interval. 19 However, it is important to note that generalizability of these animal cell models to humans is limited, in part due to potential differences in the composition of potassium channels among the different species.
Slovacek et al.14,15 propose that the mechanism of prolonged QT interval is not likely due to the tamoxifen itself, but rather is related to a drug interaction that occurs when tamoxifen is used concurrently with other medications. Many different cytochrome P450 enzymes metabolize tamoxifen, one of which is the CYP 3A4 enzyme. There are a number of different drugs that have been shown to inhibit the CYP 3A4 enzyme needed to metabolize tamoxifen. When a drug that inhibits the CYP 3A4 enzyme is administered with tamoxifen, the result is decreased metabolism of tamoxifen leading to an increased concentration of tamoxifen in the plasma. Having higher concentrations of tamoxifen for a longer duration of time leads to a depression in the electrical cardiac impulses generated, which in turn could lead to prolongation of the QT interval.14,15 In addition to this, the two clinical trials citing QT prolongation as an adverse event seem to suggest that higher dose of tamoxifen (>80 mg/m2 given twice daily) may be more likely to produce QT prolongation than lower doses of tamoxifen.11,13
It appears to be possible for tamoxifen to prolong the QT interval as shown by the case reports and adverse events reported in the clinical trials discussed. However, details in these articles are restricted by the brief nature of the case reports. In addition, the two clinical trials presented discussed QT prolongation as an adverse event and were not the primary outcome of the trials. The trials were also limited by the small sample sizes and lack of information about other concurrent medications being used. While it is difficult to draw conclusions without high-level evidence, the limited number of published reports found suggests that the occurrence of QT prolongation with tamoxifen is quite rare.
Summary
Tamoxifen therapy is often used for several years, particularly in patients diagnosed with breast cancer. Therefore, it is not unusual for patients to be on a number of concurrent medications, which may also have a known risk of prolonging the QT interval. Many of these drug interactions identified by tertiary drug information sources have enough evidence of QT prolongation to warrant caution or even contraindication to using the two medications together. However, based on the limited number of reports found, it appears that concurrent use of tamoxifen with other agents that have the potential to prolong the QT interval is likely to be of low risk for a clinically significant event occurring, especially in the patient population on 20 mg of tamoxifen daily. If a drug interaction with tamoxifen is identified as potentially prolonging the QT interval, patients should be instructed of signs and symptoms to be aware of which may warrant further investigation. Signs and symptoms include dizziness or fainting episodes and any sudden onset of chest pain or pressure. In those patients who are prescribed high-dose tamoxifen, patients with an extensive cardiac history or those patients considered high risk for QT prolongation due to other risk factors, it may be pertinent to obtain a baseline ECG in order to have a comparator should the patient develop any signs or symptoms of QT prolongation in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.