
Abstract
This is a case report of a patient who developed severe, irreversible hypocalcemia after receiving one dose of pamidronate 90 mg for hypercalcemia of malignancy. Hypocalcemia is a known risk of bisphosphonate treatments, but the incidence of severe hypocalcemia is rare, and the risk factors are well established. However, in the treatment of hypercalcemia of malignancy, the treatment objective is to reduce the elevated serum calcium level, and the bisphosphonate is usually given as one time dose only. The potential for developing severe hypocalcemia may not be considered a significant concern in this setting compared to the setting of the treatment of bone metastasis, where the baseline serum calcium level is not elevated and the bisphosphonate is administered at a regular interval of every three to four weeks. Furthermore, there is unawareness of prevalence of vitamin D deficiency in cancer patients, especially in those with advanced cancer, which may lead to inadvertent, severe hypocalcemia from bisphosphonate treatment. The objective of this case report is to bring awareness to the risk of severe hypocalcemia in patients with hypercalcemia of malignancy and the high prevalence of unrecognized vitamin D deficiency in cancer patients.
Introduction
In oncology, bisphosphonates, such as pamidronate and zoledronic acid, are widely used for the treatment of bone metastases and hypercalcemia of malignancy. Bisphosphonates induce apoptosis of osteoclasts resulting in the inhibition of bone resorption and calcium efflux from bone into the systemic circulation. 1 Inherently, there is a risk of developing hypocalcemia from bisphosphonate treatments, and patients with impaired maintenance of calcium homeostasis are at risk of developing severe and even irreversible hypocalcemia. Nevertheless, the overall incidence of hypocalcemia is rare, and it is usually transient and mild in nature.
In the treatment of bone metastases, where the baseline serum calcium level is in the normal range usually, the risks for developing severe hypocalcemia are reviewed before bisphosphonate treatment is initiated. However, in the treatment of hypercalcemia of malignancy, where the treatment objective is to reduce the elevated serum calcium level and the bisphosphonate is usually given as a single dose, the potential for developing severe hypocalcemia may not be considered a significant concern and thus the risk factors are not reviewed carefully.
Furthermore, there is lack of awareness of the prevalence of undiagnosed vitamin D deficiency in cancer patients, especially in those with advanced cancer who may develop hypercalcemia of malignancy, which may lead to inadvertent, severe hypocalcemia. This is a case report of a patient who developed severe, irreversible hypocalcemia after one dose of pamidronate 90 mg administered for hypercalcemia of malignancy. He was admitted to the hospital and given calcium, vitamin D and other electrolyte replacements, but hypocalcemia remained severe and refractory. He succumbed to the rapidly progressing cancer during the admission. The objective of this case report is to bring awareness to the risk of severe hypocalcemia in patients with hypercalcemia of malignancy and the high prevalence of unrecognized vitamin D deficiency in cancer patients.
Case report
A 64-year-old man presented to his family physician with dysphagia and odynophagia. His medical history was significant for Barrett's esophagus, hypertension, diabetes mellitus, bilateral carotid artery stenosis, peripheral vascular disease, and three episodes of myocardial infarction. It was also significant for chronic, idiopathic hyponatremia and query hypomagnesemia. He had approximately a 40-pack year history of smoking, which he quit a few years ago. He estimated a few drinks of either wine or beer a day, but denied alcohol abuse. His home medications included acetylsalicylic acid, atenolol, atorvastatin, clopidogrel, hydrochlorothiazide (HCTZ), magnesium oxide, metformin and ramipril. He had no known allergy to medications.
Panendoscopy revealed locally advanced laryngeal carcinoma with hypopharyngeal involvement. He underwent total laryngectomy, total thyroidectomy and partial pharyngectomy with pharynx reconstruction. His parathyroid glands were spared. He recovered from the surgery uneventfully and was discharged less than two weeks after the surgery on a new medication of levothyroxine. The final pathology and diagnosis were T4aN2cM0 squamous cell carcinoma of larynx with extracapsular extension, three positive lymph nodes and perineural invasion.
He was planned for adjuvant chemotherapy treatment, but during chemotherapy planning he was found to have low serum calcium level of 1.86 mmol/L (7.5 mg/dL), (normal range, 2.20 to 2.62 mmol/L; 8.8–10.5 mg/dL). The albumin and the 25-hydroxyvitamin D (25-OHD) levels were not done. The parathyroid hormone (PTH) level was done and it was less than 0.3 pmol/L (normal range, 1.3 to 7.6 pmol/L). The serum magnesium level was normal. He did not have symptoms of hypocalcemia, such as tingling or numbness of the extremities, muscle weakness, palpitations or seizures. He was admitted to the hospital and treated with intravenous (IV) calcium, oral calcium and oral calcitriol. After 48 hours, the serum calcium level normalized, and he was discharged at his wish with a prescription for Calcium Sandoz 1000 mg orally three times daily and calcitriol 0.25 μg twice daily.
Subsequently, during re-planning of his treatment, he had hyponatremia, hypomagnesemia, hypophosphatemia and hypocalcemia on separate occasions requiring electrolyte replacements and investigations. His treatment was further delayed by another two months as a result. During the investigation, the 25-OHD level was found to be low at 36 nmol/L (normal range, 61 to 200 nmol/L) and the thyroid stimulating hormone was elevated at 14.38 mIU/L (normal range, 0.35 to 4.94 mIU/L). It was not clear if the patient had been compliant with oral calcitriol. The levothyroxine and calcitriol doses were increased to 0.15 mg once daily and 0.5 μg twice daily, respectively, and the patient was restaged with the computed tomography (CT) imaging. The CT of chest revealed lung metastases that developed in the interim and he was started on a clinical trial palliative chemotherapy treatment with vorinostat and capecitabine. During the treatment, he did not report any diarrhea, although he lost just over 5% of his weight due to reasons unavailable at the time of the report. The serum creatinine was 94 μmol/L (normal, less than or equal to 109 μmol/L) at the start of the treatment and peaked to 118 μmol/L after the second cycle of treatment, but went down to 86 μmol/L afterwards. Also, after the second cycle of treatment, he was found to have hypocalcemia, hypomagnesemia, hypophosphatemia and mild hypokalemia but they were all amenable.
After two cycles of chemotherapy treatment on clinical trial, the CT of chest was repeated. It revealed progression of the lung metastases, and the treatment was changed to a second-line, single agent gemcitabine. He received a total of three cycles of gemcitabine without recurrence of hypocalcemia, and the serum creatinine remained within the normal range. The CT of the chest was repeated, which showed further progression of the lung metastases with new bilateral pleural effusion. In addition, the CT of the head revealed new brain metastasis, and the bloodwork revealed corrected serum calcium level of 3.10 mmol/L (12.4 mg/dL). The treatment with gemcitabine was discontinued, and he was given one dose of pamidronate 90 mg IV. His serum creatinine was slightly elevated at 114 μmol/L with estimated creatinine clearance of 60 mL/min using the Modification of Diet in Renal Disease (MDRD) equation.
Nineteen days later, he was found to have corrected serum calcium level of 1.63 mmol/L (6.5 mg/dL). He was admitted to the hospital for urgent treatment with IV calcium. He was symptomatic with right finger spasms, and the electrocardiogram showed prolonged QTc of 522 ms. He was treated with IV calcium gluconate, oral calcitriol, oral calcium carbonate, but his hypocalcemia remained refractory. The serum calcium level went up to 1.85 mmol/L (7.4 mg/dL) maximum before dropping again.
In the ensuing days, he became more drowsy and fatigued. The CT of brain showed further progression to multiple brain metastases. On day five of admission, he went into coma. With his cancer progressing rapidly and the performance status declining, his wife agreed to stop active chemotherapy treatment. The patient was maintained on electrolyte replacement and comfort measures. He passed away two days later.
Discussion
Bisphosphonates
Bisphosphonates are synthetic analogues of pyrophosphates, also known as biphosphates. They have high affinity for divalent metal ions, such as calcium. 2 After they are administered intravenously, they are rapidly cleared from the circulation and taken up by osteoclasts, where they cause apoptosis. 2 This results in reduced osteoclast activity and reduced calcium efflux from bone into the circulation. The second and third generation bisphosphonates pamidronate and zoledronic acid, respectively, also known as amino bisphosphonates, are widely used in the treatment of bone metastases and hypercalcemia of malignancy. While both pamidronate and zoledronic acid are highly effective, zoledronic acid is the preferred agent due to the following reasons: a shorter infusion time of 15 minutes, versus 2 to 4 hours for pamidronate; greater antiresorptive potency of about 1000 times that of pamidronate; and longer serum half-life, all of which result in slightly longer duration of antiresorptive effect.3–5 In the treatment of hypercalcemia of malignancy, decline in the serum calcium level is observed about 48 hours following a bisphosphonate dose and normalization of the serum calcium level is observed in about seven days.3,6–8 It is noteworthy the first infusion is often associated with flu-like symptoms, such as bone pain, fever, chills and headache, but the subsequent infusions are generally better tolerated.
Hypercalcemia of malignancy
Hypercalcemia of malignancy occurs in up to 20% of patients with advanced cancer. 9 It is most commonly observed in patients with multiple myeloma, breast carcinoma, renal cell carcinoma and squamous cell carcinoma of any organ. 3 The symptoms of hypercalcemia depend on the actual serum calcium level and the rapidity of its development. 3 Hydration is the first principle in the treatment, as many of these patients are often dehydrated and/or have hypercalcemia-induced renal defect in electrolyte clearance. 3 Usually, a bolus of 1 to 2 liters of normal saline helps restore the fluid balance and enhances calcium excretion. The hydration alone can reduce the serum calcium level by up to 0.5 mmol/L. 3 Maintenance of IV hydration depends on the patient's fluid status.
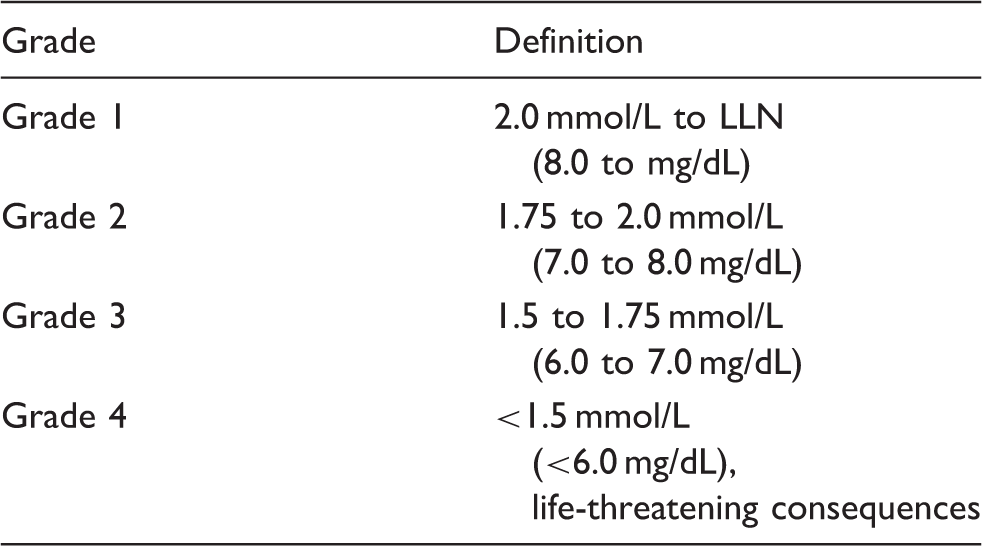
Subsequently, depending on the patient's serum calcium level and the clinical presentation, treatment with a bisphosphonate may be required. 3 If the corrected serum calcium level is greater than 3.1 mmol/L (12.5 mg/dL) treatment with bisphosphonate is warranted. 10 If the corrected serum calcium level is between 2.9 and 3.1 mmol/L (11.5 and 12.5 mg/dL) and the patient is symptomatic, that is, has any of the following symptoms, nausea, vomiting, anorexia, increased urination, constipation, fatigue, depression or mental confusion, treatment with bisphosphonate is also warranted. 10 Corrected serum calcium level that is greater than 3.4 mmol/L (13.5 mg/dL) has life-threatening consequences. 10
Bisphosphonate-induced hypocalcemia
Definition of grades of hypocalcemia according to Common Terminology Criteria for Adverse Events v4.03. 10
Calcium homeostasis
It is important to review how serum calcium homeostasis is maintained in order to understand the risks for developing hypocalcemia from bisphosphonate treatment. It is maintained primarily by the PTH, which is secreted by the parathyroid glands located behind the thyroid glands (Figure 1).
Anatomy of the thyroid and the parathyroid glands. (Printed with permission © 2012 Terese Winslow, LLC, U.S. Govt. has certain rights.)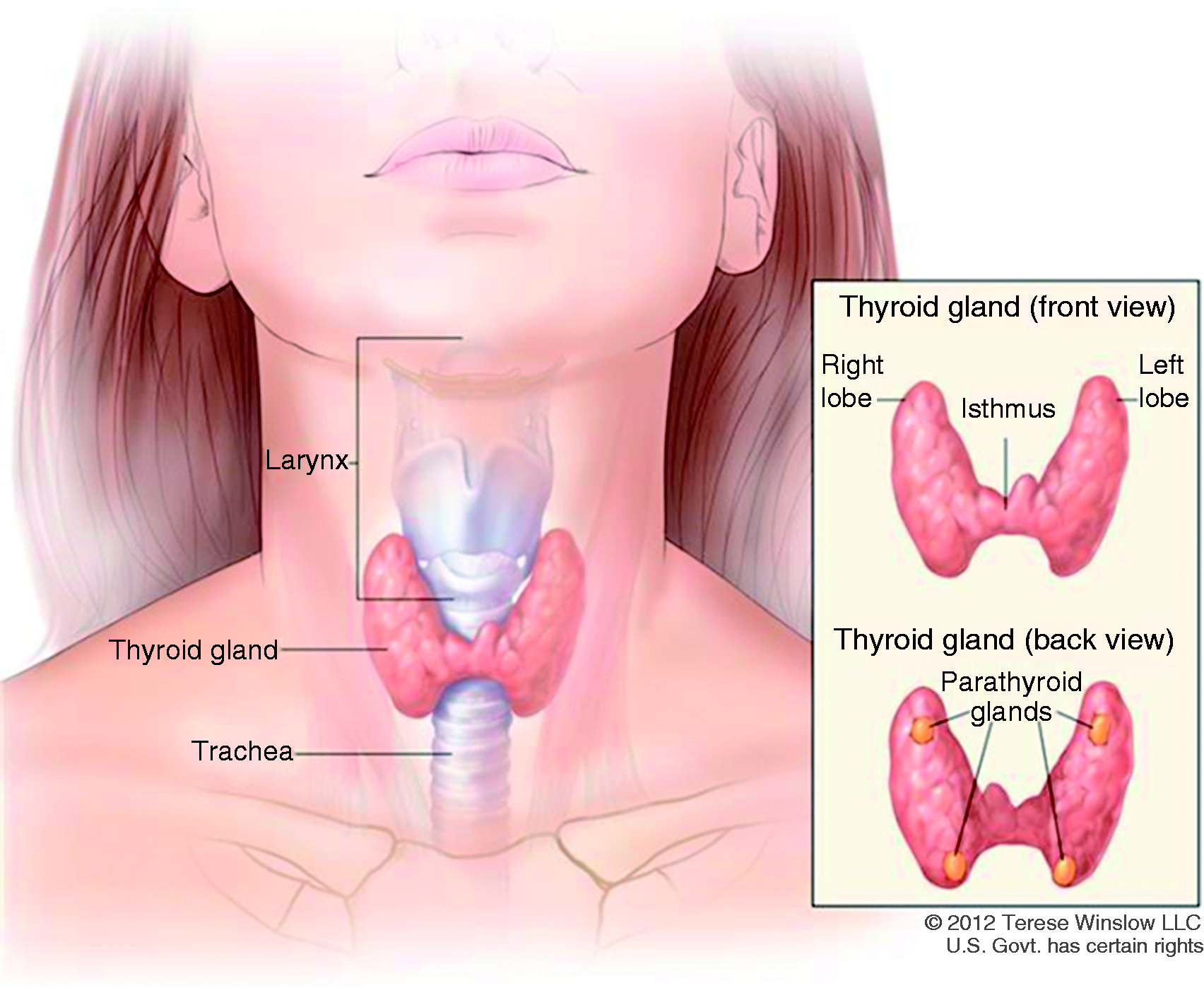
When the serum calcium level is low, the PTH synthesis and secretion are increased, which restores the serum calcium level by three mechanisms: inducing of bone resorption; converting of vitamin D to the physiologically active form, 1,25-dihyrdroxyvitamin D, which increases calcium absorption from the gastrointestinal tract; and enhancing urinary reabsorption of calcium.
9
When the serum calcium level returns to the normal range, it acts as the negative feedback on the parathyroid glands and reduces the synthesis and the secretion of the PTH (Figure 2).
9
Maintenance of calcium homeostasis. (Printed with permission Anna E. Melby, Ph.D., University of Washington.)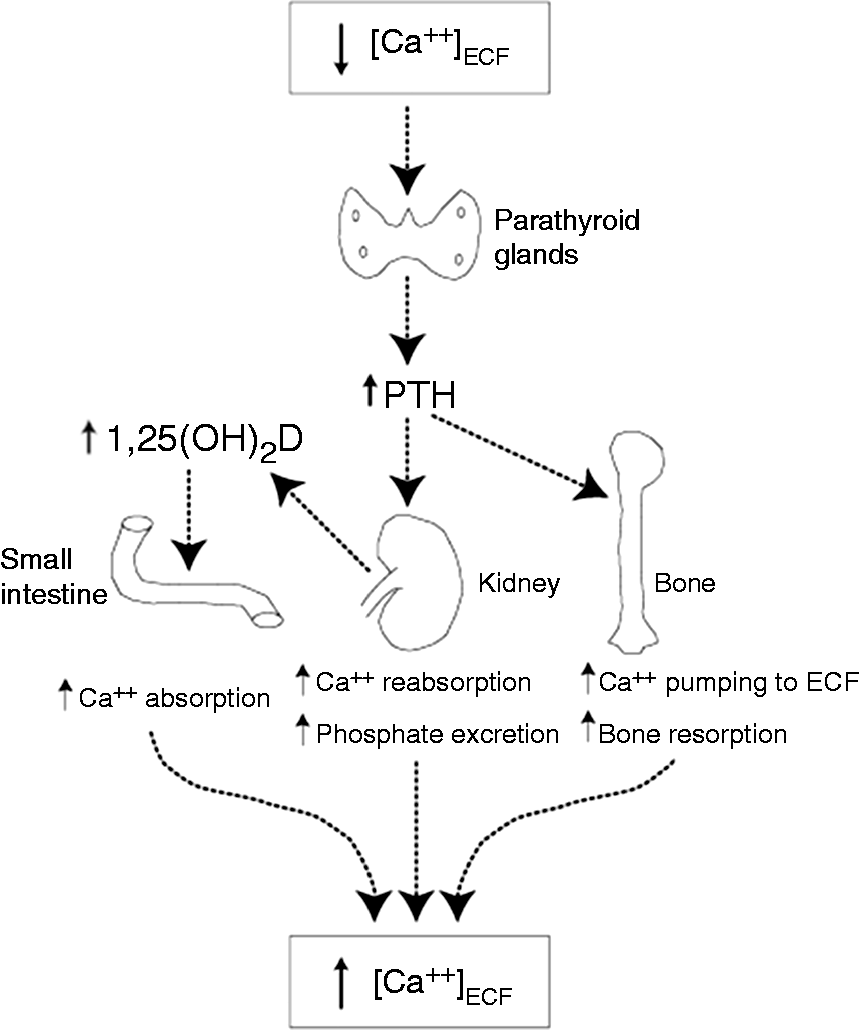
Vitamin D is an essential vitamin that must be obtained from diet or from sun exposure. The dietary source is available in vitamin D2 and D3 forms, and the sun in vitamin D3.
13
Both vitamin D2 and D3 are physiologically inactive and require conversion to the physiologically active form, 1,25-dihydroxyvitamin D, in a two-step process.
13
The first process takes place in the liver and the second process in the proximal tubules of the kidneys (Figure 3).
13
Synthesis and metabolism of vitamin D. (Printed with permission Anna E. Melby, Ph.D., University of Washington.)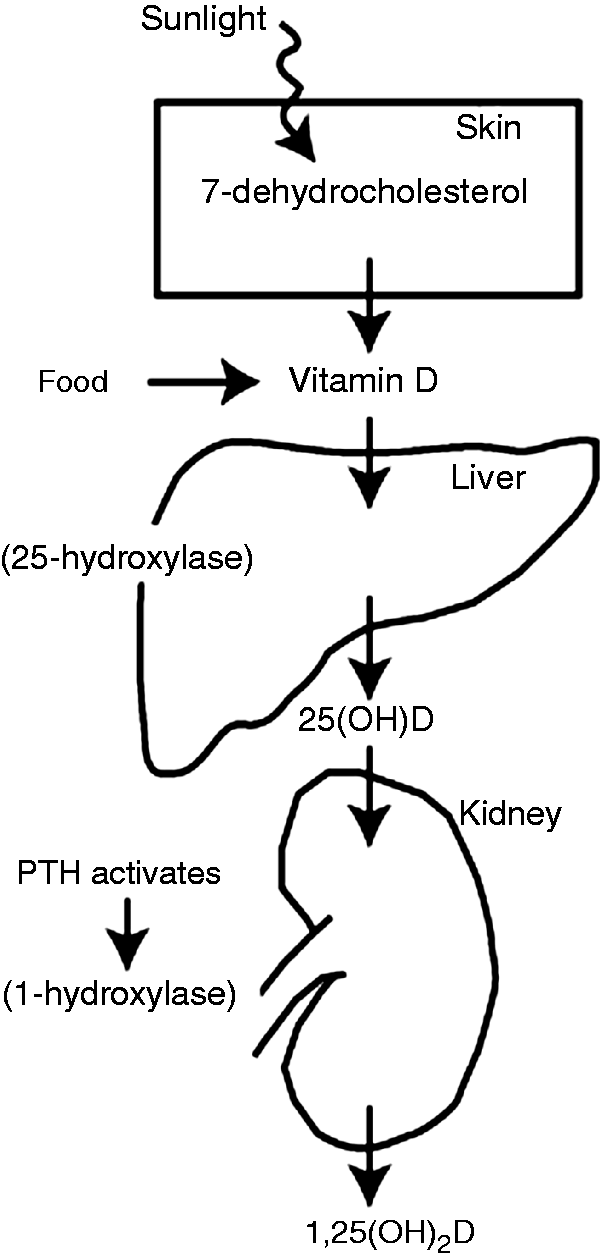
Risks for developing severe hypocalcemia
The risk factors for developing severe hypocalcemia from bisphosphonates have already been established: subclinical parathyroid gland function as a result of previous surgery or radiation treatment to the neck area, vitamin D deficiency, impaired renal function, malabsorption syndromes, malnutrition, severe hypomagnesemia and concomitant use of medications known to cause hypocalcemia.7,8,11 While subclinical parathyroid gland function is the most important risk factor,14,15 vitamin D deficiency has shown to be the most frequent underlying cause of severe hypocalcemia in case reports.
Sixteen case reports of severe hypocalcemia from bisphosphonate treatment in oncology patients were reviewed from literature search, which reported 26 cases.6,16–30 Fifteen of the cases (57.7%) were due to unrecognized vitamin D deficiency; seven cases (26.9%) due to renal dysfunction; four cases (15.3%) due to subclinical hypoparathyroidism; one case due to small bowel resection; one case due to osteoblastic bone lesion and one case due to an unknown reason.
The prevalence of vitamin D deficiency in cancer patients and chronically ill patients is unknown, but is believed to be significant. Vitamin D deficiency is generally defined as 25-OHD level less than 50 nmol/L (<20 ng/mL).31,32 Tangpricha et al. 32 and Wang-Gillam et al. 31 found that up to 50% of the cancer patients they studied, 56 and 21 patients, respectively, had 25-OHD level less than 50 nmol/L.31,32 Thomas et al. 33 found that over 50% of 290 general medicine patients with chronic illness had 25-OHD level < 37.5 nmol/L (<15 ng/mL). 33 Segal et al. 34 found that over 90% of 54 cancer patients had 25-OHD level < 75 nmol/L (<30 ng/mL). 34 In the 26 cases of severe hypocalcemia from bisphosphonate treatment that were reviewed, unrecognized vitamin D deficiency was the underlying cause in 58% of the cases, which is in line with the rate of vitamin D deficiency reported by Wang-Gillam et al. 31 and Tangpricha et al. 32 This represents a significant prevalence of unrecognized vitamin D deficiency in cancer patients.
In this case report, there were many factors that complicated the patient's case. Prior to the cancer diagnosis, he had a history of idiopathic hyponatremia and hypomagnesemia. While he did not report alcohol abuse, he reported consuming a few drinks of wine or beer daily. His nutritional status was unknown. His body mass index ranged between 20 and 21. Following the operation, and prior to commencing chemotherapy treatment, he experienced a number of episodes of electrolyte abnormalities involving calcium, magnesium, phosphates and potassium, which were all correctable. Compliance with his medications was not verified. He had a number of comorbidities, but the kidney function was relatively preserved based on the range of serum creatinine of 81 to 114 μmol/L and the estimated creatinine clearance range of 60 to 98 mL/min using the MDRD equation. There was a slight rise in his serum creatinine while on vorinostat, but it was transient. His home medications were not known to be nephrotoxic or cause hypocalcemia. Ramipril and HCTZ may cause hyperkalemia and hypercalcemia, respectively, but not hypo-. Vorinostat, and to a lesser extent, capecitabine may cause electrolyte abnormalities, and he did experience them, but they were amendable with electrolyte replenishments. There was no known interaction among his home medications and the chemotherapy medications. He had known vitamin D deficiency although the 25-OHD level was not repeated after the calcitriol dose was increased to 0.5 μg twice daily.
It was suspected the patient's parathyroid glands were impaired during total thyroidectomy, which rendered his body unable to maintain calcium homeostasis after one dose of pamidronate dose. When pamidronate was administered, the serum creatinine was 114 μmol/L, with estimated creatinine clearance of 60 mL/min using the MDRD equation. The vitamin D or the PTH level was not done at the time. One month after he had the total thyroidectomy, he was found to have uncorrected serum calcium level of 1.86 mmol/L (7.45 mg/dL). The PTH level at the time was less than 0.3 pmol/L. In patients with normally functioning parathyroid glands, the PTH level is expected to be elevated in the presence of hypocalcemia. 31
Using the Naranjo assessment, a score of six was achieved for this case, which indicates pamidronate probably caused the irreversible, severe hypocalcemia. There was a debate on the other possible causes of the severe hypocalcemia, as he had tendencies to develop hypocalcemia. However, he presented with hypercalcemia prior developing hypocalcemia, which did not fit the previous patterns.
Conclusion
Bisphosphonates are generally safe and effective in the treatment of bone metastases and hypercalcemia of malignancy. The incidence of hypocalcemia from their treatments is rare. In addition, the risk factors for developing severe hypocalcemia are known. However, the risk factors may not be reviewed with equal vigilance in the treatment of hypercalcemia of malignancy as in the treatment of bone metastases due to the goal in the treatment in hypercalcemia of malignancy of reducing the elevated serum calcium level. This case is a reminder that risk factors need to be reviewed irrespective of the goal of the treatment.
Furthermore, the prevalence of unrecognized vitamin D deficiency in cancer patients is becoming evident; especially in those with advanced disease. In the treatment of hypercalcemia of malignancy, there is no dosing guideline for patients with risk factors, and it is not practical to check the 25-OHD level, which takes days for the result. Therefore, in frail patients with advanced cancer, it would be reasonable to administer a reduced dose and monitor the serum calcium level sooner and more frequently. Lastly, it is important to check regularly with patients that they are compliant with all of their medications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.