
Abstract
Background
Ibrutinib, a Bruton’s tyrosine kinase inhibitor has reformed the treatment of various B-cell malignancies including chronic lymphocytic leukemia, mantle cell lymphoma, and Waldenstrom’s macroglobulinemia. Although generally well tolerated, here we describe our institutional experience of unique adverse effects encountered with the use of ibrutinib in patients with B-cell lymphomas.
Methods
This is a retrospective observational study done at a tertiary care facility, to evaluate adverse events in patients with B-cell malignancies on treatment with ibrutinib between 2014 and 2018. Further details including type of malignancy, cytogenetics, interventions for treatment of the side effect, and outcomes were obtained through electronic health record.
Case series
We found 10 patients with unique adverse events related to ibrutinib. Among those, six had chronic lymphocytic leukemia, two had Waldenstrom’s macroglobulinemia, and two had mantle cell lymphoma. The events included palindromic rheumatoid arthritis, diffuse spongiotic dermatitis, bullous pemphigoid, recurrent hemorrhagic stroke, peripheral neuropathy, recurrent paronychia, intramedullary fibrosis, recurrent joint pains, pulmonary aspergillosis, dyspnea with exacerbation of atrial fibrillation, and resolution of autoimmune hemolytic anemia.
Conclusion
Our case series illustrates the wide variety of unique events recognized in patients treated with ibrutinib, some of which required cessation and most had dose reduction of the treatment. Thus, stressing the importance of early identification and intervention for the events to avoid worsening of toxicity and inability to continue treatment in such patients.
Introduction
Novel therapies targeting B-cell receptors (BCRs) and their signaling pathways are rapidly changing the treatment landscape of B-cell malignancies. Ibrutinib is one such drug, currently approved for chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma, mantle cell lymphoma (MCL), 1 lymphoplasmacytic lymphoma, 2 Waldenstrom’s macroglobulinemia, and in specific cases for marginal cell lymphoma, and chronic graft versus host disease. This drug targets the Bruton’s tyrosine kinase (BTK) pathway, binding with BCR to stop the downstream signaling process. This results in decreased proliferation and the promotion of apoptosis in malignant B-cells. Ibrutinib is undergoing continuous trials, including long-term phase III studies, as well as studies investigating the drug as a combination therapy for various types of malignancies.
When tested in clinical trials, ibrutinib demonstrated rapid responses with a relatively benign toxicity profile. The most commonly described adverse events (AEs) are hematological toxicities such as thrombocytopenia, neutropenia, and frequently bleeding diathesis. 3 The most commonly described nonhematological complications include gastrointestinal such as diarrhea, nausea, and stomatitis; 4 infectious complications such as recurrent upper respiratory tract infections and pneumonia; 4 cardiac side effects such as atrial fibrillation (AF); 3 and skin and musculoskeletal toxicity such as rash and arthralgia, respectively.
Although ibrutinib does have some off-site activity, it has a high specificity for the BTK receptor which results in less AEs than competing therapeutic agents, making it a potential drug of choice for many malignancies. 5 The main off-target effects of ibrutinib result from its activity on other Tec family kinases (TFKs), such as an interleukin-2-inducible T-cell kinase (Itk) inhibitor. Itk receptors regulate the immune response by activating the differentiation of helper T-cells, which plays a role in infection and tumor regulation. Therefore, although its off-target activity is helpful to disease regulation as well, there is evidence that it can result in long-term side effects such as slow turnover of bone due to osteoclast inhibition, 6 bleeding by interference in platelet and vascular collagen function, etc. 7 Most of our reported cases will associate with the off-target effects of ibrutinib.
In this case series, we report unique adverse effects found with the use of ibrutinib at our institution, in patients with B-cell malignancies. We aim to identify and report events that are not listed among the common adverse reactions for the drug and that physicians rarely see. Our goal is to share these cases with physicians at other institutions to fortify our collective wealth of experience. We hope that we can provide helpful information for further inquiry on the off-target effects of ibrutinib, guide potential combination therapy, and expand the breadth of the safety profile of the drug.
Methods
We conducted a retrospective study at a tertiary care facility. We sought to locate and record any unique side effects of ibrutinib reported at our institution between 2014 and 2018. This was done by searching patient records using the electronic health records database, “EPIC,” used in our institution. In this study, a unique AE was defined as such which had not been documented in literature at the time of review of these cases.
The study population here is defined as all patients with a diagnosed B-cell malignancy, who were treated with ibrutinib. First, patient records were filtered by B-cell malignancy. Next, they were filtered by the usage of ibrutinib as treatment. There were no limitations with regard to the length of treatment or minimum dosage of ibrutinib. Then, each patient chart was assessed individually for note of an AE. Once these patients and their AEs were identified, their specific diagnosis, cytogenetics, interventions undertaken to treat the side effect, and the outcomes were obtained and recorded.
Case series: Cases and management
Cases of unique adverse events with ibrutinib, their management and outcomes.
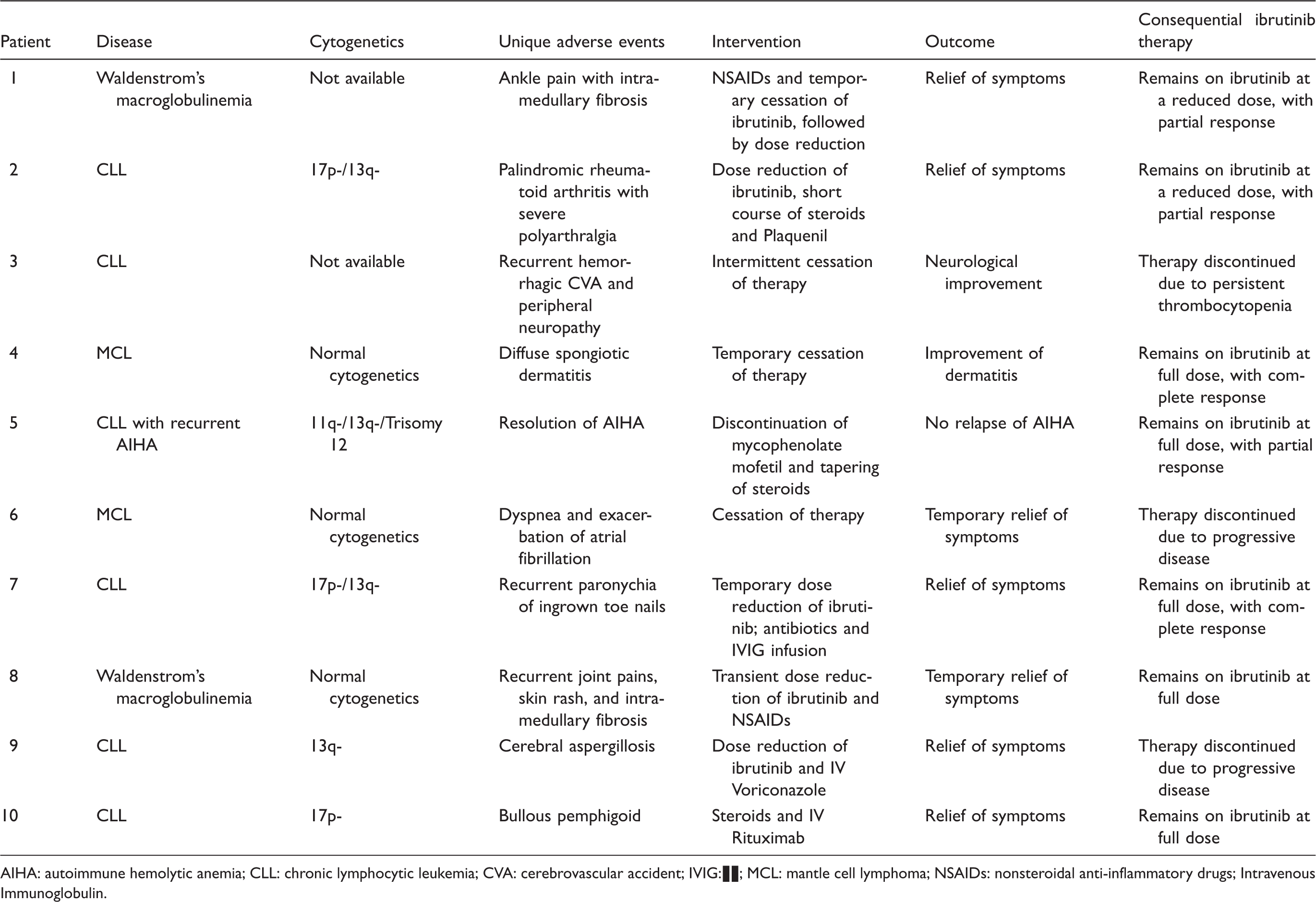
AIHA: autoimmune hemolytic anemia; CLL: chronic lymphocytic leukemia; CVA: cerebrovascular accident; IVIG:▪▪; MCL: mantle cell lymphoma; NSAIDs: nonsteroidal anti-inflammatory drugs; Intravenous Immunoglobulin.
The intervention for each case of unique AE included either a cessation in treatment with ibrutinib or a reduction in dose. With each cessation of treatment or reduction in dose, the symptoms of the AE were invariably decreased or relieved.
While four of our patients, including those with AEs of paronychia, diffuse spongiotic dermatitis, bullous pemphigoid, and skin rash with joint pains and intramedullary fibrosis were able to remain on ibrutinib at full dose after transient dose reduction or cessation in some of them, with full response of their malignancy; other three with AEs of cerebral aspergillosis, ankle pain with intramedullary fibrosis, and palindromic arthritis required dose reductions, with partial response of their malignancy. On the other hand, patients with AEs of recurrent hemorrhagic cerebrovascular accident (CVA) with peripheral neuropathy, cerebral aspergillosis, and dyspnea with exacerbation of AF had complete cessation of ibrutinib therapy due to various reasons as listed in Table 1.
To our best of knowledge, as allowed by limitations of retrospective review, we could not identify coinciding factors that could have accounted for the AEs in our patients that we associate with ibrutinib. For instance, patient 3 was not known to be on anticoagulants or antiplatelet agents that could have attributed to the recurrent hemorrhagic CVA in the patient. Nor did we find coinciding cardiovascular or respiratory diagnosis that could have explained new onset dyspnea in patient 6.
Some causes listed in literature for the discontinuation of ibrutinib therapy are disease transformation, progression of disease, AEs, etc. Three of our patients with unique AEs required discontinuation of therapy. Although our study did not establish such correlation, other studies have reported high-risk features and comorbidities in patients who required discontinuation of ibrutinib therapy. This usually confers poor prognosis, as 76% of the patients according to a study died after discontinuation. 8 Although now options such as Venetoclax and Idelalisib have offered some hope, in earlier years after approval of ibrutinib, with not many other options, discontinuation of ibrutinib conferred poor prognosis.
Although resolution of autoimmune hemolytic anemia (AIHA) is more of a favorable than AE, we decided to report this, being novel and related to the therapy with ibrutinib.
Discussion
In analyzing the AEs associated with the drug, it is important to recognize that while traditional chemotherapy is offered in time-limited regimens, targeted therapies are generally taken until disease progression or unacceptable toxicity. Lifelong dependency on a drug certainly calls for rigorous precaution or therapy for AEs, so as to be able to recognize them as early as possible, and the discontinuation of what would need to be lifelong therapy can be avoided.
Ibrutinib is generally well tolerated. The most common AEs of the drug reported in patients with B-cell malignancies are grade 1 or 2 in severity and commonly include thrombocytopenia (62%), neutropenia (61%), diarrhea (43%), anemia (41%), musculoskeletal pain (30%), bruising (30%), rash (30%), fatigue (29%), nausea (29%), hemorrhage (22%), and pyrexia (21%). 5 AEs that are of grade 3 or higher are uncommon with no proven relationship to length of treatment or dose. AEs tend to happen shortly after beginning treatment and become less common the longer the patient is taking the drug. The studies to date have shown that most AEs occur within first 15 months of the treatment. 8
Ibrutinib has pharmacokinetics sensitive to metabolic interactions. Severe diarrhea was reported in a patient, attributed to the interaction between ibrutinib and verapamil, a CYP3A4 inhibitor. 9 This fact is important as ibrutinib’s adverse effects continue to be studied, as well as the efficacy in combination therapy.
Ibrutinib has on- and off-target activity, and a large number of adverse effects result from off-target activity. 6 TFKs are the major off-target of ibrutinib, which are expressed across several cells lines, largely in the hematopoietic lineage. Other TFKs include Itc, Txk, Bmx, and Tec, located in the liver, endothelial cells, osteoclasts, etc. 6 Attenuation of these collective pathways is generally known to inhibit the inflammation, hence the anti-inflammatory activity of ibrutinib. 6
It is interesting to note that while binding BTK results in inhibition of B-cells, NK cell activation, and cytokine production, it spares the production of Ig while inhibiting the production of autoantibodies—thus potentially having a beneficial effect on autoimmune conditions. 6
As mentioned earlier, hematologic toxicities are the most commonly reported AEs in patients being treated with ibrutinib. Although, following standard chemotherapy, ibrutinib has the potential to improve cytopenias, its activity on BTK and Tec receptors on endothelial cells and various other blood cells is a proposed mechanism for bleeding. 6 Thrombocytopenia and platelet dysfunction can serve as alternate explanation for the bleeding events. Reportedly, 50% of patients on ibrutinib develop minor bleedings and around 5% have major bleedings, 10 mostly during the first two years on ibrutinib. 11 This becomes particularly challenging in patients who are on antiplatelet or anticoagulant agents. Although the majority events are mucocutaneous, cases of hemorrhagic stroke such as ours have also been observed, albeit rarely, likely from platelet dysfunction, VWF-mediated platelet activation, and disruption of the vascular system by acting on collagen and endothelial cells. 7 Besides CVA, occurrence of peripheral neuropathy in our patient was particularly unique, which we cannot explain with any known mechanisms.
Ibrutinib has shown anti-inflammatory and antifibrotic properties by inhibiting TFKs, mainly in the setting of autoimmunity. By inhibiting EGFR, on the other hand, it displays proinflammatory properties, particularly on the skin, resulting in cutaneous eruptions. 12 Skin rashes are a common AE of the drug, although spongiotic dermatitis and skin rash with intramedullary fibrosis and severe arthralgia is unique to our experience. An increased incidence of skin rash with WM is not evident yet.
Besides its anti-inflammatory activity and inhibition of B lymphocytes, ibrutinib is known to inhibit NFATc1—a major transcription factor for osteoclastogenesis, being a downstream signal of BTK, which is also expressed on osteoclasts; 6 thus, proposing the ability of ibrutinib to attenuate rheumatoid arthritis (RA).6,13
Although ibrutinib appears to be capable of anti-inflammatory effects, alleviate symptoms of autoimmune arthritis, and has been studied in mice for treatment of arthritis, 6 arthralgia persists as an AE in patients on ibrutinib, frequently to such severity that it can require termination of treatment. Three of our patients had joint pains, among whom one developed palindromic RA, the latter being novel AE of ibrutinib to our knowledge. Considering the protective effects of ibrutinib in arthritis and atopic dermatitis, the latter through Itk inhibition, 6 it is difficult to understand the pathogenesis of the palindromic arthritis in our patient or the constellation of rash–arthralgia–fibrosis. These could have something to do with osteoclast metabolism or the disturbance of inflammatory markers.
The resolution of AIHA, on the other hand, although it has never been observed before, goes well with ibrutinib’s antiautoimmunity properties. The myelofibrosis cases are unexplained and have occurred in our patients despite the known antifibrotic activity of ibrutinib. Some rare side effects such as reduction in anti-insulin and glutamic acid decarboxylase antibodies presenting in hypoglycemia have also been noticed. 14
BTK is also expressed in cardiac tissue. With inhibition of this pathway in the heart, PI3K–AKT signaling—which is cardioprotective—is inhibited as well. This is one mechanism proposed to cause of arrhythmias, particularly AF, in patients being treated with ibrutinib. Another possible mechanism is its off-target effects on TFKs and ErbB2/HER2, which are both expressed in heart. 6 According to the Pharmacyclics, grade 3 or greater AF and atrial flutter occurred in 0–6% of patients. Dyspnea, which was either related to the AF or was an independent AE in our case, has been reported as a side effect in 25% of patients in a study on the efficacy of ibrutinib in combination with lenalidomide and rituximab, and presented as grade 3 and 4 in 8% of patients. 15 Although with time many cases of AF likely associated with ibrutinib have surfaced, we decided to report this due to co-occurrence with dyspnea, which could or could not be interrelated.
Although opportunistic infections are not common with ibrutinib therapy, and it is known to offer protection against severe infection and sepsis in mice, 6 as well as in phase III clinical trials, 16 possibly by causing increase in Ig levels, 17 there remain reports of invasive fungal infections, such as in one of our patients. In a retrospective study of 33 cases of invasive fungal infections in patients taking ibrutinib, 27 were of aspergillosis, demonstrating its predominance. 16 Other less common side effects on the grounds of induced immunosuppression, for instance progressive multifocal leukoencephalopathy 18 and malakoplakia 19 have been reported.
To our knowledge, paronychia has not been reported as an adverse effect of ibrutinib before. Although it has been reported as an adverse effect of an EGFR inhibitor, afatinib; 20 knowing that ibrutinib does have some EGFR-inhibiting activity, 6 this could explain the recurrent paronychia in our patient. There are reports of other nailbed abnormalities, especially trachonychia, that occur in relationship to ibrutinib therapy. 21
Conclusion
We hope that knowledge of our cases can result in earlier detection and that practicing physicians will quickly recognize and manage such events. Overall, it appears that discontinuation of ibrutinib due to toxicity is rare. In a few rare but severe cases, as we present above, discontinuation of therapy was necessary. Early identification and intervention may mitigate worsening of toxicity and perhaps prevent cessation of an otherwise beneficial drug. In the future, we may see development of methods of early recognition for rare but severe AEs, in order to even further decrease rates of therapy discontinuation, increase the efficacy of the drug, and reduce patient morbidity and suffering.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.