
Abstract
Objective
To evaluate the current NCI-CTEP recommendation and the clinical use of Calvert Formula-derived carboplatin dosing pattern in the treatment of advanced lung cancer patients and assess carboplatin-related toxicity in relation to the degree of dose fluctuation.
Methodology
This retrospective study involved all histologically confirmed inoperable lung cancer patients receiving palliative-intent carboplatin or carboplatin-combination chemotherapy from 2012 to 2016 at Kingston Health Sciences Centre. The carboplatin dosing pattern and carboplatin-related toxicity were collected and analysed on SPSS IBM for Windows version 24.0 (IBM Corp., Armonk, NY, USA). Results were expressed in percentages and P values.
Results
Our findings (N = 75) suggested that 24% of patients had a high-degree of fluctuation in carboplatin dose (>10% variation from initial dose) if carboplatin dose was readjusted with each new creatinine. In practice, 16% of patients had a fluctuation of greater than 10% in ordered dose in the absence of planned dose reductions. Our study found no significant association between prescribed high-risk dosing fluctuation (>10% increased from initial dose) and carboplatin-related toxicities.
Discussion and conclusion
In contrast to some prescribing recommendations such as NCI-CTEP, our study suggested that most medical oncologists incorporate new serum creatinine in calculating carboplatin dose for each cycle. Only 9% of patients were treated with a fixed dosing pattern (i.e. no fluctuation). Nonetheless, no significant associations were found between high-risk carboplatin dosing fluctuation and its-related toxicity. Whether such practice was due to the forcing function of the computer order entry system (CPOE), or conscious decisions by medical oncologists was unknown. Further analysis in evaluating physicians' preferences and influencing factors on dosing pattern decision would be recommended.
Keywords
Introduction
Platinum-based doublet combination therapy is a mainstay of treatment in patients with advanced non-small cell lung cancer (NSCLC) 1 and small-cell lung cancer (SCLC). 2 A recent meta-analysis shows different toxicity profiles but no differences in overall survival in both cisplatin- and carboplatin-based therapy in advanced NSCLC 3 or SCLC 2 patients. Carboplatin is often viewed favourably over cisplatin in the initial treatment for lung cancer in palliative settings given the toxicity profiles including less nausea and/or vomiting events, lower rates of neuropathy, nephropathy, and hearing loss.3–7
Carboplatin dosing is calculated via Calvert Formula, which incorporates target Area Under Curve (AUC) and Glomerular Filtration Rate (GFR). 8 Due to the lack of clinical convenience or resources of measuring the actual GFR, various formulas have been studied to compare estimated GFR to measured GFR.9–11 Serum creatinine acts as a surrogate for kidney function in all estimated GFR formulas.9–11
Electronic chemotherapy order entry is frequently used in order to reduce errors. In some chemotherapy order entry programs, creatinine is forced to be re-entered with each chemotherapy dose. This may lead to fluctuating doses of carboplatin based on serum creatinine, despite no meaningful difference in glomerular filtration rate. The National Cancer Institute-Cancer Therapy Evaluation Program (NCI-CTEP) recommends the usage of a fixed-dosing regimen of carboplatin based on initial serum creatinine and to continue with that same dosage throughout the subsequent cycles unless patients required dosage modification due to toxicity. 12 Other recommendations are to reduce doses in the case of increasing serum creatinine, but to not increase based on reductions in serum creatinine. A recent study suggests that most physicians tend to incorporate new serum creatinine in calculating carboplatin dose for each cycle, and that this practice patterns resulted in wide fluctuations in Calvert formula-derived carboplatin doses when compared to a fixed-dosing regimen. 13 We hypothesise that such practice may lead to under- or over-dosing of carboplatin, given that fluctuating serum creatinine levels may represent muscle wasting, physical condition, and nutrition status instead of the actual function of cortical collecting tubules. Thus, it is important to evaluate both dosing patterns in the context of clinical outcomes. This study aims to evaluate the dosing pattern in the cancer centre of Kingston Health Sciences Centre and its implication of carboplatin-related toxicity in relation to the degree of dose fluctuation.
Methodology
Setting, patients, study design, and measurement outcomes
We conducted a retrospective study utilising chart review. Ethics approval was obtained from Kingston Health Sciences Centre Research Ethics Board on August 2016. We included all patients with histologically confirmed stage 3 and 4 lung cancers (NSCLC and SCLC) receiving palliative-intent carboplatin-combination chemotherapy from 2012 to 2016 in the past five years at Kingston Health Sciences Centre. We excluded patients with stage 1 and 2 lung cancers as well as those treated with curative, neoadjuvant, or adjuvant intent. We also excluded patients who only received one cycle of chemotherapy and those who received cisplatin chemotherapy prior to switching to carboplatin due to toxicity. Patients were identified through a search of computerised order entry database at the hospital, which captured all carboplatin-based chemotherapy administered during this time period.
Demographic and medical information including age, gender, smoking history, Body Mass Index (BMI), height (first dose), weight (first dose), cancer types/stages, performance status, number of medications, treatment modality, and serum creatinine were extracted from the medical chart.
The estimated GFRs and theoretical carboplatin doses were calculated based on Cockroft-Gault Formula and Calvert Formula, respectively.
Hematologic toxicity was assessed from the laboratory values in the electronic medical record. They included anemia as defined by Chemotherapy-Induced Anemia WHO Classification Toxicity Level, 14 significant hemoglobin drop of ≥20 g/L, neutropenia (absolute neutrophil count ≤ 1.5 × 109 cells/L), thrombocytopenia (platelet <150 × 109 cells/L), fever (single measurement of Toral ≥ 38.3℃ or a sustained Toral ≥ 38.0℃ over 1 h), febrile neutropenia (fever as defined previously plus absolute neutrophil count ≤0.5 × 109 cells/L or ≤1.0 × 109 cells/L with an anticipated decline to ≤0.5 × 109 cells/L within a 48-h period), red blood cell or platelet transfusion use, and hospital admission.
Statistical analysis
To understand the impact of serum creatinine and weight changes alone in dose calculations, we compared the theoretical carboplatin dose for each cycle in comparison to the initial carboplatin dose calculated in cycle 1. We reported the frequency and the number of patients who had calculated dose fluctuations of greater than or equal to 20% from the initial dose, those who have a potential dose fluctuation of 10.1–20%, and those with no significant dose fluctuation (i.e. all doses within 10% of initial calculated dose).
In regards to understanding the impact of fluctuated dosing and toxicity, we expected that only patients for whom the fluctuating pattern resulted in a >10% increase in dose would have increased toxicity. This was based on standard practice that >10% dose increase was considered clinically significant. Previous study suggested that approximately 25% of theoretical carboplatin doses resulted in >10% dose increase when compared to cycle 1 based on serum creatinine alone. 13 However, there was no further evidence suggesting if such cut-off resulted in increased toxicity risks. We thus analysed patients for whom the dose increased by greater than 10% (i.e. high risk) for toxicity signals in comparison to those with no significant change in dose (i.e. low risk).
Descriptive statistical analyses were conducted on SPSS IBM for Windows version 24.0 (IBM Corp., Armonk, NY, USA) to evaluate different fluctuating dosing patterns in relation to its clinical outcomes. All independent variables were converted to categorical variables to increase sample size, and we used Fisher's exact test or Chi-Square test where appropriate. P-value was set to <0.05 to indicate statistically significant results. We also used the same method to conduct toxicity analyses on four different patient subgroups – elderly patients defined as age ≥65, overweight and obese patients with BMI ≥ 25, patients with polypharmacy ≥4 medications, as well as patients with combination of all the above.
Results
Patient flow and demographics
We identified 209 patients who received carboplatin-based chemotherapy for lung cancer regimens. Thirty-one patients were excluded for receiving one treatment cycle only, 31 patients for receiving curative/adjuvant intent chemotherapy, 10 patients for receiving carboplatin for a non-lung primary, one patient for not receiving their first cycle of chemotherapy, and 29 patients for receiving cisplatin prior to switching to carboplatin.
Thirty-two patients developed toxicity after the first cycle of chemotherapy. These patients were excluded from the analysis of toxicity based on dosing pattern, as they had not the ability yet to be classified into a dosing pattern after only one cycle. This left 75 patients for the toxicity analysis. Demographics can be seen in Table 1, Appendix 1.
Drug delivery, dosing method, and toxicity outcome
Most medical oncologists in Kingston Health Sciences Centre would input serum creatinine level at the beginning of each carboplatin dosing cycle via Cancer Care Ontario's Oncology Patient Information System (OPIS). Others would input serum creatinine level in the first carboplatin dose calculation and continue to use that dose unless patient experienced toxicity subsequently. This part of the practice was not standardised. In total, there were 185 cycles of carboplatin-based chemotherapy administered in cycles 2, 3, and 4. Table 2, Appendix 1 presented the differences in carboplatin theoretical dose calculated via Calvert formula in relation to its first-cycle calculated dose. Of the 185 cycles, cycles 12 (6%) and 24 (13%) showed a calculated dose which was decreased by ≥20% as well as a decrease of 10.1–19.9% from the initial theoretical dose, respectively. One hundred and seven (58%) of the cycles were within ±10% of initial theoretical dosing. In contrast, 24 (13%) and 18 (10%) cycles had calculated carboplatin doses which were increased by 10.1–19.9% and ≥20%, respectively from the initial dose. Similar patterns were observed on all types of carboplatin-based chemotherapy regimens. Overall, 18 of the 75 patients (24%) had an increase in calculated theoretical carboplatin dosing that was greater than 10% (i.e. high risk), based solely on reductions in serum creatinine.
A graphic representation of relationships between fluctuation of serum creatinine, theoretical carboplatin dosing pattern, and prescribed carboplatin dosing pattern in relation to cycle 1 could be seen in Figure 1. In all cases in which the creatinine clearance decreased, the dosing of carboplatin was reduced appropriately. Additional reductions in dose were seen beyond just that associated with creatinine increase in a substantial portion of patients. In cases (n = 37) where the calculated creatinine clearance increased – as a result of a decrease in serum creatinine – there were only six cases where the initial dose from cycle 1 was used (i.e. fixed dosing), whereas 31 cases demonstrated dosage calculation with new creatinine clearance. Only 1 of 75 (1%) patients received prescribed dose higher than the theoretical dose, while 42 (56%) patients received dose reduction of any degree. Thirty-two (43%) patients did not receive any dose modification. Of the 32 patients with no dose reduction, 7 (22%) and 1 (3%) were in the increased 10.1–19.1% and increased ≥20%, respectively. The average dose reductions in all cycles were 8.5%. Overall, 12 of the 75 patients (16%) received a prescribed carboplatin dose in the high risk group, which was reduced from 18 (24%) when compared to theoretical carboplatin dosing pattern.
Fluctuation of serum creatinine, theoretical carboplatin dosing pattern, and prescribed dosing pattern in comparison to cycle 1.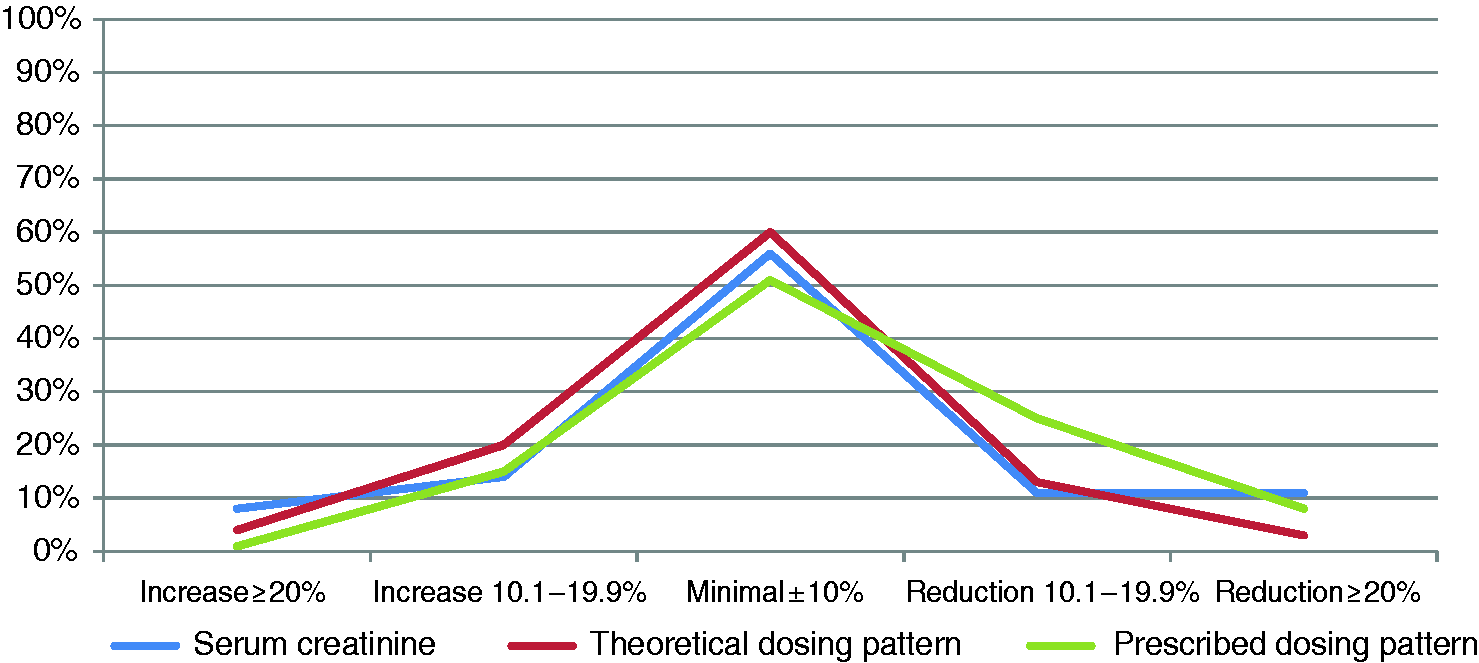
Toxicity results can be seen in Table 3, Appendix 1.
Discussions
Carboplatin dosing via the Calvert Formula had been a controversial issue, given that it was based on eGFR rather than an actual measurement of creatinine clearance. Within its limitations, current guidelines accepted its use along with Cockfroft-Gault formula in which the eGFR was derived. The discussion of various parameters such as obesity15–17 affecting serum creatinine was beyond the scope of our paper, and it had already been discussed in previous papers.15–17
Our study suggested that most medical oncologists in our cancer centre incorporated new serum creatinine in calculating carboplatin dose for each cycle, largely a result of the ‘forced’ input of creatinine into each new cycle. This clinical practice of carboplatin dosing pattern was consistent with other cancer centres. 13 Only 9% of patients had a fixed dosing pattern (i.e. no fluctuation) in our study.
For the majority of patients (51%), incorporating the new serum creatinine with each visit led to a minimal change of less than 10% from the initial dose. Nonetheless, we found no association between the extent of carboplatin dosing fluctuation and its related toxicities. This might be because physicians tend to practice dose reduction in cases where the calculated carboplatin doses were higher when compared to cycle 1. A calculated dose decrease of greater than 10% occurred in 33% of patients, while a calculated dose increase of greater than 10% occurred in only 16% of patients.
Previous study suggested that polypharmacy was a determining factor for medical oncologists in practicing chemotherapy dose reduction. 18 This was important due to the potential, complex chemotherapy-to-drugs interaction which might result in toxicity.19,20 Our study failed to confirm any significant correlation between high-risk carboplatin prescribed dosing pattern and carboplatin-related toxicity in the setting of polypharmacy (4 medications and above). Nonetheless, this might be secondary to small sample size, and that we only included the quantity rather than the type of medications in our analysis. Future study in this topic would be required.
Interestingly, patients who had toxicity after the first cycle of chemotherapy had higher subsequent creatinine and creatinine clearance fluctuations than patients who did not have toxicity after the first cycle. In fact, 25% of patients with first cycle toxicity had creatinine clearances change to an extent that their carboplatin dose would change by greater than 20% based on creatinine clearance alone. It may be that these patients had spuriously high creatinine clearance calculated at baseline, which led to the toxicity by second cycle, or that toxicity caused calculated creatinine clearance to change. This would need to be evaluated in a subsequent study.
There were several limitations to be addressed in this study. First, the nature of retrospective study might present difficulty in establishing temporal relationship between toxicity and carboplatin fluctuation degree. However, we had minimised such bias by eliminating patients who had developed toxicity with previous chemotherapy prior to carboplatin, as well as those who developed toxicity after first dose of carboplatin as they would not represent fluctuating dose–related toxicity. Second, the small sample size of this study might underestimate the result of our study. Nonetheless, we believed our results might be representative, given that the practice dosing patterns were consistent with previous study. 13 In addition, this limitation could be eliminated by involving other regional cancer centres. Lastly, we excluded 31 patients who received carboplatin as curative or adjuvant intent. We suspected that medical oncologists might practice less chemotherapy dose reduction in curative/adjuvant settings when compared to palliative intent; thereby, it might result in different fluctuating dosing patterns between various treatment intentions. Unfortunately, there was a lack of available supporting evidence. Future studies in this setting would eliminate this issue. Overall, we hoped this study would provide insights for physicians' awareness while prescribing carboplatin to their patients.
Conclusions
The current system avoided the issues associated with inadvertently overdosing patients who might be having a decrease in renal function. Fortunately, there were only a small minority of patients without first cycle toxicity (16%) who had a significant increase in creatinine clearance of more than 10% increased from initial dose. Further study evaluating physicians' preferences and influencing factors on dosing pattern decision would be important.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.