
Abstract
In the late 20th to early 21st century, most new Kaposi’s sarcoma cases were associated with HIV coinfection and low CD4 T-cell counts. After introduction of effective antiretroviral therapy, the clinical and epidemiologic characteristics of Kaposi’s sarcoma may have changed. We analyzed and now report on 27 consecutive Kaposi’s sarcoma patients treated at our institution from 2007 to 2017. Most patients were HIV-positive Caucasian men on antiretroviral therapy; the average CD4 T-cell count was above the AIDS-defining level of 200 cells/mm3. Seven patients had Kaposi’s sarcoma with mucosal involvement, and 20 had skin-only Kaposi’s sarcoma. Mucosal Kaposi’s sarcoma patients had a mean CD4 T-cell count of 83 cells/mm3 as opposed to 381 cells/mm3 for patients with skin-only involvement (p = 0.005). Survival was significantly compromised in both groups but even more so in Kaposi’s sarcoma patients with mucosal involvement (306 vs. 609 days). Along with other reports, our findings suggest that Kaposi’s sarcoma may develop in HIV patients in the modern era despite well-controlled HIV disease. This is significant since Kaposi’s sarcoma remains an important contributor to morbidity and mortality in HIV-infected patients.
Keywords
Introduction
Kaposi’s sarcoma (KS) is a vascular neoplasm caused by human herpesvirus type 8 (HHV-8). KS is further divided into four subtypes: classic, African endemic, iatrogenic, and Acquired Immunodeficiency Syndrome (AIDS) associated. In Human Immunodeficiency Virus (HIV)-infected individuals, KS is the most commonly encountered malignancy and is an AIDS-defining diagnosis. Several other malignancies associated with HIV and for which HHV-8 is etiologic include Castleman’s disease, body cavity lymphoma, and plasmablastic lymphoma. In the U.S., during the early 1990s, patients with AIDS were 20,000 times more likely to develop KS than the general population.1,2 The incidence of KS has since decreased significantly following the advent of antiretroviral therapy (ART). 2
Historically, KS in HIV patients has been associated with low CD4 T-cell counts, with studies showing significantly higher incidence in patients with CD4 T-cell counts less than 200 cells/mm3. 2 In the modern era of effective HIV treatment, however, the clinico-pathologic presentation of this malignancy may have evolved to differ from what has been seen in the past.
Methods and results
To explore this hypothesis, we obtained institutional review board approval to conduct a review and clinico-epidemiologic analysis of consecutive KS patients treated at Eisenhower Medical Center in Rancho Mirage, CA, from 2007 to 2017. Of note, our center serves a population of over 200,000 in Southern California, USA. We identified 27 patients, out of whom 20 identified themselves as Caucasians and seven as Hispanics. The mean age at diagnosis was 48 years; 92% (25/27) patients were male; 84% (21/27) were HIV-positive. 3 For patients with available data, the median time from HIV diagnosis to KS diagnosis was 11 years (range, 1–24). A total of 25.9% (7/27) of patients had mucosal involvement with KS, and the rest had skin-only involvement. Castleman’s disease was identified in 7.4% (2/27) KS patients. We found no cases of body cavity or plasmablastic lymphoma in our cohort. HHV-8 viral load was assessed in only a minority of patients (7.4%) and only at the request of an infectious disease physician.
Significance of associations was assessed via Fisher’s exact test. Two-sample t-tests with homoscedastic variance were used to compare the CD4 T-cell counts and HIV viral load in patients with mucosal versus skin-only involvement.
Clinical characteristics of the KS patient cohort.
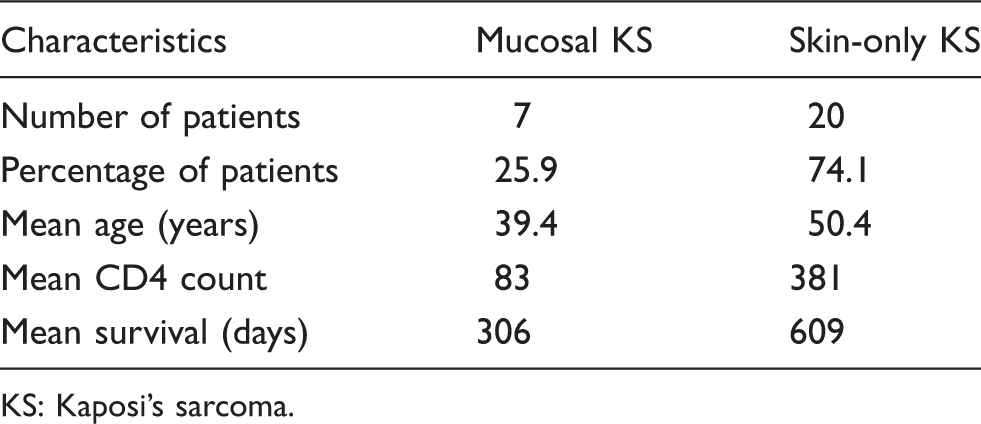
KS: Kaposi’s sarcoma.
A total of seven patients died during the study period. Three of the deceased had mucosal KS involvement, and four had skin-only KS. One patient died as a result of a fatal bleeding due to KS with mucosal involvement. Other deaths occurred as a result of infectious complications, organ failure, or other malignancies. The mean time to death in the patients with mucosal involvement was 306 days compared to 609 days in the patients with skin-only involvement (Table 1). 3
Discussion and conclusions
Importantly, most KS patients in our cohort presented with CD4 T-cell counts well above 200 cells/mm3. Similarly, in a study conducted by the AIDS Malignancy Consortium, 4 31% of KS patients had undetectable HIV viral loads and high CD4 T-cell counts. Yanik et al. 5 concluded that in the modern ART era, the incidence of KS is highest within the first six months of initiating ART but remains at a constant plateau afterwards despite normalization of CD4 T-cell count. These results suggest that patients with controlled HIV infection and CD4 T-cell counts that are not typically associated with opportunistic/AIDS defining illnesses are still at risk of developing KS.
Most commonly, KS manifests as cutaneous lesions involving lower/upper extremities and trunk.6,7 HIV-associated KS differs from other variants in that its clinical course is often aggressive with more widespread lesions and a greater propensity for mucosal involvement. 8 Mucosal involvement itself may vary in its presentation from an isolated oropharyngeal entity to disseminated disease involving pulmonary and gastrointestinal viscera. Mucosal KS frequently is an indicator of advanced disease and is associated with lower CD4 T-cell counts. 9
While the retrospective design of our analysis did not enable us to identify the reasons why some KS patients did undergo treatment and others did not, we assume that these decisions reflected the treating physicians’ and/or patients’ preferences. Several patents had relocated and were lost to follow-up. Radiotherapy and surgery were elected for a limited number of skin lesions, while systemic therapy was elected for multiple skin and/or mucosal lesions. All patients treated with liposomal doxorubicin tolerated therapy fairly well, with no significant treatment delays or grade 3/4 adverse events. All patients responded to liposomal doxorubicin; all responses to chemotherapy were partial. The decreases in CD4 T-cell counts in HIV-infected patients during chemotherapy were minor and transient.
In our cohort, KS patients with mucosal disease and HIV were younger and had lower CD4 counts and more aggressive disease compared to KS patients with HIV with skin-only involvement (Table 1). Although prognosis in this cohort has significantly improved with the introduction of ART, survival is still significantly compromised. In a retrospective study by Laresche et al., 10 mortality due to AIDS-associated KS was 21%, and all diseased patients had visceral/mucosal involvement.
Treatment options for KS range from surgical excision of skin lesions and localized radiation therapy to systemic treatment with agents such as liposomal doxorubicin. Analysis of our cohort showed that nearly half of KS patients did not require specific KS-directed therapy. Some patients only required local therapy. A quarter of our KS patients including all patients with mucosal involvement required systemic chemotherapy. Despite these interventions, severe (and often fatal) mucosal bleeding complicates the disease course. 11 In part, mortality in these patients is increased due to infections or other malignancies. 12
Although KS incidence has drastically declined in recent years, we believe that its occurrence in HIV patients who are on appropriate therapy carries substantial significance. Adherence to effective ART remains the cornerstone intervention for primary and secondary KS prevention; however, well-controlled HIV disease and normal CD4 T-cell counts do not eliminate the risk of developing KS or experiencing disease recurrence. Further investigations of HHV-8 and its genetic expression in KS may provide additional insights as to why this occurs. In addition, studies exploring the role of antiherpetic therapy in combination with ART in terms of preventing HHV-8-associated disease appear warranted. 13 Meanwhile, awareness of the various clinical manifestations of KS and multidisciplinary input from medical and radiation oncology, surgery, dermatology, oncology pharmacy and infectious disease physicians remain paramount for the optimal management of this clinical entity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.