
Abstract
Background
The optimal duration of empiric antimicrobial therapy in febrile neutropenia of unknown origin is unclear. This study evaluated outcomes in autologous and allogeneic hematopoietic cell transplantation recipients with febrile neutropenia of unknown origin who received early de-escalation of broad-spectrum antimicrobials prior to hematopoietic recovery versus those who continued broad-spectrum antimicrobials until hematopoietic recovery.
Methods
A single-center, retrospective study assessed hematopoietic cell transplantation recipients with febrile neutropenia of unknown origin. Patients were categorized into either cohort 1, representing early de-escalation prior to hematopoietic recovery, or cohort 2, representing continuation of broad-spectrum antimicrobials until hematopoietic recovery.
Results
A total of 107 patients were included (22.4% in cohort 1 and 77.6% in cohort 2). Most patients (87.5%) in cohort 1 underwent haploidentical hematopoietic cell transplantation, whereas 84.3% of patients in cohort 2 received autologous hematopoietic cell transplantation. There were no significant differences in rates of recurrent fever (4.2% versus 7.2%, in cohorts 1 and 2, respectively, adjusted odds ratio = 0.84, P = 0.85), re-escalation (4.2% versus 4.8%, adjusted odds ratio = 1.57, P = 0.64), and Clostridioides difficile-associated infections (4.2% versus 2.4%, adjusted odds ratio = 2.27, P = 0.43). No patient experienced in-hospital mortality, intensive care unit admission, or bacteremia.
Conclusion
Hematopoietic cell transplantation recipients with febrile neutropenia of unknown origin in which broad-spectrum antimicrobials were de-escalated prior to hematopoietic recovery did not experience adverse outcomes. These results concur with recently published studies and the Fourth European Conference on Infections in Leukemia guidelines. An early de-escalation approach in haploidentical hematopoietic cell transplantation recipients specifically appears safe and may result in a reduction in antimicrobial utilization.
Keywords
Introduction
Antimicrobial stewardship (AS) has become widely accepted as an essential practice to address the critical issue of antibiotic resistance. In March 2015, the United States White House released the “National Action Plan for Combating Antibiotic-Resistant Bacteria,” which included a goal for all states to incorporate stewardship in healthcare settings by 2020. 1 Despite the increased use of formal stewardship activities in many acute care settings, published data on the safety and efficacy of these methods in immunocompromised patients, particularly hematopoietic cell transplantation (HCT) recipients, remain scarce.
Antimicrobial optimization in HCT recipients has unique challenges due to the level of immunosuppression coupled with difficulties in diagnosis and high risk of mortality.2,3 HCT recipients are susceptible to a wide variety of infections, including bacterial, viral, and fungal infections. With periods of prolonged neutropenia often accompanied by fever, HCT recipients are exposed to numerous antimicrobials for both prophylaxis and treatment. This extensive antimicrobial exposure places patients at risk for developing infections with multidrug resistant organisms (MDROs). Studies have found the rates of MDROs are increasing in patients with hematologic malignancies and have a significant impact on morbidity and mortality.2,4,5 One report found mortality rates as high as 69% in neutropenic patients with carbapenem-resistant Enterobacteriaceae bloodstream infections. 6
Given this growing threat, the treatment of febrile neutropenia (FN) in cancer patients has been targeted as an area for AS by the Infectious Diseases Society of America (IDSA) with a recommendation to develop institution-specific guidelines on management. 7 However, the optimal duration of empiric antimicrobial therapy in FN of unknown origin is unclear.8,9 Recent studies of patients with hematologic malignancies and FN have demonstrated that de-escalation of broad-spectrum antimicrobials (BSA) prior to hematopoietic recovery is associated with greater antimicrobial-free days, but without increased risks, such as recurrent fever, bacteremia, intensive care unit (ICU) admission, or in-hospital mortality. However, the safety of this de-escalation approach has not been extensively studied within the United States as most prior studies were conducted in Europe, and among the studies conducted in the United States, autologous and haploidentical HCT recipients were excluded.10–14 The purpose of this study was to evaluate the outcomes associated with early de-escalation of BSA prior to hematopoietic recovery in autologous and allogeneic HCT recipients with FN of unknown origin.
Methods
Study design
This was a single-center, retrospective study of adult HCT recipients with FN at Carolinas Medical Center, an academic teaching hospital in Charlotte, North Carolina, between March 2014 and April 2018. This study was approved by the site's institutional review board.
Patients were identified via an internal database, and clinical data were obtained from the electronic medical record system. Patients 18 years of age or older who received an autologous or allogeneic HCT for a hematologic malignancy, developed FN (absolute neutrophil count (ANC) < 500 cells/mm3 or expected ANC < 500 cells/mm3 over the next 48 h and a single oral temperature ≥ 38℃ (100.4°F)), and were initiated on BSA for at least 48 h were included. Patients were included only if fever was due to an unknown origin, which was defined as lack of clinical, microbiological, or radiographic diagnosis of active bacterial, fungal, or viral infection (including patients with lone coagulase-negative staphylococcus species blood cultures, but excluding cytomegalovirus reactivation or BK virus). Patients could be included more than once if they received more than one transplant, but only the first episode of FN following each transplant was included in the evaluation. Chronic neutropenia lasting over 90 days since transplant, fevers ( ≥ 38℃ (100.4°F)) persisting more than five days from initial fever episode, and death within 48 h of FN diagnosis were criteria for exclusion. Patients were also excluded if they were receiving BSA prior to the FN episode.
Donor source, conditioning regimen, and graft-versus-host disease (GVHD) prophylaxis were selected according to institutional standard operating procedures. Standard GVHD prophylaxis for haploidentical HCT consisted of cyclophosphamide 50 mg/kg on days + 3 and +4, tacrolimus on days +5 through + 180, and mycophenolate mofetil on days +5 through + 35. All patients received antimicrobial prophylaxis (levofloxacin or a third-generation cephalosporin if unable to receive a fluoroquinolone) from day −1 until start of intravenous (IV) empiric BSA or hematopoietic recovery. Broad-spectrum therapy was initiated according to the institutional standard operating procedure and included an extended-infusion (EI) antipseudomonal beta-lactam (cefepime, piperacillin-tazobactam, or meropenem), or aztreonam if drug allergy, given alone or in combination with an agent with expanded Gram-positive coverage (vancomycin, daptomycin, or linezolid) and/or an aminoglycoside (tobramycin) or fluoroquinolone (ciprofloxacin). Following IDSA guidelines, indications for addition of a Gram-positive agent included: hemodynamic instability or other evidence of severe sepsis, pneumonia, suspected catheter-related infection, skin or soft-tissue infection, colonization with methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus, or penicillin-resistant Streptococcus pneumoniae, severe mucositis (if fluoroquinolone prophylaxis given and ceftazidime employed as empiric therapy), or selection of aztreonam as the antipseudomonal agent.
Eligible patients were categorized into one of two cohorts based on the time of de-escalation or discontinuation of BSA (Figure 1). Cohort 1 (early de-escalation) represented patients who were de-escalated from BSA to prophylactic antimicrobials prior to hematopoietic recovery (first day of ANC ≥ 500 cells/mm3 for three consecutive days). Cohort 2 (hematopoietic recovery de-escalation) represented patients who continued BSA until hematopoietic recovery. All patients had defervesced (absence of a temperature ≥ 38℃ (100.4°F) for at least 48 h) at the time of antimicrobial de-escalation or discontinuation. The decision to de-escalate BSA prior to hematopoietic recovery was based on the hematology–oncology attending physician's discretion in discussion with the rounding team consisting of an advanced care practitioner and an oncology-trained clinical pharmacist. Moreover, our institution has a robust AS program in which infectious diseases/AS clinical pharmacists are available for assistance with optimizing antimicrobial regimens and providing recommendations to consider de-escalation of BSA after discussion with an infectious diseases attending physician.
Summary of study design. BSA: broad-spectrum antimicrobials; FN: febrile neutropenia; HCT: hematopoietic cell transplantation.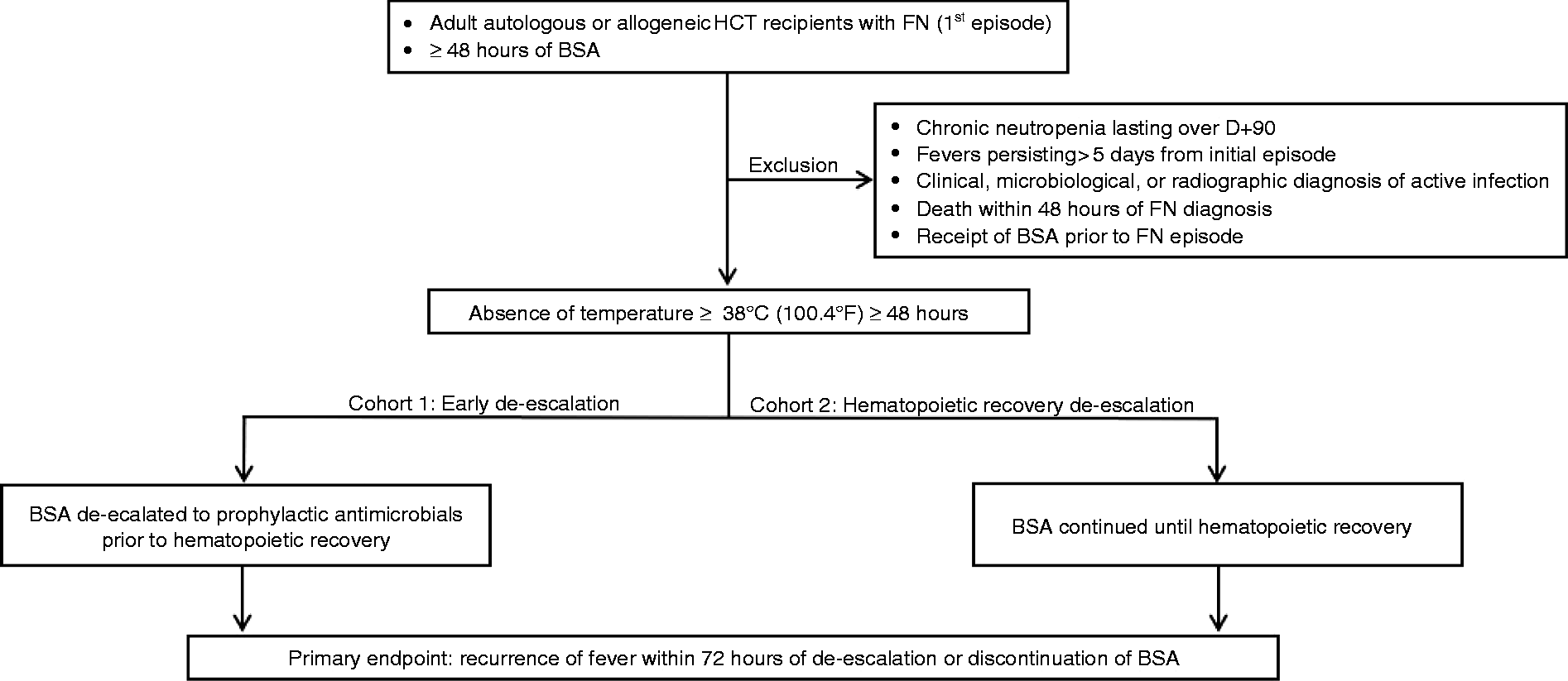
Outcomes
The primary endpoint was the rate of recurrent fever (single fever ≥ 38℃ (100.4°F)) within 72 h of de-escalation or discontinuation of BSA. The selection of the 72 h time frame was based on previous studies in order to avoid inclusion of fever or re-escalation of antimicrobials due to infectious or noninfectious causes unrelated to the original neutropenic fever episode.13,14 Secondary endpoints included rates of re-escalation of BSA, ICU admission, and bacteremia within 72 h following de-escalation or discontinuation of BSA, Clostridioides difficile-associated infections (CDI) within 30 days from hematopoietic recovery, and in-hospital mortality.
Antimicrobial use was measured using days of therapy (DOT), defined as the aggregate sum of the days of exposure for which a specific antimicrobial was administered. 15 Antimicrobial costs were based on group purchasing organization pricing at the time of data analysis and calculated with the assumption that every patient received a standard dosing regimen for normal renal function as follows: EI cefepime 2 g IV every 8 h, EI piperacillin-tazobactam 4.5 g IV every 8 h, EI meropenem 500 mg IV every 6 h, aztreonam 2 g IV every 6 h, vancomycin 1 g IV every 12 h (using weight of 70 kg), daptomycin 500 mg IV every 24 h (approximately 7 mg/kg using weight of 70 kg), and linezolid 600 mg IV every 12 h. Costs were the aggregate sum of the cost per day multiplied by the duration of therapy for every antimicrobial administered in each patient during the FN episode.
Statistical analysis
Baseline characteristics were compared using a descriptive statistical analysis. Fisher's exact test was conducted for categorical variables, while Mann–Whitney U test was employed for continuous variables. A multivariate logistic regression model adjusted for gender, race, and age was utilized to determine adjusted odds ratios (AORs) to evaluate rates of recurrent fever, re-escalation of therapy, and CDI between the two cohorts. A Firth's penalized-likelihood estimate was used to reduce small-sample bias given low event rates. Corresponding P-values and 95% confidence intervals were determined by Wald chi-square test. A two-tailed P-value of < 0.05 was considered statistically significant. All statistical analyses were performed using Base SAS® 9.4.
Results
Baseline characteristics.
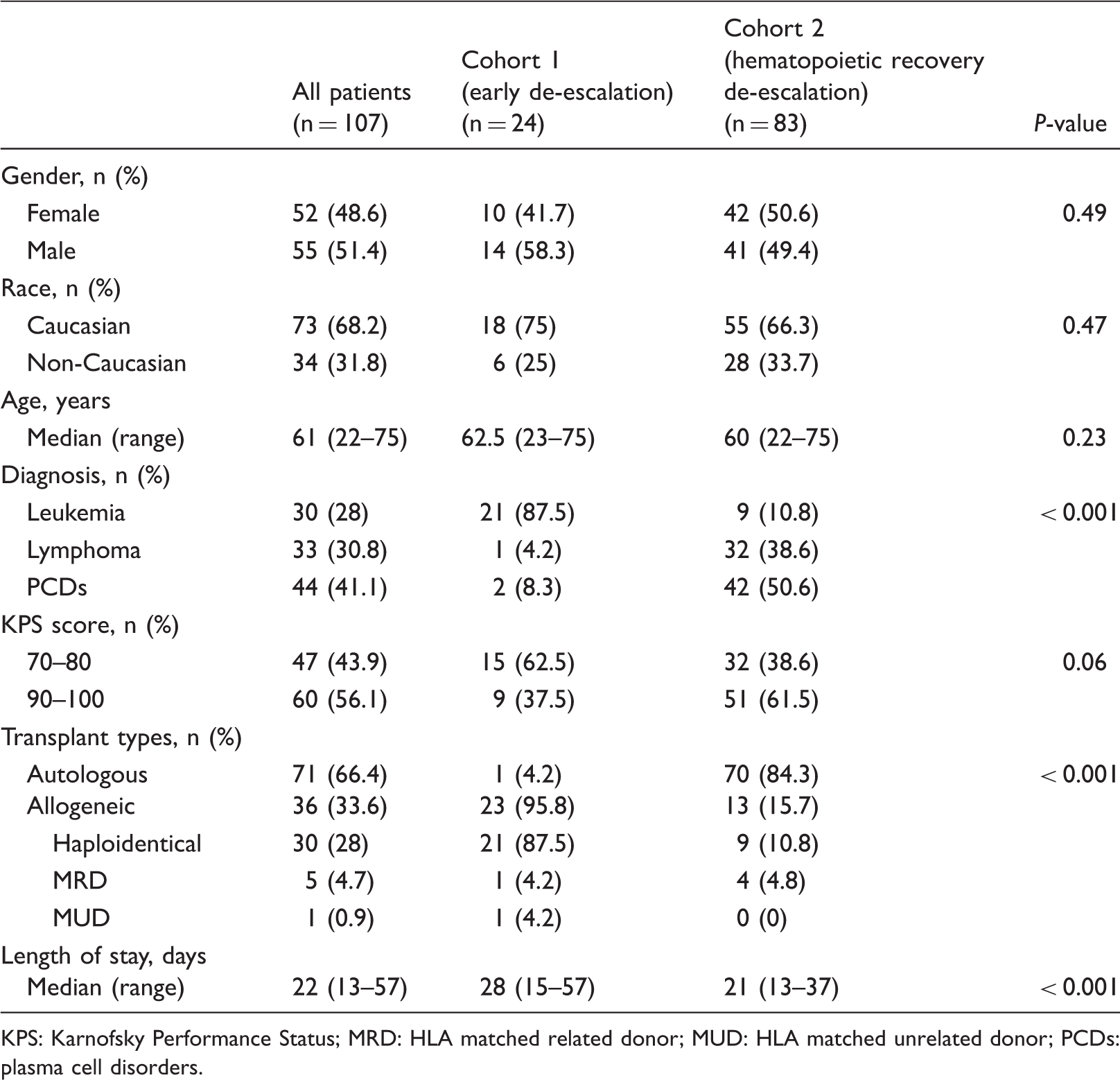
KPS: Karnofsky Performance Status; MRD: HLA matched related donor; MUD: HLA matched unrelated donor; PCDs: plasma cell disorders.
Febrile neutropenia-associated characteristics.
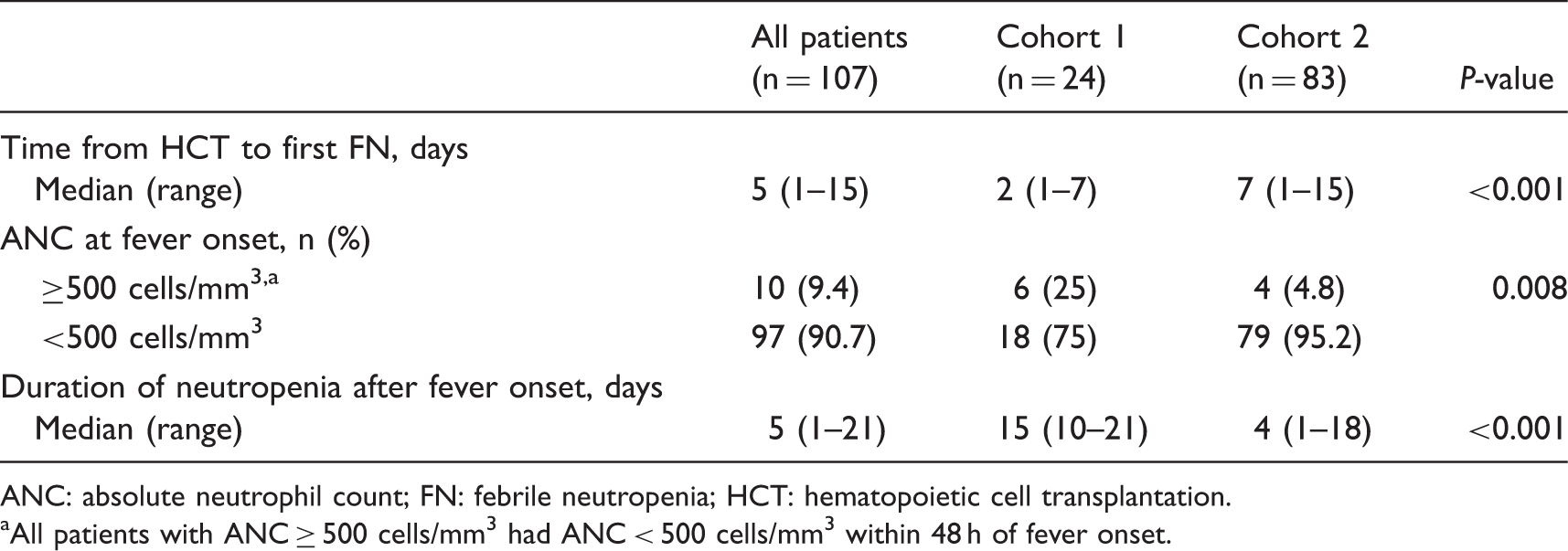
ANC: absolute neutrophil count; FN: febrile neutropenia; HCT: hematopoietic cell transplantation.
All patients with ANC ≥ 500 cells/mm3 had ANC < 500 cells/mm3 within 48 h of fever onset.
Primary and secondary endpoints. a
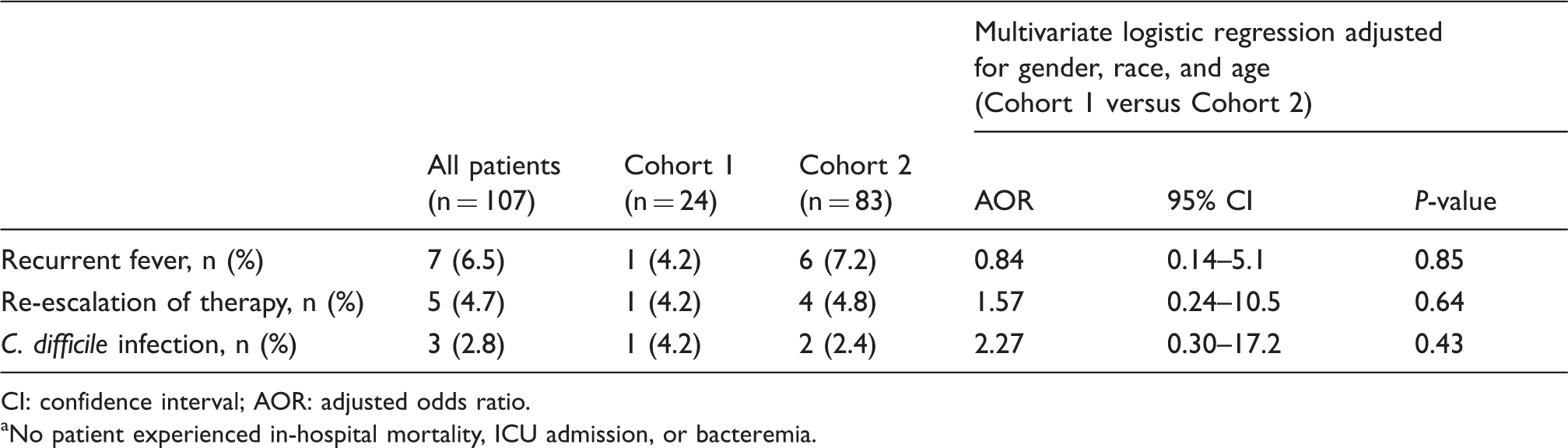
CI: confidence interval; AOR: adjusted odds ratio.
No patient experienced in-hospital mortality, ICU admission, or bacteremia.
Broad-spectrum antimicrobial use and cost outcomes.
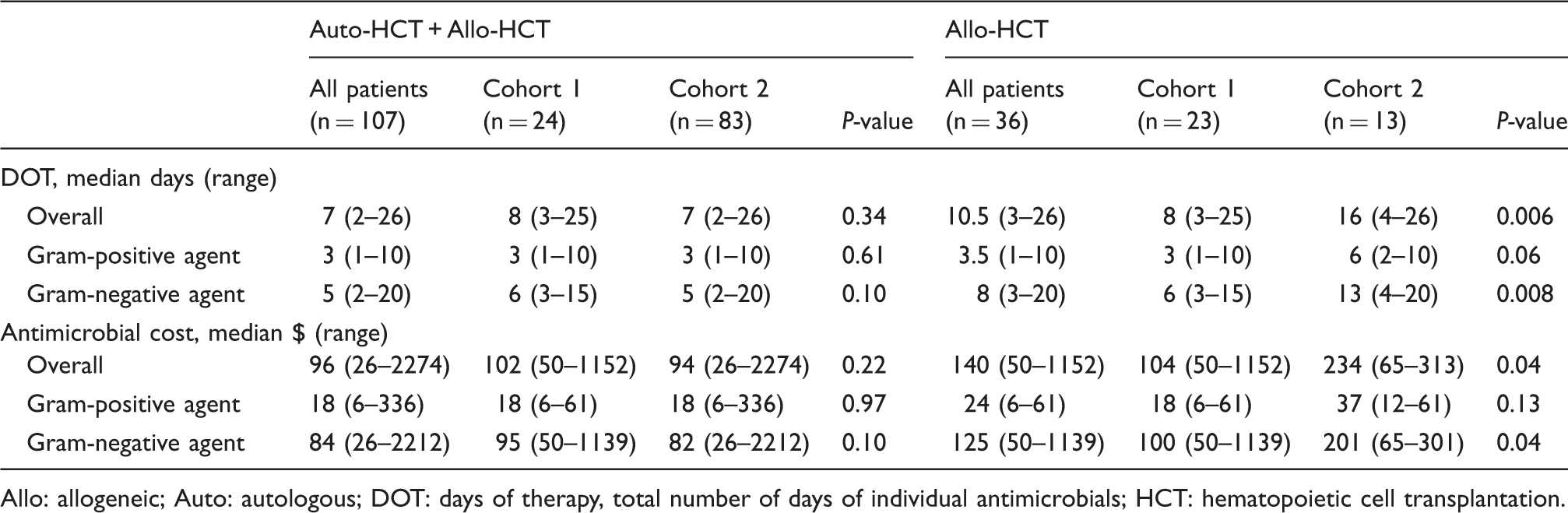
Allo: allogeneic; Auto: autologous; DOT: days of therapy, total number of days of individual antimicrobials; HCT: hematopoietic cell transplantation.
In a subgroup analysis of only allogeneic HCT recipients (n = 23 in cohort 1 and n = 13 in cohort 2), haploidentical was the most common transplant type with 21 (91.3%) in cohort 1 and 9 (69.2%) in cohort 2 (Table 1). The median time from HCT to fever onset in haploidentical HCT recipients was one day in both cohorts (range 1–4 days). Recurrent fever was only observed in one allogeneic HCT recipient in cohort 1, whereas no allogeneic HCT recipients in cohort 2 experienced a recurrence of fever (P > 0.999). Significant reductions in BSA use were observed in cohort 1 compared to cohort 2 in terms of overall DOT (8 versus 16 days, P = 0.006) and Gram-negative DOT (6 versus 13 days, P = 0.008). Similarly, overall BSA cost ($104 versus $234, P = 0.04) and Gram-negative cost ($100 versus $201, P = 0.04) were significantly lower in cohort 1 compared to cohort 2 (Table 4).
Discussion
This retrospective study demonstrates that de-escalation of BSA prior to hematopoietic recovery in haploidentical HCT recipients with FN of unknown origin is safe without resulting in higher rates of recurrent fever, re-escalation of therapy, CDI, bacteremia, ICU admission, and in-hospital mortality. Extrapolation to other types of allogeneic and autologous HCT recipients is limited given that the majority of patients who received early de-escalation of BSA in this study were haploidentical HCT recipients.
Summary of previous trials evaluating early de-escalation in patients with febrile neutropenia.
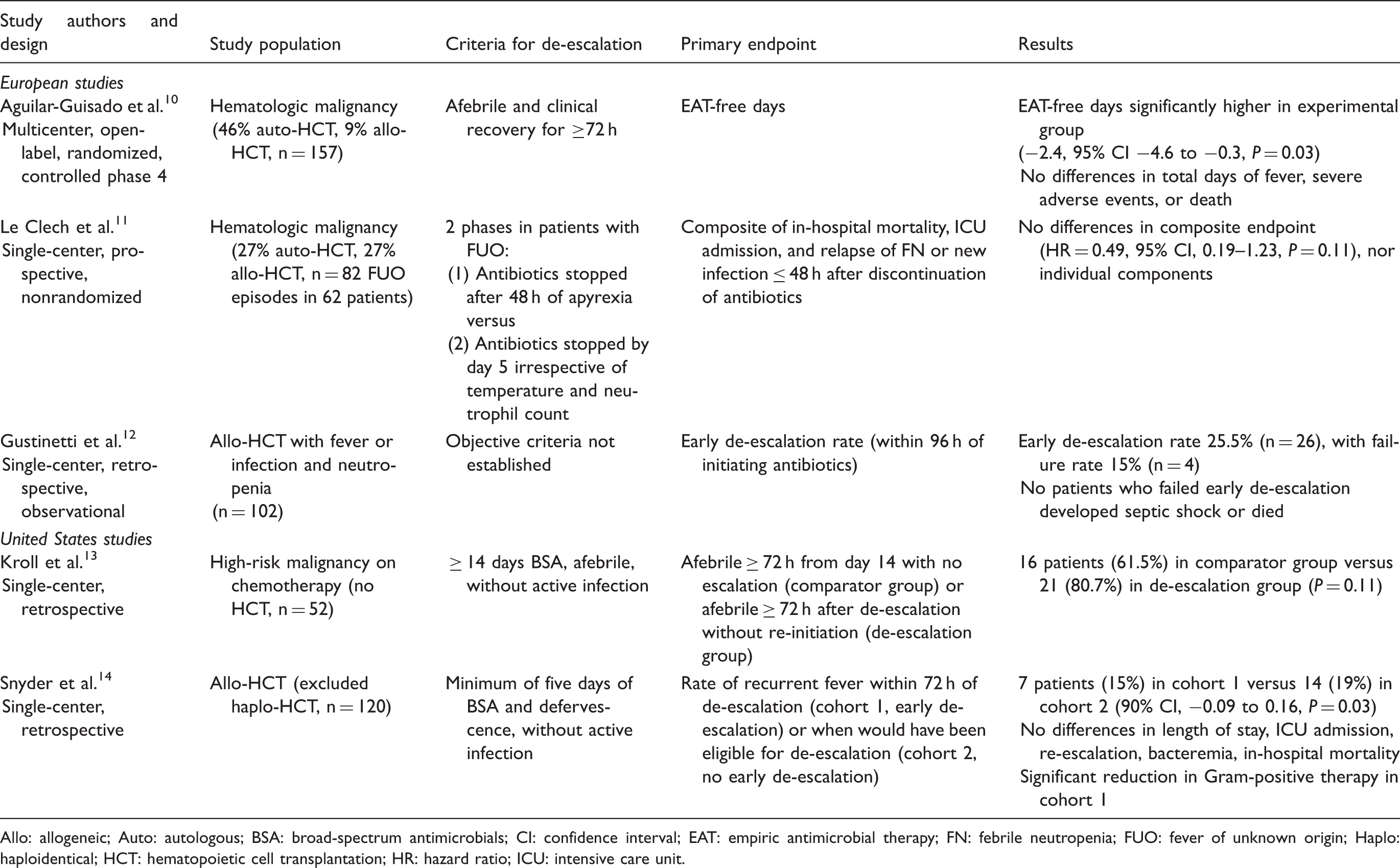
Allo: allogeneic; Auto: autologous; BSA: broad-spectrum antimicrobials; CI: confidence interval; EAT: empiric antimicrobial therapy; FN: febrile neutropenia; FUO: fever of unknown origin; Haplo: haploidentical; HCT: hematopoietic cell transplantation; HR: hazard ratio; ICU: intensive care unit.
In this study, indications for addition of a Gram-positive agent were based on the IDSA guidelines. However, given increasing vancomycin resistance, the most recent National Comprehensive Cancer Network's (NCCN) guidelines, along with recommendations from the Hospital Infection Control Practices Advisory Committee of the Centers for Disease Control and Prevention, emphasize the judicious use of vancomycin only in patients at high risk for serious Gram-positive infection and should not be considered as a routine component of initial therapy for fever and neutropenia.16,17 In contrast to the IDSA guidelines, the NCCN guidelines do not include pneumonia as an indication for the addition of vancomycin and place a strong emphasis against the routine addition of vancomycin for mucositis. If empiric vancomycin is initiated, the NCCN guidelines recommend reassessment within two to three days of initiation, and if no resistant Gram-positive pathogen is identified, vancomycin should be discontinued. In light of these recent recommendations and the growing threat of vancomycin resistance, updates to our institutional guidelines will be considered to reduce the use of vancomycin in patients with FN.
Limitations of this study include its single-center, retrospective study design and the imbalanced distribution of transplant types between the two cohorts, in which the early de-escalation group (cohort 1) and hematopoietic recovery group (cohort 2) consisted of mostly allogeneic and autologous HCT recipients, respectively. Patients were included in cohort 1 if, based on physician discretion, BSA were de-escalated prior to hematopoietic recovery which introduces potential selection bias. Physicians are likely more inclined to de-escalate in haploidentical HCT recipients as fevers following stem cell infusion in this population are commonly associated with the cytokine release syndrome, rather than an infectious etiology.18,19 The greater composition of autologous HCT recipients in cohort 2 may be attributed to physician preference to continue BSA as fevers in this population often occur just prior to hematopoietic recovery. Although BSA were continued until hematopoietic recovery in most autologous HCT recipients in this study, prior studies have demonstrated an early de-escalation approach is safe in this population.11,12 Nonetheless, further study in large, prospective, randomized trials to confirm these findings is warranted. The results of this study also did not show that an early de-escalation approach reduces LOS. On the contrary, LOS was significantly longer in cohort 1 compared to cohort 2. However, given that the majority of patients in cohort 1 consisted of allogeneic HCT recipients, this is an expected finding given that allogeneic HCT recipients typically have longer hospital admissions than autologous HCT recipients. Lastly, antimicrobial use data were limited as costs were estimated based on the assumption that a standard dosing regimen in a patient with normal renal function was used rather than evaluating the actual dose administered in each patient. A comparison of antimicrobial-free days was unable to be performed as the time frame for collecting antimicrobial administration data was within 72 h of de-escalation or discontinuation and therefore did not capture re-escalation of therapy. However, in the study by Snyder et al., 14 early de-escalation resulted in significant reductions in Gram-positive BSA utilization, with trends toward lower use of broad-spectrum Gram-negative agents and associated costs.
Despite these limitations, the results of this study, along with prior studies, highlight the importance of collaboration between an AS program and the primary transplant team in optimizing antimicrobial use in order to minimize collateral damage including the possible development of multidrug resistance, in a population as vulnerable as HCT recipients. A strategy of early antimicrobial de-escalation in HCT recipients with FN of unknown origin will be incorporated into AS initiatives at our institution through our recent implementation of “handshake stewardship,” which involves communication of interventions in person by a pharmacist–physician team and has been shown to result in decreased antimicrobial use in a pediatric patient population. 20 With a large proportion of haploidentical HCT recipients at our institution who typically have prolonged and profound neutropenia post-transplant, this practice has the potential to be of most benefit in this patient population through a reduction in antimicrobial use and cost. Moreover, an interesting area for further research would be to evaluate the impact of an early de-escalation approach on intestinal microbiota composition and complications such as GVHD in allogeneic HCT recipients.
Conclusion
An early de-escalation approach in haploidentical HCT recipients with FN of unknown origin appears safe and may result in a reduction in antimicrobial use. Further study is warranted in other types of HCT recipients. Promotion of this practice through AS programs is imperative in the fight against antimicrobial resistance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.