
Abstract
5-fluorouracil and capecitabine are chemotherapeutic agents commonly used to treat solid malignancies. Increased susceptibility to 5-fluorouracil or capecitabine, caused by impaired clearance, dihydropyrimidine dehydrogenase deficiency, or other genetic mutations in the enzymes that metabolize 5-fluorouracil can lead to severe life-threatening toxicities and are typically manifested by an early onset of symptoms. We report and discuss the management and outcome of capecitabine toxicity with the recently FDA approved antidote, uridine triacetate (Vistogard), in a 57-year-old female breast cancer patient with homozygous dihydropyrimidine dehydrogenase deficiency who received treatment beyond the recommended 96 h window from the last dose of capecitabine.
Introduction
5-fluorouracil (5-FU) and capecitabine, an orally bioavailable prodrug of fluorouracil, are cytotoxic antimetabolites that are used to treat a variety of malignancies. Common toxicities of these agents are seen in rapidly dividing tissues, such as gastrointestinal mucosa and bone marrow.1,2 Severe toxicity can result from genetic variations, medication errors such as pump malfunction and dose miscalculations, or overdose suicide attempts.3–6 Over 80% of 5-FU is catabolized by the rate-limiting dihydropyrimidine dehydrogenase (DPD) enzyme in the liver.7–9 DPD deficiency syndrome, a familial disorder that results from the allelic mutations within the DPYD gene, is characterized by early onset and severe toxicities including mucositis, diarrhea, and myelosuppression, and rarely, neurologic deficits as well as cardiac toxicities.10,11 Genetic variation in the sequence of the DPD gene can lead to either partial loss of function, occurring in 3–5% of the population, or complete loss of enzyme activity, occurring in 0.2% of the population.12–15
Uridine triacetate, approved by FDA in December 2015, is indicated for those who exhibit early onset, severe, or life-threatening 5-FU or capecitabine toxicities, or those with an overdose within 96 h following the end of 5-FU or capecitabine administration.16,17 Uridine triacetate is deacetylated to provide circulating uridine to reduce incorporation of 5-fluorouridine-5′-triphosphate into RNA of hematopoietic cells and gastrointestinal mucosal cells, reducing 5-FU toxicity in normal tissues. Because it is highly lipophilic, uridine triacetate is quickly absorbed in the gut, rapidly deacetylating to deliver free uridine.1,18 Prior to uridine triacetate, there were no approved therapeutic options available for patients experiencing serious or life-threatening 5-FU toxicities or overdoses besides supportive care. The approval of uridine triacetate was based on data from two single-arm, multicenter open-label trials with 135 patients who received uridine triacetate for 5-FU or capecitabine overdose, or who had severe or life-threatening toxicities within 96 h following the end of 5-FU or capecitabine administration. 16 Of the 135 patients treated, 96% (n = 130) survived to day 30 or resumed chemotherapy prior to day 30, and 4% (n = 5) died. Four patients were treated outside the 96 h window, and 50% of these patients died. In the historical cohort, the clinical trial uridine triacetate recipients were compared to, consisting of patients overdosed by 5-FU infusion rate, 21 of 25 (84%) patients receiving solely supportive care died. The safety and efficacy of uridine triacetate initiated over 96 h following the end of 5-FU or capecitabine administration has not been established.1,16,19
Case report
The patient is a 57-year-old woman who presented with a rapidly growing right medial breast mass, measuring 3 cm × 2 cm, fixated to the chest wall. Excisional biopsy in February 2016 revealed an infiltrating ductal carcinoma that was estrogen receptor, progesterone receptor, and Her2/neu negative, Ki 67 unfavorable, and clinical stage of T4NX M0. Germline BRCA testing demonstrated no deleterious mutation, and computerized tomography of the chest, abdomen, pelvis, and bone scan revealed no systemic metastasis. Her past medical history was significant for hyperthyroidism, hyperlipidemia, asthma, and left-sided cerebrovascular accident with no apparent residual neurologic deficit. The patient was treated with neoadjuvant chemotherapy consisting of cyclophosphamide and docetaxel for five cycles, complicated by allergic reaction to docetaxel, and thus the planned sixth cycle was not given. At this point, her tumor had shrunk significantly in size, but was still palpable and had remained unchanged for her past two cycles of chemotherapy. After undergoing lumpectomy and sentinel node sampling in August 2016, surgical pathology revealed residual invasive ductal carcinoma, measuring 1.8 cm, with clear margins and a negative sentinel node biopsy for metastasis. Finally, adjuvant breast and chest wall irradiation was given and completed by November 2016.
Notably, a recent phase III study had demonstrated that capecitabine given as adjuvant chemotherapy in Her2/neu negative breast cancer patients with residual disease, following neoadjuvant chemotherapy and surgery, significantly reduced risk for disease recurrence, especially in triple negative patients. 20 The patient was therefore initiated on capecitabine at 850 mg/m2 twice daily as adjuvant therapy. After four days, capecitabine treatment was stopped due to nausea, vomiting, and skin rash. Six days after the last capecitabine dose, the patient presented to the emergency room at a local hospital with intractable nausea, oral mucositis, swollen face and lips, and a diffuse upper body skin rash. Complete blood counts, serum electrolytes, creatinine, and transaminases were normal upon presentation. She was briefly admitted and treated with antiemetics, steroids, and intravenous fluids. The swelling and rash improved, the nausea resolved, and the patient was discharged.
Nine days post her last dose of capecitabine, the patient was readmitted to another hospital with worsening mucositis, diarrhea, recurrent nausea, vomiting, and fever. On admission, she was noted to be pancytopenic, with a white blood cell count of 400 µl−1, hemoglobin 14.7 g/dl, and platelet count 16,000 µl−1 (Figure 1). She was thus started on empiric broad spectrum antibiotics and filgrastim for neutropenic fever. The patient’s DPD genotype was also tested upon admission. Uridine triacetate was not given, as the patient had taken her last dose of capecitabine over 96 h ago and did not fit the FDA-approved criteria for usage.
Patient recovery course after uridine triacetate administration.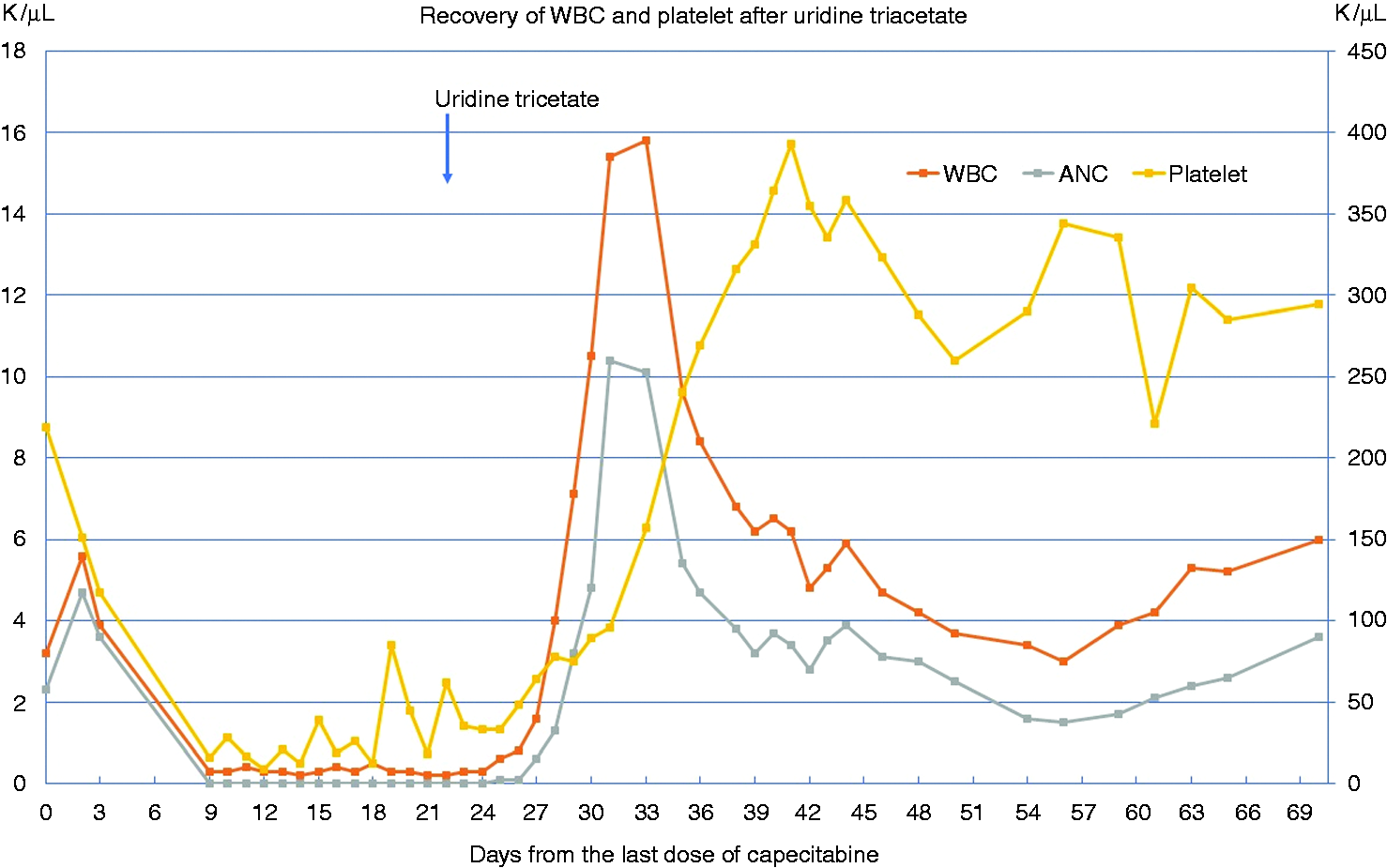
The patient’s hospital course was complicated by persistent pancytopenia with no response to daily filgrastim, severe mucositis, hemorrhagic colitis requiring total parenteral nutrition and blood and platelet transfusions, and mental status changes with extreme lethargy and confusion (Figure 1). She developed intermittent fever despite multiple antibiotics and recurrent episodes of paroxysmal ventricular tachycardia treated with amiodarone. By day 11 of hospitalization, the DPD assay ordered upon admission returned indicating the patient was positive for the homozygous DPD mutation c.1905 + 1 G > A (*2 A) variant, in which a splicing defect causes skipping of the entire exon 14 resulting in a nonfunctioning enzyme, and hence severe DPD deficiency. 15 At this point, despite maximal medical management, the patient was clearly deteriorating. Uridine triacetate was thus initiated as a desperate effort, three weeks after her last dose of capecitabine (Figure 1). The patient received a total of 20 doses of uridine triacetate via nasogastric tube as her mental status would allow. Her mucositis and pancytopenia started to improve six days after initiation of uridine triacetate. Improvement in her mental status and hemorrhagic diarrhea followed shortly thereafter. Five days after the completion of uridine triacetate treatment, by the time which the patient had recovered from her mucositis, diarrhea, lethargy, and pancytopenia, she suddenly developed right-sided weakness and recurrent confusion. Electroencephalography, lumbar puncture results, and magnetic resonance imaging (MRI) of the head were unremarkable. One week later, repeat MRI of the head showed a patchy abnormal signal in the pons, suggestive of central pontine myelinolysis. Throughout her admission, the patient’s blood chemistries were checked daily, and no sudden shift in her electrolytes was ever recorded to account for this. Over the next three weeks, the patient gradually recovered the use of her right side, experienced improvement in her mental status, and was discharged home after a total of five weeks of hospitalization.
Discussion
Severe life-threatening 5-FU toxicities can occur in patients with impaired clearance related to DPD deficiency. Such patients typically present with early onset severe toxicities, commonly with oral mucositis, diarrhea, and pancytopenia, and rarely, central nervous system toxicity and cardiomyopathy. Our patient did exhibit early onset symptoms but her presentation was atypical. She had presented with swollen lips and face, mild oral mucositis, and diffuse upper body rash soon after the last dose of capecitabine, responding to steroids with reduction in swelling and resolution of her rash. A hyperinflammatory response, masquerading as an allergic reaction, may be the first sign of homozygous DPD-related 5-FU toxicity and should have prompted early administration of uridine triacetate.
Further, the patient’s sudden development of right-sided weakness and mental confusion with MRI scans suggestive of central pontine myelinolysis was notable. Neurologic manifestations, such as somnolence, rapid deterioration of consciousness, and cerebellar ataxia are some of the less frequent 5-FU toxicities, occurring in about 5% of patients. 21 There have also been limited reports of neurologic events such as peripheral neuropathy, cerebellar dysfunction, and encephalopathy. 22 For DPD-deficient patients specifically, treatment with 5-FU can result in severe and prolonged neurologic toxicity. 21 Six previous reports of DPD-deficient patients treated with 5-FU involved occurrences of ataxia, confusion, seizures, motor neuropathy, and coma. 21 In a study that examined six breast cancer patients with 5-FU-induced leukoencephalopathy, the patients experienced slowly progressing symptoms, such as impaired cognitive function, ataxic gait, and abulia, with MRI on admission showing diffuse signal intensity changes on periventricular white matter. 22 Instances of multifocal inflammatory leukoencephalopathy and demyelination have been noted to occur during the first three weeks of chemotherapy.23,24 In experimental studies, when 5-FU was administered to dogs, lesions in the myelin and axons developed, but disappeared six months after termination of administration. 22 Most authors report improvement of neurologic symptoms in patients upon withdrawal of therapy with fluorouracil agents, and the period of recovery has been cited to range from one week to four months.6,21,25 Our patient’s neurological symptoms may have been a delayed manifestation of 5-FU neurotoxicity, and whether or not the uridine triacetate she had on board helped with her neurologic recovery is unclear.
The pharmacogenomics of fluorouracil were recently reviewed by Matsusaka and Lenz. Several genetic variations, including mutations in Orotate phosphoribosyltransferase, thymidylate synthase, and methylene tetrahydrofolate reductase, may contribute to excessive toxicity of 5-FU and capecitabine. 14 If our patient’s genetic test had resulted negative for DPD deficiency, she may not have received uridine triacetate given its cost and that three weeks had elapsed since her last dose of capecitabine. Since the mechanism of action of uridine triacetate is to replenish the cellular store of uridine counteracting the effects of 5-FU, independently of the presence of any genetic mutation, we believe that one should consider uridine triacetate if a patient develops severe, prolonged, and unexpected toxicity after 5-FU or capecitabine, regardless of the genetic test outcomes or whether the patient’s last dose is beyond the 96 h cutoff.
By the time of her second hospitalization, our patient was nine days post her last dose of capecitabine. It was notable that, despite provision of maximum medical support in the intensive care unit, the patient continued to deteriorate. To all the physicians involved in her care, it was clear that use of uridine triacetate was instrumental in her recovery. Without it, the patient likely may not have survived, suggesting that even the delayed use of uridine triacetate can potentially be lifesaving.
Overall, homozygous dihydropyrimidine dehydrogenase deficiency is rare, and genetic testing for DPD deficiency before 5-FU administration is generally not recommended. 15 With the widespread use of 5-FU and its oral prodrug, capecitabine, the number of patients with early onset severe toxicity could be substantial. Early recognition of this potentially catastrophic complication can be difficult, as our case illustrates. Additionally, the expense of uridine triacetate, along with the time restriction upheld by the FDA approved indication, limits its availability and usage. Of the 173 patients who were treated with uridine triacetate in clinical trials that included patients who enrolled after the new drug application submission, there were only eight early onset patients included who initiated treatment outside of the 96 h window, of which three (38%) survived. 1 Results from a trial including such a small number of early onset patients treated outside the window, it is felt, should not necessarily restrict the use of a potentially lifesaving medication in early onset severe toxicity cases. The outcomes of more cases, such as ours, that detail the use of uridine triacetate beyond 96 h post 5-FU, should hopefully prompt liberalization of uridine triacetate usage beyond the recommended 96 h treatment window.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.