
Abstract
Introduction
The increasing incidence of cancer and the finite capacity of hospital aseptic compounding units pose a serious challenge to the provision of cancer care. Chemotherapy dose-banding is a method of rationalising parenteral chemotherapy dosing and supply, whereby patient-individualised doses are rounded to predetermined banded doses. The banded doses may be outsourced as stock items which increases the supply capacity of the aseptic compounding unit.
Methods
Kotter’s 8-step change management model was used to structure the implementation of dose-banding of 5-fluorouracil 46-h infusers on the haematology–oncology day ward in St. James’s Hospital, Dublin. The impact of dose-banding on local practice was assessed through pre- and post-implementation surveys of stakeholders.
Results
In-house surveys of pharmacy, medical and nursing staff identified a generally favourable attitude towards implementing changes in the parenteral chemotherapy supply system, with some resistance to change evident. Dose-banding of 5-fluorouracil 46-h infusers was implemented successfully on the haematology–oncology day ward. Dose rationalisation and flexibility of re-allocation of standard banded doses between patients were the primary benefits of dose-banding found. Post-implementation surveys showed that clinical staff were in favour of adopting dose-banding into standard practice; however, they were cautious about the degree to which the results of this limited study would be translated into substantive benefits if dose-banding was adopted for all suitable preparations.
Conclusion
The success of the implementation process and the favourable opinions of stakeholders shown in the post-implementation survey enabled the dose-banding service to be extended to a further nine drugs. Kotter’s 8-step change management model was a useful tool for structuring this process change in St. James’s Hospital.
Introduction
Globally, the incidence of cancer is increasing due to the growth and ageing of the world’s population.1,2 Furthermore, the prevalence of lifestyles known to increase cancer risk, including smoking, poor diet and physical inactivity, as well as advances in the screening for and diagnosis of cancer, may contribute to the rising number of cancer cases.3,4
Cytotoxic chemotherapy drugs, one of the cornerstones in the treatment of many cancers, are frequently dosed using body surface area (BSA) in an attempt to achieve dosing uniformity in patients. 5 Despite well-documented limitations, BSA-based dosing continues to be the most common method for calculating chemotherapy doses.6–11 Dosing according to BSA leads to the preparation of individualised parenteral chemotherapy doses for patients. 12 In the Irish hospital setting, parenteral chemotherapy is compounded in a hospital aseptic compounding unit (ACU) or designated compounding area, or alternatively, the dose is purchased as a ready-to-administer, pre-compounded product from an external compounding facility licensed by the medicines regulator. 13
The manufacturing capacity of an ACU is thus a critical component in the provision of parenteral chemotherapy. Demand for chemotherapy is currently outstripping capacity in Irish cancer centres. 14 Irish cancer incidence projections predict the incidence of cancer in Ireland to double by 2040, while the number of patients having chemotherapy is projected to increase by 42%–48% between 2010 and 2025. 15
Since doses are usually prepared for patients shortly before administration in accordance with their clinical status and laboratory data, this can also add to capacity problems in hospital ACUs. 12 Provision of a substantial amount of what is known as ‘just-in-time’ compounding, for example within 24 h of administration, may cause delays for patients awaiting treatment when this high workload is unplanned.12,16–19
Dose-banding is a chemotherapy dose-rounding system, agreed between pharmacists and prescribers, whereby patient-individualised doses of parenteral drugs are rounded to predetermined banded doses. 12 A maximum variation of ±5% between the dose individualised by BSA or other parameters and the banded dose is typically allowed in dose-banding schemes. 12 The banded doses may be outsourced from external compounding facilities as stock items, which reserves ACU manufacturing capacity for drugs unsuited to dose-banding.12,17,20 For example, a 5-fluorouracil infuser may be prepared in a hospital ACU or alternatively, it may be outsourced as a pre-compounded, ready-to-administer product.
Nevertheless, dose-banding has potential drawbacks which must be considered before its introduction. Limitations of individualised BSA dosing also apply to dose-banding schemes based on BSA. 21 Dose-banding within ±5% is not thought to introduce clinically significant variation in dosing compared with a dose-individualisation system, and a number of studies have reported dose-banding within ±5% or ±10%10,16,22; however, further studies are needed to show that dose-banding is non-inferior to BSA dosing.6,21 Dose-banding is not recommended in extremes of bodyweight or in the paediatric setting and may only be used in clinical trials with prior agreement of the principal investigator and sponsor.21,23 In order to effectively manage stock, the key determinants for dose-banding are extended physicochemical stability after compounding (usually greater than 30 days) and a high prescribing volume for that drug.10,23
Assigning an expiry date for a product aseptically compounded in a hospital ACU is dictated by a number of factors including the physicochemical stability after compounding, the environment in which the product is compounded and the systems in place for quality control and quality assurance.17,24,25 In the absence of specific Irish national guidance on the maximum expiry date which may be applied to products compounded in unlicensed compounding facilities, a maximum expiry of seven days has been adopted by many hospital ACUs in accordance with guidance from the United Kingdom (UK).24,26 The physicochemical stability upon compounding remains a primary determining factor as some drugs will not be sufficiently stable to allow a seven-day expiry (for example, in St. James's Hospital, Dublin (SJH), azacitidine is assigned a 45-min expiry upon reconstitution).
Licensed compounding facilities operate to a higher environmental grade and have more robust quality control and quality assurance procedures in place than unlicensed hospital ACUs, which allows extension of the expiry date, provided physicochemical stability data are available. Ready-to-administer chemotherapy doses outsourced from licensed compounding facilities therefore typically have longer expiry dates than chemotherapy compounded in hospital ACUs. The long shelf-life gained from outsourcing dose-banded products permits a range of stock doses to be kept.16,27
Dose-banding has been described as a step forward in the rationalisation of chemotherapy preparation and dosing.12,16,17 Advantages of dose-banding have been demonstrated in several studies including reduction in chemotherapy turnaround time,16,18,22 reduction in patient waiting times for chemotherapy16,22,27 and reduction in wastage.16,27 Outsourcing dose-banded chemotherapy has been used as a strategy to improve pharmacy capacity.16,22 Dose-banding therefore balances the provision of high volumes of chemotherapy doses to meet demand and frees the limited capacity of hospital ACUs to meet the need for chemotherapy that must be individualised and/or has a short shelf-life.16,20
In SJH, the majority of parenteral chemotherapy is compounded in-house in the ACU with approximately 70% of it being prepared on a ‘just-in-time’ basis. The growing demand for chemotherapy is expected to eventually exceed the capacity of the services available in SJH. Two options were identified – significant capital investment in upscaling the in-house equipment, premises and staffing levels or alternatively, an increase in the number of products outsourced. Therefore, the feasibility of using a dose-banding system based on outsourced products needed to be evaluated as a strategy to manage increasing chemotherapy demand in SJH.
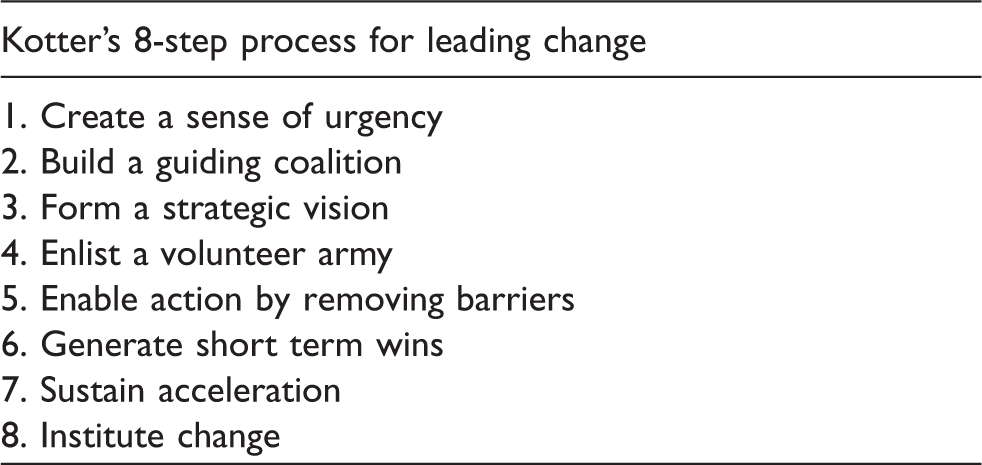
Since the introduction of dose-banding in SJH would require a multi-faceted change process which would affect members of the oncology multi-disciplinary team including nurses, pharmacists, pharmacy technicians and prescribers, a suitable method to manage the change was required. Kotter’s 8-step change management model has previously been applied in healthcare settings.28,29 The overall aim of this practice-based study was to implement dose-banding of 5-fluorouracil 46-h home infusers (5-FU infusers) in a clinical setting using Kotter’s 8-step change management model as a framework.
Methods
Setting
SJH is an acute, adult, academic teaching hospital with 1000 beds situated in Dublin, Ireland, and incorporates one of the eight cancer centres of the Irish National Cancer Control Programme (NCCP). Chemotherapy is supplied for administration on in-patient wards and on the designated haematology–oncology day ward (HODW).
Change management tool
Implementation of dose-banding
Inclusion–exclusion criteria for 5-FU infuser dose-banding.
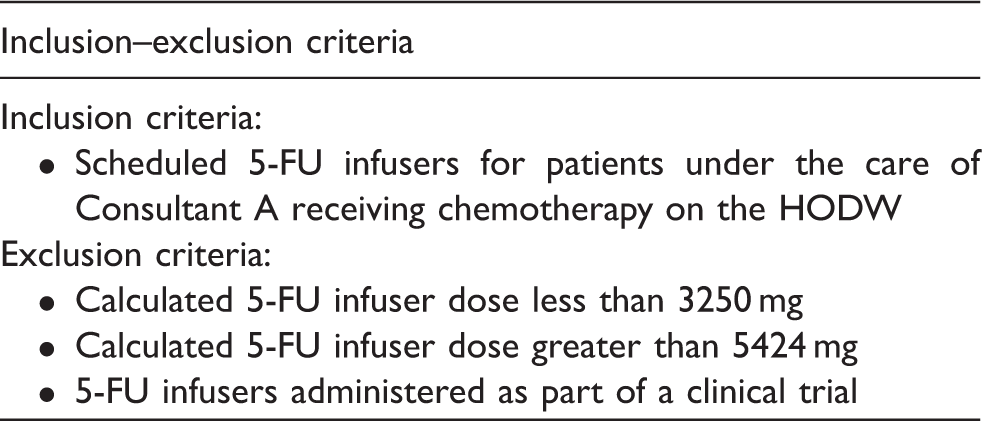
5-FU infuser: 5-fluorouracil 46-h infuser; HODW: haematology–oncology day ward.
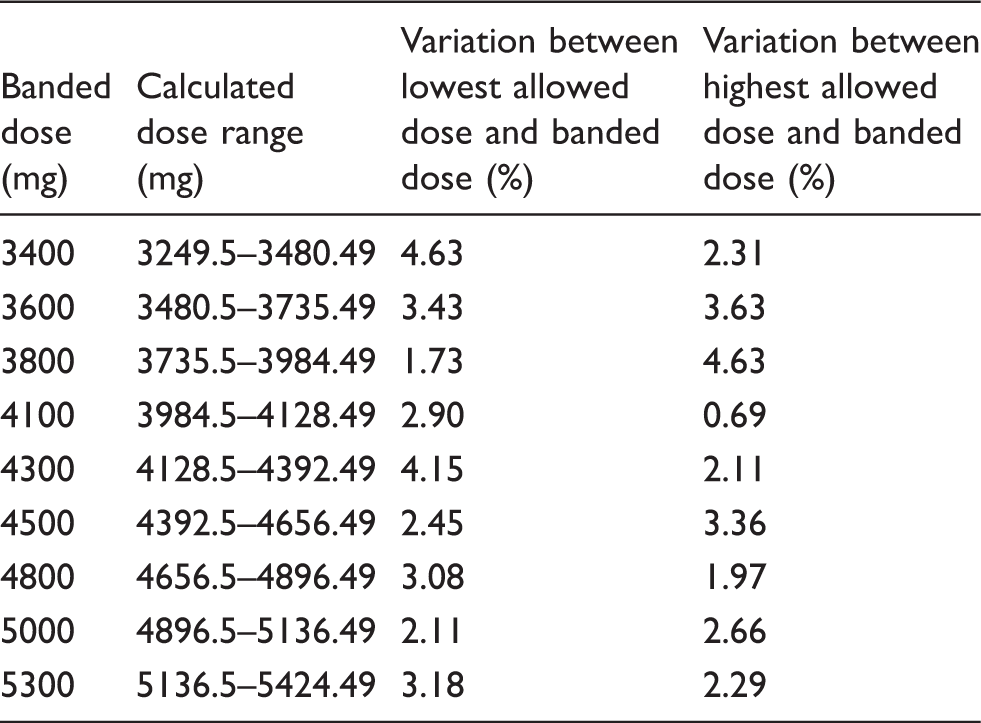
A retrospective review of 5-FU infuser data in SJH was conducted to establish local dosing and usage patterns, which was used to guide the selection and development of a dose-banding table suitable for use in SJH. The dose-banding table included nine banded doses for an overall dose range of 3250 mg–5424 mg and was adapted from previously published tables. 21
Dose-banding table for 5-fluorouracil 46-h infusers.
Pre- and post-implementation surveys
Pre-implementation survey.
BSA: body surface area; ACU: aseptic compounding unit.
Prescriber = registrar (n = 6), specialist registrar (n = 1).
Use of Kotter’s framework to introduce dose-banding on the HODW in SJH.
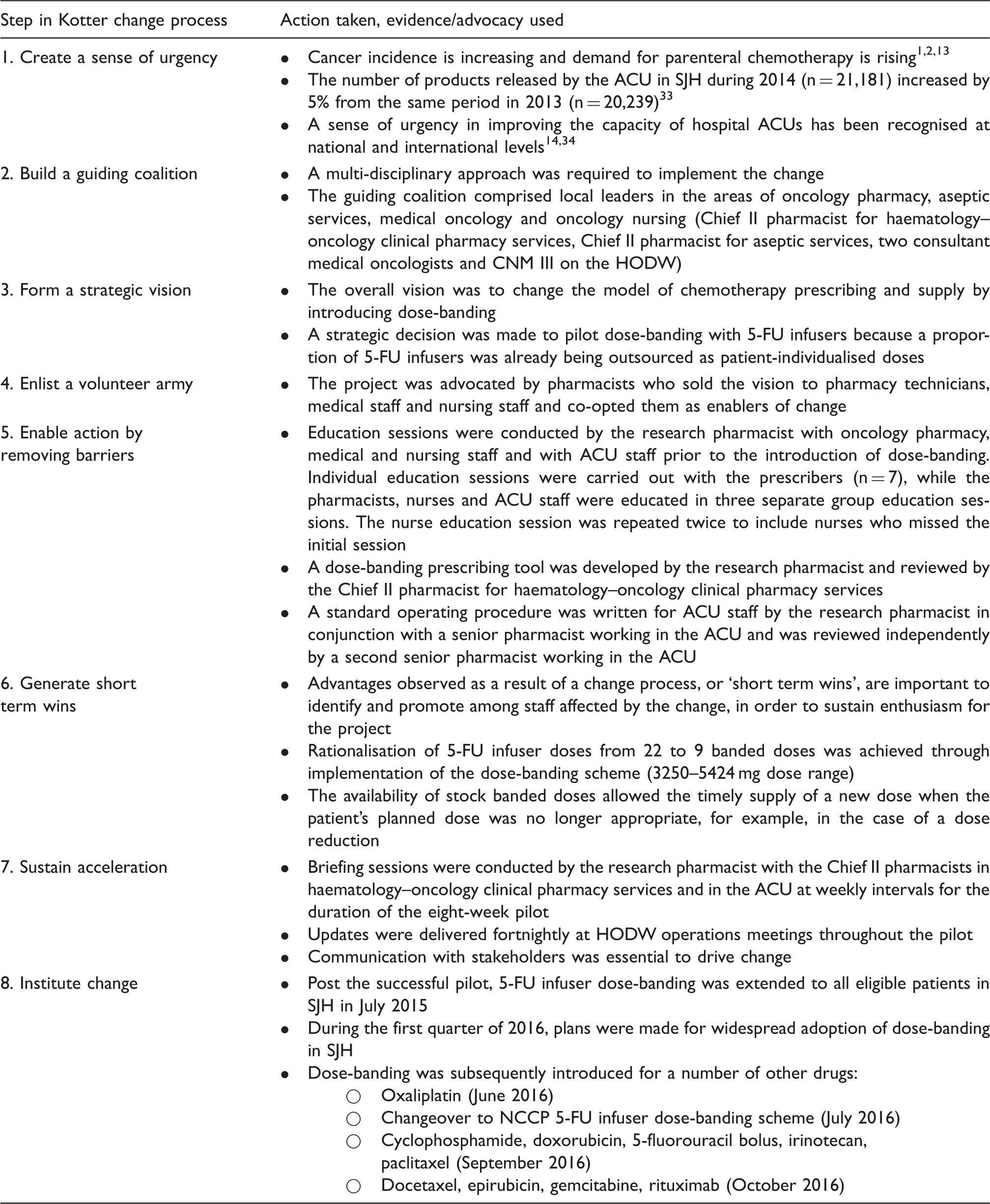
HODW: haematology–oncology day ward; SJH: St. James’s Hospital; ACU: aseptic compounding unit; CNM III: Clinical Nurse Manager III; 5-FU infuser: 5-fluorouracil 46-h infuser; NCCP: National Cancer Control Programme.
Post-implementation survey core questions.
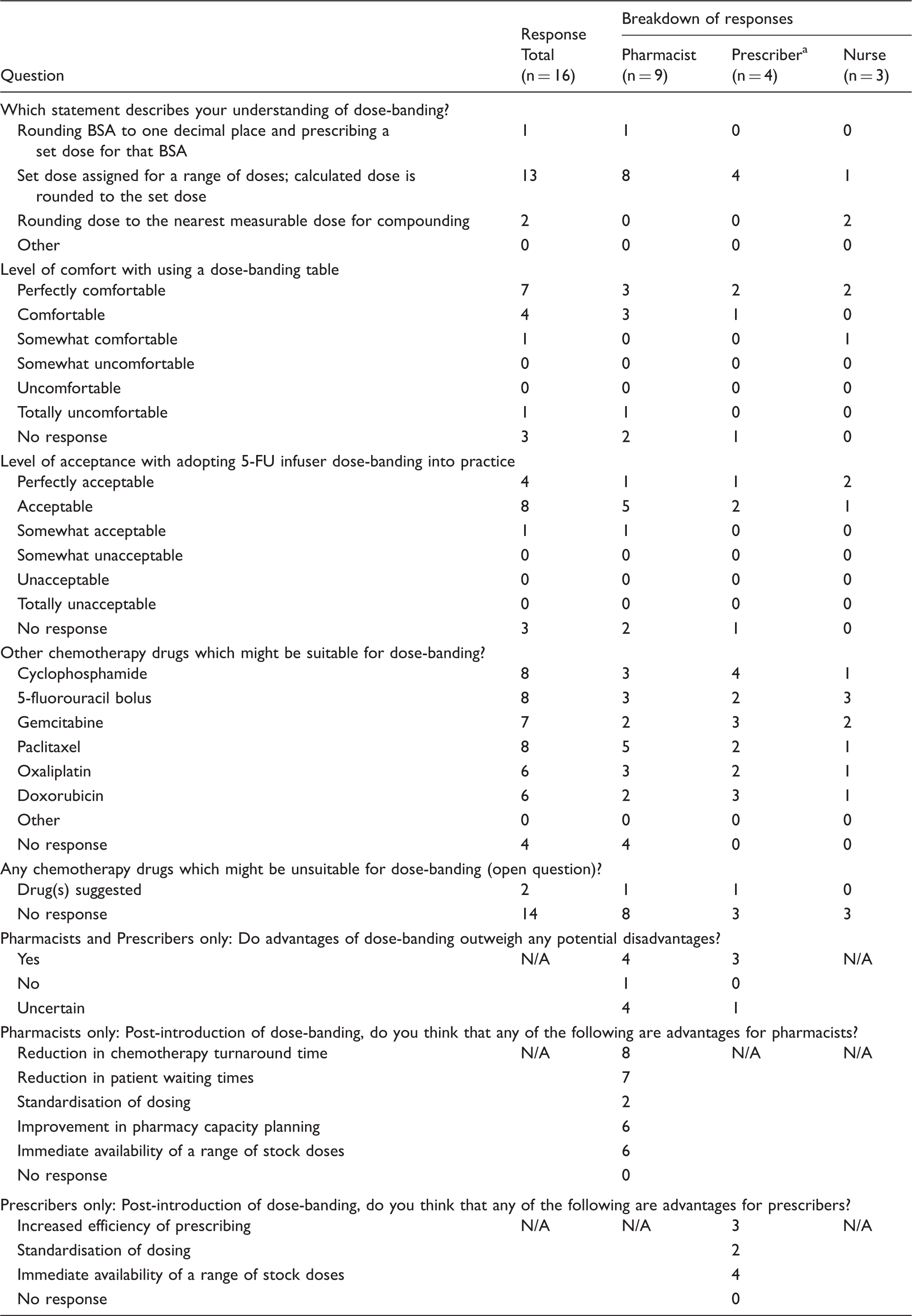
BSA: body surface area; 5-FU infuser: 5-fluorouracil 46-h infuser; N/A: Not applicable.
Prescriber = registrar (n = 3); specialist registrar (n = 1).
Results
Pre-implementation survey
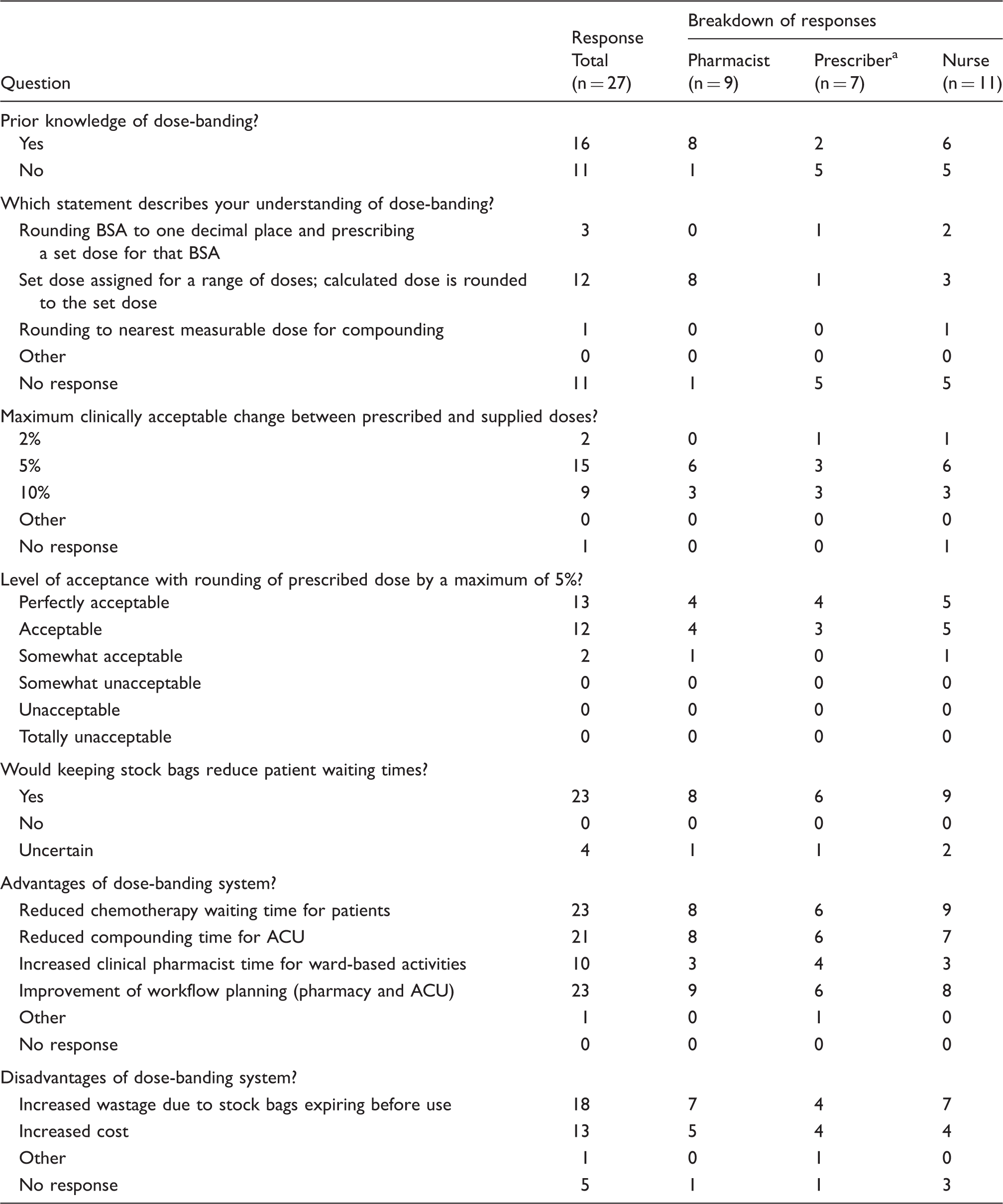
The pre-implementation survey (Table 4; Supplementary Material) was completed by 27 participants (response rate 84%). Overall, 16 of 27 respondents stated that they knew of chemotherapy dose-banding, with eight of nine pharmacists having heard of dose-banding previously.
In SJH, existing practice allowed a deviation of ±5% between the parenteral chemotherapy dose prescribed for a patient and the dose supplied by the ACU. All respondents were accepting of dose-rounding within a maximum of ±5%, with responses varying from somewhat acceptable to perfectly acceptable.
All survey participants believed there would be one or more advantages to having a dose-banded system, whereby stock doses of certain high-usage drugs would be kept by pharmacy. The majority of survey respondents (n = 22) thought that there would be one or more disadvantages of using a dose-banding system.
Implementation of dose-banding
Kotter’s 8-step change management tool was used to structure the implementation of 5-FU infuser dose-banding (Table 5).
30
During the period of data collection, 91% (n = 130) of 5-FU infusers scheduled for patients under the care of Consultant A on the HODW fit the inclusion–exclusion criteria and were dose-banded (Figure 1).
Application of inclusion–exclusion criteria.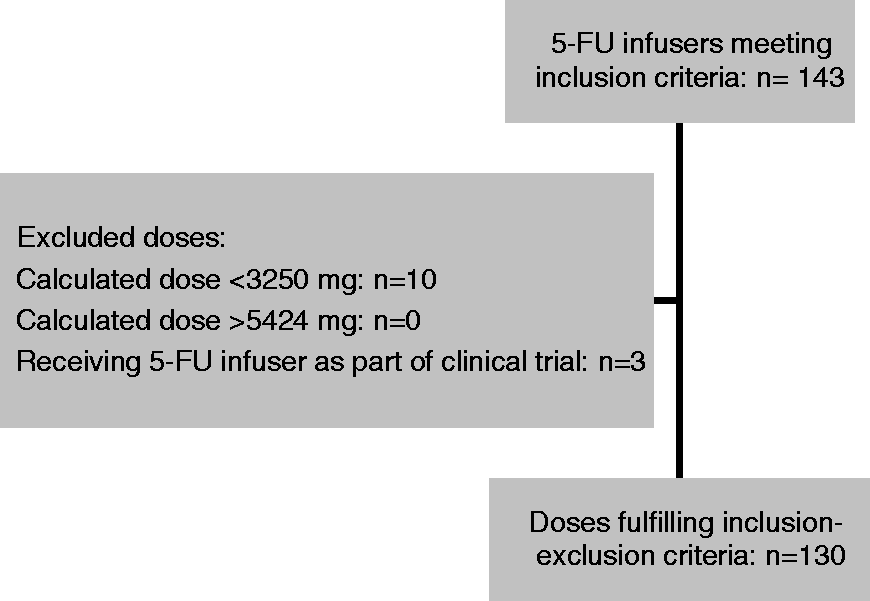
Post-implementation surveys
The post-implementation survey was completed by 16 participants (response rate 70%). A number of core questions were posed to all three professional groups, with pharmacists and prescribers also questioned on perceived advantages and disadvantages of a dose-banding system (Table 6, Supplementary Material).
Acceptance levels of adopting 5-FU infuser dose-banding into standard practice were positive, with 50% of respondents (n = 8) stating that this practice would be acceptable, while 25% (n = 4) stating that it would be perfectly acceptable. Respondents were asked whether they thought any other chemotherapy drugs would be suitable for dose-banding. The most frequently chosen responses were cyclophosphamide, 5-fluorouracil bolus and paclitaxel (50% in each case; n = 8).
All three professional groups were also asked an open question regarding drugs which may be unsuitable for dose-banding; however, only two respondents provided suggestions for this question. One pharmacist suggested that bortezomib and an intravenous admixture of doxorubicin and vincristine would be unsuitable for dose-banding, while one registrar thought that paclitaxel would be unsuitable.
Discussion
Successful implementation of dose-banding requires acceptance and adoption of the concept by members of the haematology–oncology multi-disciplinary team. 12 Pharmacy, medical and nursing staff in SJH were open to the concept of dose-banding, with all pre-implementation survey participants accepting of the established practice of rounding prescribed chemotherapy doses by a maximum of ±5%. This practice primarily allowed for rounding to the nearest measurable dose for compounding or re-use of chemotherapy in the event of treatment cancellation. Dose-banding formalises the practice of rounding doses to within ±5%. 12 This acceptance of dose-rounding, and consequently dose-banding, echoes survey results exploring opinions on dose-banding previously published.12,32
Acceptance of dose-banding by staff affected by the process change was crucial to the success of the project; however, the dose-banding scheme also needed to work in practice. The SJH 5-FU infuser dose-banding table used an approach whereby banded doses are assigned to defined dose ranges. This type of dose-banding table has broad clinical applicability since dose reductions can be accommodated by the table and the approach can be applied to chemotherapy drugs regardless of whether the drug is dosed according to BSA or another parameter (for example carboplatin dosing). 21
All 5-FU infuser doses that fit the inclusion–exclusion criteria for the project were prescribed according to the dose-banding scheme. Furthermore, an analysis of all 5-FU infuser doses prescribed on the HODW, indicated that the overall dosing range in the dose-banding table had good capture (>90%) for all patients prescribed 5-FU infusers. These preliminary results suggested that the dose-banding table could be rolled out to other prescribers of 5-FU infusers in SJH, if they were agreeable to the concept of dose-banding.
During the scoping stages of the project, stakeholder input was secured in each of the four employee groups who would be directly affected (pharmacy, aseptic services, medical oncology and oncology nursing); these key stakeholders comprised the guiding coalition in Kotter’s change management model and were all local leaders within haematology–oncology in SJH (Table 5). 30 Kotter explains that the biggest challenge in causing change is creating a strong sense of urgency. 35 In order to create a culture of urgency, the need to improve ACU capacity to cope with increasing chemotherapy demand was emphasised to the guiding coalition, who in turn, highlighted this urgency to members of the volunteer army who would be involved in implementing dose-banding.
A number of steps were taken to engage the volunteer army, including pre- and post-implementation surveys, education sessions and regular feedback on progress. The pre-implementation survey sought to determine baseline knowledge of dose-banding; however, it also served a dual purpose. The survey raised awareness of and promoted the dose-banding project to staff beyond the guiding coalition and reassured staff that the project was rooted in the context of everyday work processes in the ACU and on the HODW. Survey participants were asked to consider possible advantages of dose-banding, which could be considered as short-term wins. Short-term wins are needed to generate momentum and sustain enthusiasm for a project. 36
Identifying barriers to change is also crucial to ensuring the success of an intervention. 36 The members of the guiding coalition provided perspective on discipline-specific conditions of implementing dose-banding and potential barriers to change. Potential disadvantages of dose-banding were also identified from the literature.12,20,21 By asking pre-implementation survey participants about disadvantages of dose-banding, it was acknowledged that there are some limitations of the system.
The majority of pre-implementation survey participants (67%, n = 18) expressed concerns that a dose-banding system could increase wastage in the event that stock ready-to-administer chemotherapy expired before use. Preliminary results suggested that dose-banding in SJH may result in less wastage. During the pilot, 5% of dose-banded 5-FU infusers were discarded compared with 9% discarded pre-implementation of dose-banding; this benefit of dose-banding has also been described in the literature.16,19,27 If stock levels are managed correctly, taking advantage of the longer expiry date offered from outsourcing ready-to-administer chemotherapy, it should be possible in theory to minimise wastage.
When introduced in the UK in the 1990s, dose-banding was initially proposed as part of a strategy to rationalise chemotherapy dosing and chemotherapy service provision. 22 Prior to the introduction of dose-banding in SJH, 5-FU infusers were rounded to the nearest 100 mg for compounding, meaning that for the dose range of 3250 mg–5424 mg, 22 rounded doses were possible. Rationalisation of 5-FU infuser doses was achieved as a result of dose-banding. By standardising 5-FU infuser doses through dose-banding, the number of possible doses to be prescribed within the defined range was rationalised from 22 to 9.
Outsourcing of chemotherapy frees up capacity in an ACU as it limits the volume of compounding required. By rationalising the doses which are outsourced, ACU capacity can be further increased. Dose rationalisation reduces the number of potential standard doses which may be prescribed, which facilitates stock management processes. The availability of stock banded doses allowed the timely supply of a new dose when the patient’s planned dose was no longer appropriate. For example, this may arise if a patient is newly started on treatment at short notice or if a patient’s dose changes on the day of treatment. This benefit of dose-banding was confirmed in the post-implementation surveys of pharmacists and prescribers, with 10 out of 13 participants stating that this scenario was an advantage of dose-banding.
In the pre-implementation survey, 48% (n = 13) of participants thought that increased cost due to outsourcing chemotherapy would be a disadvantage of dose-banding. It is more costly to outsource chemotherapy than to compound in-house. However, if an ACU is working at maximum capacity with the available equipment and resources, some products will need to be outsourced if demands for chemotherapy are to be met in a timely fashion. Prior to this project, a proportion of 5-FU infusers were already outsourced by SJH on a named patient basis. 5-FU infusers were therefore chosen for the dose-banding pilot in SJH, to rationalise the outsourcing of these products and to develop a stock management system for banded doses.
Rationalisation of doses and establishment of a stock management system open up the possibility of creating a standard ordering system with an external licensed compounded facility. Stock chemotherapy levels could be topped up to the desired stock level once a week or once a fortnight. Weekly or fortnightly orders would be advantageous from the external licensed compounding facility’s point of view since the workload would be planned. The potential for negotiating prices on stock chemotherapy therefore exists; however, the scale of this study was not large enough to investigate this.
This practice-based study was carried out on a small scale, intentionally focussing only on 5-FU infuser dose-banding to trial dose-banding in a defined cohort of patients. However, the scale of the project may limit the generalisability of the results to other settings beyond SJH. Furthermore, the majority of the questions in pre- and post-implementation surveys were centred on local practice in SJH, to establish both successes of the pilot and areas which needed to be improved upon.
Of note, some post-implementation survey participants (n = 5) were uncertain as to whether advantages of dose-banding outweighed disadvantages and one survey participant thought that advantages did not outweigh disadvantages. Feedback from staff directly involved in the dose-banding dispensing process, suggested that ACU ordering, dispensing and checking processes needed to be further refined. Several staff members also pointed out that in order to explore the full benefits of dose-banding, the system should be rolled out to all consultants prescribing a particular drug, rather than having some doses patient-individualised and some dose-banded during the same time period. Monitoring of the costing of dose-banding by quantifying the change in stock levels and the amount of wastage would also be necessary to ensure that it was used for those preparations for which the benefits outweighed any disadvantages.
The pilot of 5-FU infuser dose-banding in SJH pre-dated Irish national guidance on dose-banding and was investigated to future-proof a possible method for coping with increased chemotherapy demand in SJH. While dose-banding had been in place in some UK hospitals since the 1990s, it was estimated in 2013 that less than half of all chemotherapy providers in England had adopted dose-banding. 20 No Irish data were found on the prevalence of dose-banding among Irish cancer centres; however, anecdotal evidence suggested that dose-banding policies were in place in at least three hospitals.
The NCCP was established to reorganise cancer care delivery in Ireland. 37 The NCCP acknowledged the rises in workload experienced in ACUs as a result of growing demand for chemotherapy in Ireland and recognised that there was a need to develop dose-banding guidance in an attempt to rationalise chemotherapy services. 38 Irish national dose-banding tables were developed by the NCCP and published during 2016 after this study had been completed. 39
Rationalisation of banded doses at a national level should lead to consistency of dose-banding practice across cancer centres. 23 Harmonisation of dose-banding across a region or country also provides an opportunity to improve the cost-effectiveness of a dose-banding scheme through competitive pricing of outsourced products.20,23
While Kotter’s 8-step change management model was used for the purposes of introducing a 5-FU infuser dose-banding pilot in SJH, the success of and lessons learned from the pilot paved the way for subsequent introduction of the NCCP dose-banding tables for a range of other drugs (Table 5). The positive acceptance levels of adopting 5-FU infuser dose-banding into standard practice observed in the post-implementation survey confirmed that clinical staff were supportive of the concept of dose-banding. Staff were cautious about the degree to which the results of this limited study would be translated into substantive benefits if dose-banding was adopted as standard practice for all suitable preparations.
Conclusion
Kotter’s 8-step change management model was used as a structure to prepare for the introduction and implementation of dose-banding on the HODW in SJH. Dose-banding is a viable option in SJH to rationalise outsourcing of chemotherapy with the aim of increasing ACU capacity.
Footnotes
Acknowledgements
The authors would like to thank the staff of the Pharmacy Department and the HOPe Directorate, SJH, Dublin who were involved in the project and are grateful for the support received from Dr Sinéad Cuffe, Prof John Kennedy, Jennifer Kerlin and Gail Melanophy throughout the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.