
Abstract
A 60-year-old Japanese man, with no medical or family history of diabetes, presented with acute-onset type 1 diabetes following nivolumab treatment for advanced non-small-cell lung cancer. During cycle 35 of nivolumab therapy, his glycated hemoglobin level increased from 7.6% to 9.1% in one month. Test results for islet-related and anti-thyroid peroxidase antibodies were negative. A glucagon tolerance test showed insulin dependency. Type 1 diabetes after anti-programmed death-ligand 1 antibody administration is an immune-related adverse event, and numerous reports suggest that fulminant type 1 diabetes can develop in these patients. However, there are few reports of acute-onset type 1 diabetes mellitus.
Introduction
Numerous studies have investigated immune checkpoint inhibitors (ICIs) such as nivolumab and pembrolizumab as immunotherapy agents in several cancers, including non-small-cell lung cancer, melanoma, and renal-cell carcinomas.1–4 ICIs can cause immune-related adverse events (irAEs), especially in the endocrine system, including hypophysitis, hypothyroidism, hyperthyroidism, thyroiditis, adrenal insufficiency, and diabetes.5,6 The National Comprehensive Cancer Network Guidelines in Oncology recently published clinical recommendations for grades 1–4 toxicities related to irAEs. 7 Autoimmune diabetes mellitus (DM) associated with ICI treatment has been reported rarely.8,9 Methods of managing irAEs are also important when considering future use of ICIs to treat patients with other types of carcinoma.
Case report
A 60-year-old Japanese man was diagnosed with stage IVB lung adenocarcinoma (cT4N2M1b) with adrenal metastasis and multiple muscle metastases. His HbA1c was 5.8% before lung cancer treatment, and he had no family history of diabetes or past treatment. His body mass index was 21.8 kg/m 2 (height, 175 cm and weight, 67 kg). He received first-line chemotherapy with cisplatin plus pemetrexed and second-line chemotherapy with gemcitabine plus nanoparticle albumin-bound-paclitaxel, with standard-dose dexamethasone at 6.6 mg/week during each chemotherapy cycle. Dexamethasone was given to control late-onset chemotherapy-related emesis.
Following four courses of second-line chemotherapy, computed tomography showed disease progression (adrenal metastasis progression). Laboratory analysis showed that the patient's HbA1c was 5.3%. His anti-programmed death-ligand 1 (PD-L1) tumor proportion score was 15%, and he received nivolumab (3 mg/kg) every two weeks as third-line therapy. He showed good response to nivolumab therapy (Response Evaluation Criteria in Solid Tumors (RECIST) criteria ver. 1.1: Partial Response), which was continued until cycle 36 (Day 490). Plasma glucose and HbA1c levels gradually increased, and the patient was diagnosed with diabetes according to the American Diabetes Association criteria.
10
Oral diabetes medications, including an alpha-glucosidase inhibitor, biguanide, and dipeptidyl-peptidase 4 inhibitors, were initiated and continued until he later developed insulin dependence. During cycles 35 and 36 of nivolumab administration, the patient showed no symptoms such as thirst, fatigue, polyuria, or weight loss, although his HbA1c level had increased dramatically (7.6% to 9.1%; Fig. 1).
Blood glucose levels and glycated hemoglobin (HbA1c) during nivolumab treatment. Blood glucose levels and HbA1c tended to increase slightly until cycle 34 of nivolumab therapy (Day 456). At cycle 36 of nivolumab therapy (Day 491), hyperglycemia was observed, with rapidly increasing HbA1c. HbA1c: hemoglobin A1C.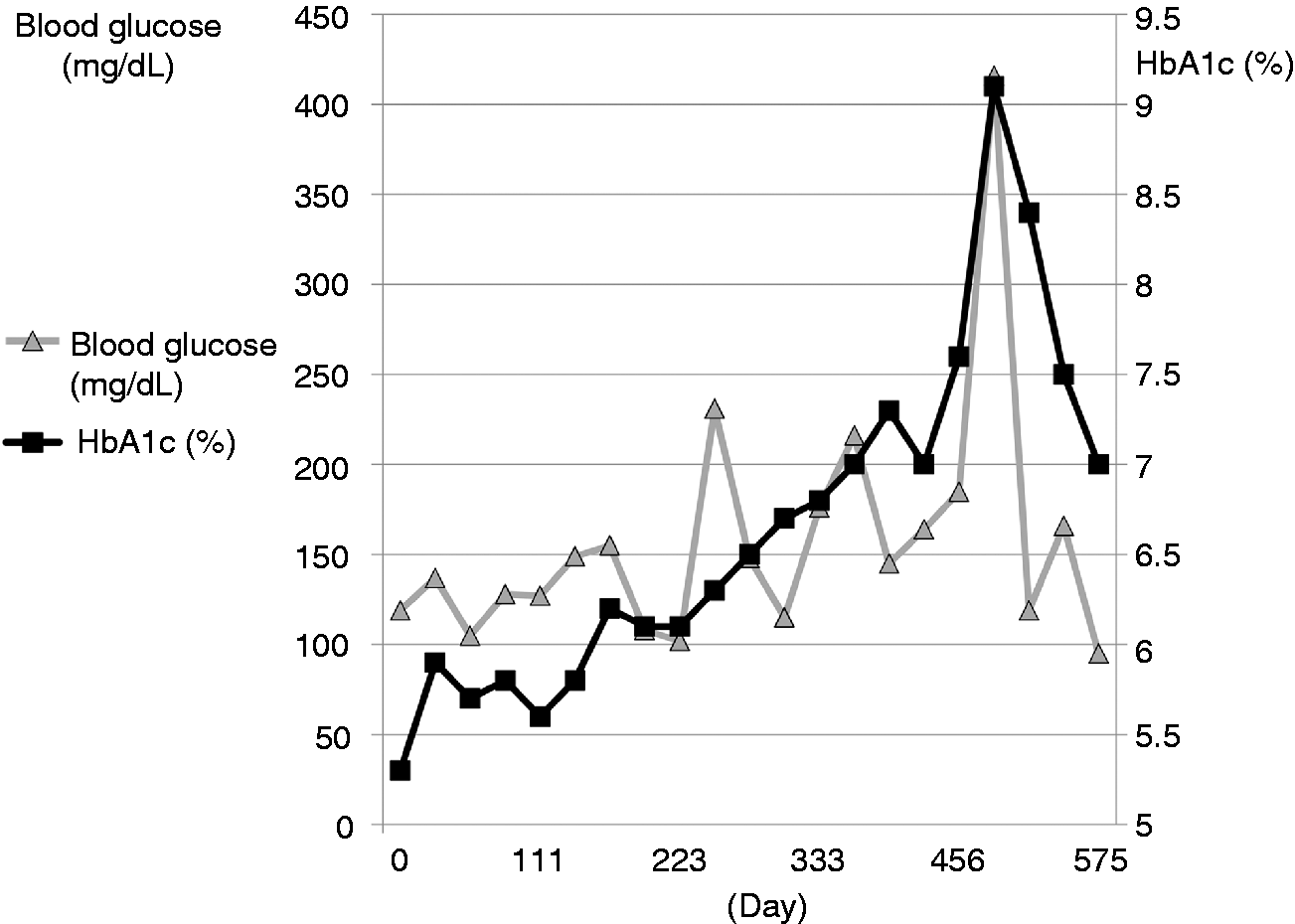
Laboratory test results after the first administration of nivolumab (Day 491).
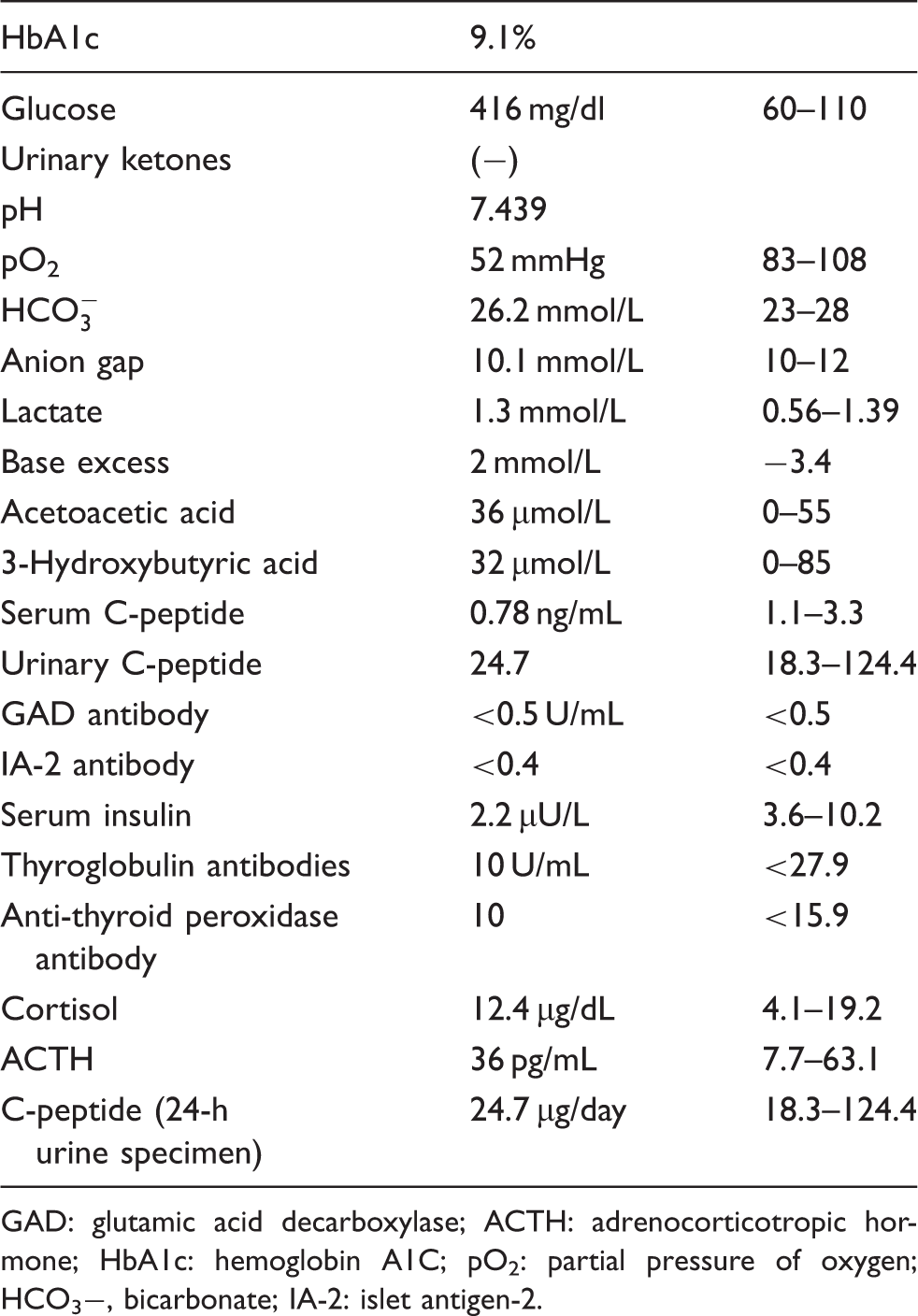
GAD: glutamic acid decarboxylase; ACTH: adrenocorticotropic hormone; HbA1c: hemoglobin A1C; pO2: partial pressure of oxygen; HCO3−, bicarbonate; IA-2: islet antigen-2.
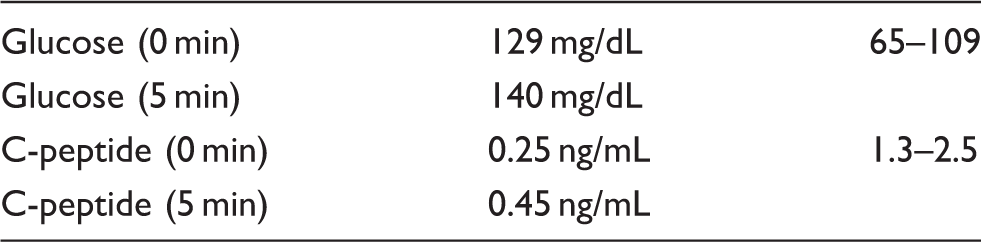
Glucagon stimulation test (Day 498).
Nivolumab administration was reinstituted two weeks later, to maintain the partial response, which was considered to be a therapeutically effective level based on the RECIST response criteria.
Discussion
ICIs are negative regulators of T-cell immune function. Infiltration of T cells into organs causes an immune reaction, resulting in an immune-activation response11,12 that destroys β cells and causes absolute insulin deficiency.
Type 1 diabetes is classified as fulminant, 13 acute-onset, or slow-progressive (known as latent autoimmune diabetes in adults). 14 Some reports discuss the fulminant type, 15 but the acute-onset type is associated with significantly fewer irAEs compared with the fulminant type, which has been reported with ICI therapy in patients with lung cancer and melanoma.16,17 Generally, type 1 diabetes develops with many symptoms such as dry mouth, polydipsia, and polyuria; however, no hyperglycemic symptoms were observed in our patient. Also, results were negative for urine ketones and metabolic ketoacidosis. A possible explanation is that he had visited the clinic as an outpatient every two weeks, which led to early detection of pre-diabetic ketoacidosis that was diagnosed using two of the diagnostic criteria for the acute type: the need for continuous insulin therapy and the presence of endogenous insulin deficiency. 18 The increase in HbA1c did not meet the clinical criteria for the fulminant type, and thus, the patient was diagnosed with the acute type. Acutely, endogenous insulin is reduced but eventually leads to depletion. Anti-GAD and anti-IA-2 antibody test results are usually positive in more than 80% of common acute cases immediately after onset, 18 but patients in whom ICI therapy has caused type 1 diabetes show different trends. Our patient had neither a medical history of obesity nor a family history of diabetes. Also, glycemic tolerance was normal during dexamethasone therapy, and ICI therapy showed good tumor response, suggesting that it was unlikely that he developed type 2 diabetes as a result of disease progression or dexamethasone therapy. Although he had no autoimmune antibody response, including GAD or IA-2 antibody, we could not verify levels of neuronal cell surface marker antibody Zn-8 or insulin auto-antibody, or perform human leukocyte antigen typing, and he rapidly developed severe insulin deficiency during ICI treatment. Our patient required insulin therapy within five months after the treatment of diabetes, suggesting that he had newly developed type 1 diabetes. 19 We also assessed causality between nivolumab and type 1 diabetes using the Naranjo adverse drug reaction probability scale. 20 We obtained a score of 7 for nivolumab with a probable adverse drug reaction score of 5 to 8.
ICI treatment is associated with strong improvement in patient prognosis in numerous cancers.1–4,21 Therefore, the frequency of ICI administration has increased within a short time since its approval. Post-marketing product surveillance is a significant part of assessing irAEs, and this surveillance is both important and ongoing. Continuous treatment suggests a trend toward improved overall survival compared with the one-year treatment arm with nivolumab. 22 Specifically, in advanced non-squamous non-small-cell lung carcinoma (NSCLC) and squamous-cell NSCLC that has progressed during or after platinum-based chemotherapy, overall survival was longer with nivolumab than with docetaxel.1,23 However, the duration of treatment with anti-PD-1/PD-L1 antibody is an important clinical problem that has not yet been clarified. Because ICI treatment results in prolonged overall survival, the number of chronic irAEs is expected to gradually increase.
Severe irAEs necessitate stopping continuous therapy, but treatable irAEs, such as with endocrine system disease, are manageable for most patients, and our patient continued ICI therapy. Signs of systemic disease are often difficult to detect early, especially with nonspecific findings. Adequate treatment of irAEs, such as insulin replacement therapy, enables continuation of ICI therapy; therefore, collaboration between medical departments is also important for early irAE detection.
Footnotes
Acknowledgment
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.