
Abstract

Cancer immunotherapy is one of the most rapidly evolving fields in medicine. Immune checkpoint inhibitors act by releasing a molecular brake-like programmed death-1 (PD-1) or its ligand PD-L1, thus enabling the immune system to attack and destroy cancer cells. These drugs are used to treat a number of patients with a wide variety of solid tumors including metastatic melanoma, non-small cell lung cancer, renal cell carcinoma, urothelial cancer, head and neck cancer, gastroesophageal cancer, hepatocellular carcinoma, and hematologic malignancies like Hodgkin’s lymphoma. Currently, there are several Food and Drug Administration-approved immune checkpoint inhibitors that target the PD-1/PD-L1 pathway: nivolumab, pembrolizumab, atezolizumab, durvalumab, and avelumab. 1
A healthy immune system is capable of destroying tumor cells. However, tumor cells and antigen-presenting cells often express immune checkpoints like PD-L1 on their surface. When PD-L1 molecules bind to PD-1 molecules on T cells, they inhibit T-cell function and the tumor cells evade immune surveillance. Immune checkpoint inhibitors directed against PD-1/PD-L1 restore immune function by inhibiting those inhibitory molecules.
Unbalancing of immune system leads to immune-related adverse events (IRAEs) in some patients treated with anti-PD-1/PD-L1 therapy. Diarrhea/colitis and pneumonitis are frequent causes of hospitalization among patients receiving immunotherapy. Grade 3/4 immune-mediated diarrhea/colitis are seen in approximately 1 to 2% of cases, 2 while the incidence of grade 3/4 pneumonitis have been reported in up to 1% patients. Other IRAEs include endocrinopathies, hepatotoxicity, renal toxicity, and dermatologic toxicity.
Recently, the composition of gut microbiome has been an active area of interest in cancer immunotherapy. Gopalakrishnan et al. 3 analyzed the oral and fecal microbiome in melanoma patients treated with anti-PD-1/PD-L1 therapy and showed that there is a significant difference in the diversity and composition of gut microbiome among responders vs. non-responders. In their study, they showed that the within sample diversity of gut microbiome, which takes into account both the number of different species as well as their relative distribution, was significantly higher among responders compared to non-responders.
Proton pump inhibitors (PPIs) are commonly used around the world for different indications including gastro-esophageal reflux disease and prevention and treatment of peptic ulcer disease. In 2013, esomeprazole (PPI), was the second largest drug in the US in terms of revenue. 4 A recent study by Imhann et al. 4 found that PPI use was associated with a decreased diversity of the gut microbiome as compared to the non-users.
Based on the information presented above, it was hypothesized that cancer patients receiving anti-PD-1/PD-L1 therapy, while taking PPIs concurrently, will have a different outcome compared to those who are not using PPIs.
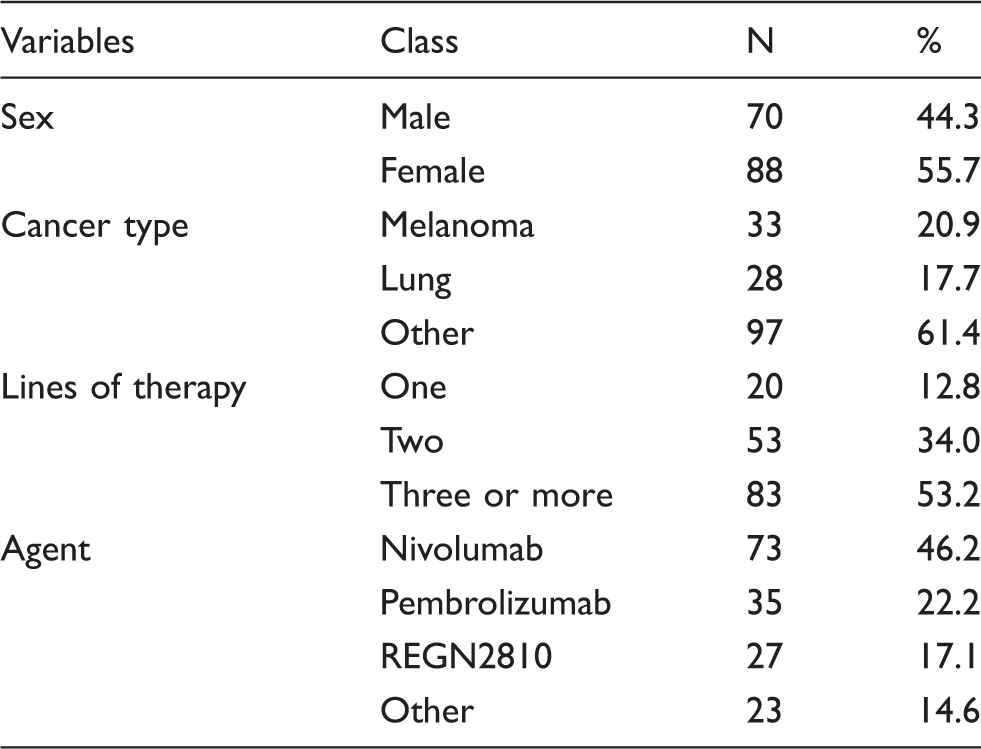
A retrospective review was performed on 158 patients aged 18 years or older, treated at the University of Oklahoma Health Sciences Center with anti-PD-1/PD-L1 therapy between 2014 and 2016. PPI use was assessed based on medical record review of prescribed and self-reported medications. This study was approved by the institutional review board. Our primary objective was to investigate whether the survival of patients treated with anti-PD-1/PD-L1 agents was affected by PPI use. Overall survival (OS) was defined as the time from getting first dose of anti-PD-1/PD-L1 therapy to death. Progression-free survival (PFS) was defined as the time from getting first dose of anti-PD-1/PD-L1 therapy to the first documented disease progression or death or loss to follow-up (whichever occurred first). Our secondary objective was to identify any differences in the immune-related side-effect profile between PPI users and non-users. Adverse events were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0. The OS and PFS were calculated using the log-rank tests. Survival curves were generated using the Kaplan-Meier method. The proportions of grade 3 or 4 colitis or pneumonitis were compared between PPI users and non-users using the Fisher’s exact test. We specifically selected grade 3 or 4 pneumonitis or colitis since they frequently lead to hospitalization. SAS 9.4 was used for the statistical analysis. All associations were considered statistically significant at an alpha error of 0.05.
Baseline characteristics of the study population.
The findings of this study have several limitations. Firstly, we recognize the inherent limitations of a retrospective analysis. Secondly, we did not assess the type and dose of PPI or compliance to PPI in our analysis. There is a significant difference in the acid suppression capacity among different types and doses of PPIs. 5 Differences in acid suppression may lead to different alterations in gut microbiome, thus potentially affecting response to anti-PD-1/PD-L1 treatment. Thirdly, we were not able to assess the effect of other medications which could potentially affect the gut microbiome. Lastly, this was a single institution retrospective study with a relatively small number of patients.
In conclusion, the composition of gut microbiome has been recently shown to affect the response to immune checkpoint inhibitors in melanoma patients. 3 Given that PPIs are known to affect the gut microbiome, 4 we examined the effect of PPI use in a cohort of patients treated with anti-PD-1/PD-L1 agents and did not detect a difference in outcomes. Further larger studies are needed to reexamine the effect of medications that alter the gut microbiome in patients receiving immunotherapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.