
Abstract
Introduction
Anti-angiogenic treatment in adjunct with chemotherapy is widely used for the treatment of various cancers. These agents inhibit vascular endothelial growth factor (VEGF) signaling thereby inhibiting tumor proliferation and invasion. Dysphonia, or voice changes, has been documented, but is an underreported side effect of anti-angiogenic agents. We report a case of intermittent dysphonia in a patient with metastatic, platinum-refractory ovarian cancer treated with bevacizumab.
Case report
A 48-year-old female with high grade mixed type ovarian adenocarcinoma and concurrent left sided breast cancer was transitioned to palliative therapy with gemcitabine-bevacizumab for her ovarian cancer. At a follow-up visit after three cycles of the new therapy, the patient complained of intermittent changes in her voice, describing periods of hoarseness or softness in her voice after the chemotherapy—sometimes to the point that her voice was inaudible.
Management and outcome: A new pelvic thrombus was discovered upon assessment of the patient’s disease. Bevacizumab was held and she was referred to ear, nose, and throat evaluation for dysphonia. Laryngoscopic examination showed normal vocal cord, with normal movements and no lesion or necrosis. During subsequent follow-up, the patient reported improvement in her voice with no additional dysphonia.
Discussion
Vocal adverse effects of anti-VEGF agents have been documented in landmark trials and case reports; however, clinicians are often unaware of this rare side effect. Although VEGF-induced dysphonia may be rare and may not impede the patient’s quality of life in some cases, it is critical to acknowledge and not underestimate this adverse effect.
Introduction
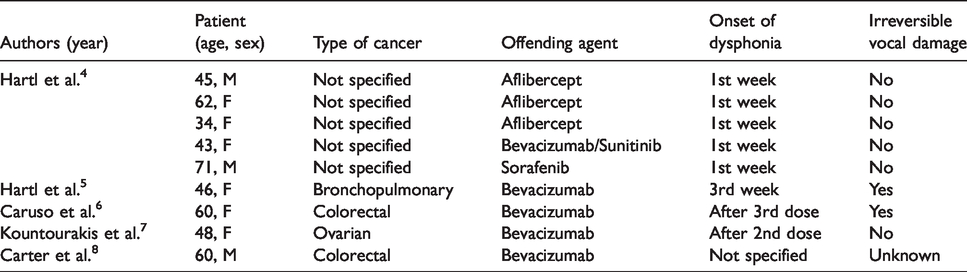
Bevacizumab is a monoclonal antibody that inhibits vascular endothelial growth factor (VEGF). It is widely used as an adjunct to chemotherapy for the treatment of multiple different cancers including colorectal, ovarian, cervical, breast, and renal cell carcinoma. 1 The inhibition of VEGF leads to controlling or slowing the proliferation of tumors which require angiogenesis for survival. Bevacizumab has been shown to cause hypertension, proteinuria, impaired wound healing, diarrhea, thromboembolic events, gastrointestinal perforation, bleeding, and hemorrhage.2,3 Dysphonia, or voice changes, is a known but less documented side effect of anti-angiogenic treatments like bevacizumab. Previous documented case reports related to VEGF inhibitor-induced dysphonia are summarized in Table 1.4–8 Additionally, reports of bevacizumab-related dysphonia are summarized in Table 2. 9 Dysphonia has been documented with other anti-VEGF agents, such as sunitinib, sorafenib, pazopanib, axitinib, and regorafenib.4,7,9,10 Here, we present a case of dysphonia without anatomical changes from bevacizumab in a patient with metastatic, platinum-refractory ovarian cancer.
Reports of bevacizumab-related dysphonia. 4-14
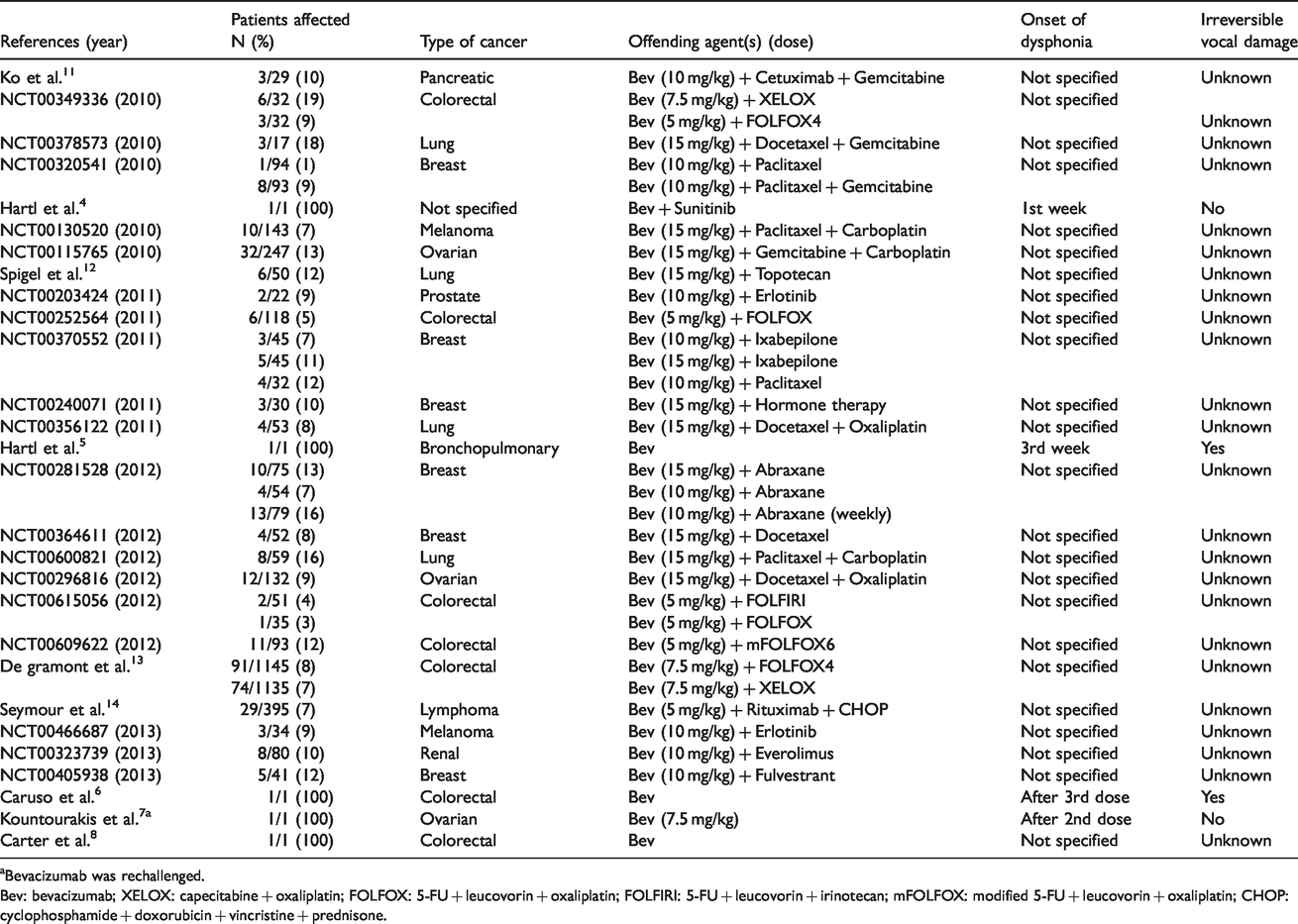
aBevacizumab was rechallenged.
Bev: bevacizumab; XELOX: capecitabine + oxaliplatin; FOLFOX: 5-FU + leucovorin + oxaliplatin; FOLFIRI: 5-FU + leucovorin + irinotecan; mFOLFOX: modified 5-FU + leucovorin + oxaliplatin; CHOP: cyclophosphamide + doxorubicin + vincristine + prednisone.
Case report
A 48-year-old female patient with no medical history was found to have a large right-sided ovarian mass with peritoneal implant and subsequently diagnosed with high-grade mixed type ovarian cancer. She was also found to have concurrent left-sided ER/PR/HER2 neu-positive breast cancer. She was started on paclitaxel-carboplatin-trastuzumab-pertuzumab chemotherapy. Interval imaging after three cycles showed a good response after which the patient underwent interval debulking surgery for the ovarian mass. Trastuzumab and pertuzumab were continued during the surgery. Carboplatin and paclitaxel were continued five weeks after surgery once the incision had healed and patient had recovered. Patient completed three additional cycles of chemotherapy. Following completion of six cycles of therapy, she had repeat imaging that showed progression of disease with multiple new peritoneal implants and pelvic lymph node, consistent with platinum-refractory disease. She was then transitioned to palliative therapy with gemcitabine-bevacizumab for her ovarian cancer. Trastuzumab was continued for her HER2 neu-positive breast cancer during this time.
At a follow-up visit after three cycles of gemcitabine-bevacizumab, the patient complained of intermittent changes in her voice. She described periods of hoarseness or softness in her voice after the chemotherapy—sometimes to the point that her voice was inaudible, usually after the chemotherapy, lasting for two days. The patient denied stridor, pain or difficulty in breathing during this episode. The symptoms improved days after chemotherapy. She was otherwise doing well. Physical examination was unremarkable, and imaging studies were ordered, with plan to continue the treatment as she was responding well.
Management and outcome
Imaging studies showed stability of the peritoneal implants and lymph nodes. Scans of neck area were normal with no obvious mass or lymphadenopathy. She was, however, found to have a new pelvic thrombus. Bevacizumab was held and she was referred to ear, nose, and throat evaluation for dysphonia. Laryngoscopic examination showed normal vocal cord, with normal movements and no lesion or necrosis. During subsequent follow-up, the patient reported improvement in her voice with no additional dysphonia. The probability of bevacizumab causing dysphonia is calculated in Table 3.
Naranjo adverse drug reaction probability scale. 15
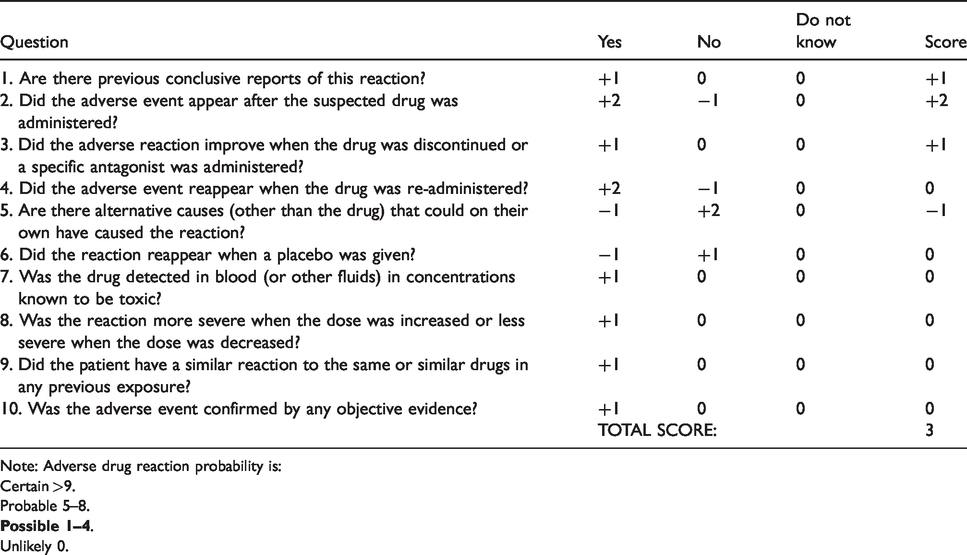
Note: Adverse drug reaction probability is:
Certain >9.
Probable 5–8.
Unlikely 0.
Discussion
We described a patient experiencing bevacizumab-associated dysphonia. While most adverse effects of anti-angiogenic agents present as a “class effect” due the downstream effects of inhibiting the VEGF pathway, dysphonia is a much-underreported side effect. A 2012 report by Hartl et al. 5 explains that these effects are due to the loss of capillary density to the vessels vascularizing the mucosa found in the superficial lamina propria, which are required for vibration in order to produce voice. Previous studies have also linked laryngeal adverse effects to VEGF inhibition. Saavedra et al.’s review evaluated the incidence of dysphonia or voice changes in the phase I, II, and III clinical trials for all the VEGF inhibitors, and found that dysphonia was more associated with aflibercept (VEGF-trap) and the oral anti-angiogenic small molecule tyrosine kinase inhibitors (TKIs) like axitinib, regorafenib, and sorafenib. 9
This patient experienced dysphonia secondary to bevacizumab after three cycles, which falls in the time frame that has been previously described with bevacizumab and other anti-VEGF inhibitors. Bevacizumab-induced dysphonia has been described to occur as early as the first week of treatment up to the third cycle.4,6,7 Furthermore, our patient’s laryngoscopic examination did not show any anatomical changes, which is usually the case for VEGF-related dysphonia.
Although the vocal effects of anti-VEGF agents have been documented in landmark trials as well as a few case reports, clinicians are often unaware of this rare adverse effect. In most reported cases, the dysphonia was reversible upon discontinuation or completion of treatment; however, two cases involved permanent vocal loss with damage leading to laryngeal necrosis.5,6 In our case, the dysphonia resolved upon discontinuation of the bevacizumab. Therefore, although VEGF-induced dysphonia may be rare and may not impede the patient’s quality of life in some cases, it is critical for clinicians to acknowledge and not underestimate this adverse effect.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.