
Abstract
Purpose
The goal of this survey was to identify opportunities for health systems to increase implementation and adoption of oncology-focused pharmacogenomics services.
Methods
An online survey assessing respondent demographics, baseline knowledge and training in pharmacogenomics, comfort level with pharmacogenomic data, and challenges of implementing clinical pharmacogenomic platforms was distributed to professional colleagues and over national oncology pharmacy listservs. Pharmacists were grouped based on their comfort level with pharmacogenomic data. Results were analyzed utilizing Pearson chi-square test. A p value of <0.05 was considered significant.
Results
A total of 84 participants from 58 cancer centers participated in the survey. Most participants were post-graduate year 2 trained and a majority reported being comfortable assessing oncology pharmacogenomic data. Respondents indicated that pharmacogenomics reported within the electronic medical record was the most common institutional process to support pharmacogenomics for oncology patients. Despite this, poor visibility of pharmacogenomics within the electronic medical record was the most challenging aspect of implementing a pharmacogenomic program. Additional challenges included lack of resources for pharmacogenomic programs, insurance denials for pharmacogenomic-driven testing and medication, and prolonged turnaround time of pharmacogenetic results. Length of practice, post-graduate year 2 residency training, institutions with pharmacist involvement on hematology/oncology molecular tumor board, and institutions where a pharmacist helped create local pharmacogenomic policies were significantly associated with respondents’ comfortability in assessing pharmacogenomics.
Conclusion
Oncology pharmacists reported substantial challenges in implementing a pharmacogenomic program. Future efforts to assist in developing pharmacogenomic efforts should focus on increasing pharmacist involvement, expanding education and training, and improving clinical decision support tools.
Background
Pharmacogenomics have become prevalent within healthcare and are driving treatment decisions at an increasing pace, especially within oncology patient populations. Over the last 20 years, 42 mutation-targeted medications have been approved for the treatment of various hematologic and oncologic diseases. 1 Complex coordination among the medical team is required when determining the best treatment option for the patient, which now includes ordering necessary genomic tests and assessing the clinical utility of any mutations. American Society of Health-System Pharmacists (ASHP) recently encouraged pharmacists to become leaders in clinical pharmacogenomic efforts. 2 This direction included assisted ordering of pharmacogenomic tests, assessing results and interpretations, and implementation of optimized therapy in collaboration with the medical team. Since this initiative, there have been successful reports of implementing pharmacists into various pharmacogenomic programs;3–6 however, there are still many barriers to successfully incorporate pharmacogenomics into every day clinical practice.
Pharmacogenomics clinical impact in recent years has grown significantly faster than clinical practice infrastructure to support its use. This rapid growth is predicted to continue as the Precision Medicine Initiative, a key part of the United States 21st Century Cures Act, will allocate up to $1.455 billion over 10 years to advancing patient care in this field. 7 The sheer volume of genetic information has yielded one of the largest challenges for clinicians as, for example, the National Cancer Institute’s (NCI) Cancer Genome Atlas alone has generated over 2.5 petabytes of genomic, epigenomic, transcriptomic, and proteomic data, which is currently being used clinically to diagnose, treat, and prevent cancer. 8
There are very few pharmacist pharmacogenomics specialists and training programs in the United States. It has been noted that pharmacy schools are not providing sufficient pharmacogenomics education to provide graduate comfort level with the practice. 9 There remains only two pharmacogenomics pharmacy residency positions nationwide of over 1300 specialty training options, despite a 65% growth rate of specialty pharmacy residency positions from 2014 to 2019. 10 Post-doctoral fellowship training options also continue to be limited; however, a positive step occurred in 2019 as four additional National Human Genome Research Institute funded positions were allotted, the first such increase since 2014.11 This allotment reflects that the growing need for pharmacogenomic specialists and institutions across the nation is encouraged to follow the National Human Genome Research Institutes’ lead.
While acknowledging the excellent leadership and skill of many pharmacists nationwide, implementation and expansion of robust pharmacogenomic programs will be challenging at many health systems for the foreseeable future. Front-line pharmacy staff, who may not be comfortable assessing pharmacogenomics, will be increasingly faced with questions regarding a genetic mutation’s impact on patient care. Pharmacists’ traditional pride in being the most accessible clinicians will be diminished without widespread implementation of pharmacogenomics expertise. Here, we undertook a survey of current state of pharmacogenomics practice with an aim to define opportunities that health systems can assess to increase implementation and adoption of pharmacogenomics services.
Methods
A work group consisting of two oncology clinical pharmacists, an oncology pharmacy informatics pharmacist, and a post-graduate year (PGY)-1 pharmacy resident was formed. The survey group worked to develop a validated online survey using design, conceptualization, drafting, and testing methodology from the University of Wisconsin’s Survey Center. An online survey generator, Qualtrics, was utilized to assist with creating the survey. Qualtrics provides the end user with a multitude of different question types including multiple choice, matrix, and open-ended styles. It also has the capability of running statistical analyses on the data obtained and determining how the survey created may be perceived by participants. Ultimately, this survey comprised of 12 questions and was created via Qualtrics (https://uwmadison.co1.qualtrics.com/jfe/form/SV_9RiHxOEUIayoTw9). After release, survey responses were validated to ensure completeness and comprehensiveness after 10 responses and then again after 20 responses. The overall goal of this survey was to assess pharmacogenomic training of oncology pharmacists, measure the role of pharmacists within pharmacogenomic practices, and define the current state of pharmacogenomic program implementation. This survey was distributed to the American College of Clinical Pharmacy’s Hematology/Oncology Practice and Research Network and Vizient University Health System Consortium’s Cancer Care listservs as well as through personal communication with professional pharmacy colleagues. Participants were given two weeks to complete the survey. After this period, the survey was distributed to PGY-2 oncology pharmacy residency program directors at NCI designated cancer centers who had not yet completed the survey. An additional two weeks were allotted to complete the survey.
Results of the survey were analyzed with SPSS version 24.0 (Statistical Package for the Social Sciences, Chicago, IL). Pharmacists were grouped based on their comfort levels with the following variables: next-generation sequence panels, cytogenetics, molecular genetic tests, and genetic-driven protein biomarkers. Pharmacists were classified as comfortable if they reported being comfortable or very comfortable with three or more of these variables. Those who were comfortable with two or less of these variables were classified as not comfortable. To further assess participants comfort level in assessing pharmacogenomic data, binary results were analyzed for length of time in oncology practice, highest level of post-graduate training, dedicated pharmacy full-time employment (FTE) to pharmacogenomics at their institution, pharmacist involvement on molecular tumor board (MTB), and pharmacist involvement on creating internal pharmacogenomic policies. Additionally, a composite score of challenges with implementing a pharmacogenomic program was calculated using the sum of challenging or very challenging responses to variation in utilization and interpretation of pharmacogenomic results, complicated inventory management, difficulties in multidisciplinary coordination, prolonged turnaround time of genetic results, insurance denials of gene-targeted medications, lack of dedicated pharmacogenomic resources, and poor pharmacogenomic visibility within the medical record. Composite scores were then assessed to determine whether there was a difference for any of the following: dedicated pharmacy FTE to pharmacogenomics at their institution, pharmacist involvement on MTBs, and pharmacist involvement on creating internal pharmacogenomic policies. Statistical analyses performed included Pearson chi-square test. A p value of <0.05 was considered significant. All other results were analyzed descriptively. For institutions with multiple respondents, institutional processes were considered present if reported by at least one respondent.
Results
A total of 84 participants from 58 health systems participated in the survey, including 21 of 63 (33%) NCI designated cancer centers and 16 of 28 (57%) National Comprehensive Cancer Network (NCCN) cancer centers. Survey responses came from 29 of 50 (58%) states representing all regions of the country. Pharmacists had a wide range of practice experience and most (61%) were PGY-2 trained. Additionally, most (71%) have an MTB at their institution and a pharmacist participates on about two-thirds of these. Three-quarters of respondents reported that their institutions currently have pharmacogenomic reports displayed in the electronic medical record (EMR), which represented the most common institutional process supporting pharmacogenomics. Additionally, 60% of pharmacists indicated that internal pharmacogenomic policies existed. There were low rates of clinical decision support tools, pharmacogenomic patient communication portals, and pharmacogenomic specialty modules in the EMR (Table 1). Participants indicated that they have received pharmacogenomic training in a variety of settings with the most common being on the job (76%) followed by continuing education (64%) and pharmacy school (42%). A complete overview of participants’ previous pharmacogenomic training is available in Table 2.
Current institutional processes in place to support pharmacogenomics (n = 58).

Previous pharmacogenomic training (n = 84).
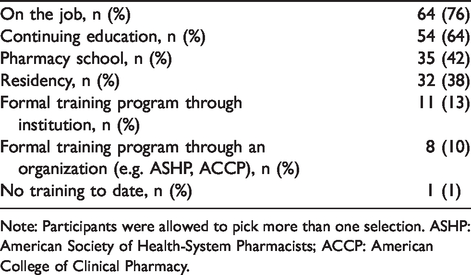
Note: Participants were allowed to pick more than one selection. ASHP: American Society of Health-System Pharmacists; ACCP: American College of Clinical Pharmacy.
Participants indicated that they were comfortable with nearly all pharmacogenomic data (Figure 1). Fifty-seven percent of participants reported being comfortable with three or more pharmacogenomic data. Participants were the most comfortable with genetic-driven protein biomarkers, such as breast cancer gene 1/2 (BRCA1/2) and programmed death-ligand 1 (PD-L1) (78% comfortable). Participants were the least comfortable with next-generation sequencing panels (49% comfortable). As outlined in Table 3, pharmacists who practiced in oncology for more than 10 years (p = 0.02), completed PGY-2 or fellowship training in oncology (p = 0.04), reported pharmacist involvement on the MTB at their institution (p = 0.01), or reported pharmacist involvement in creating internal pharmacogenomic policies (p = 0.02) were significantly more comfortable with pharmacogenomic data. Pharmacists who practice at institutions with dedicated FTE to pharmacogenomics also had a substantially higher comfort rate with pharmacogenomic data.
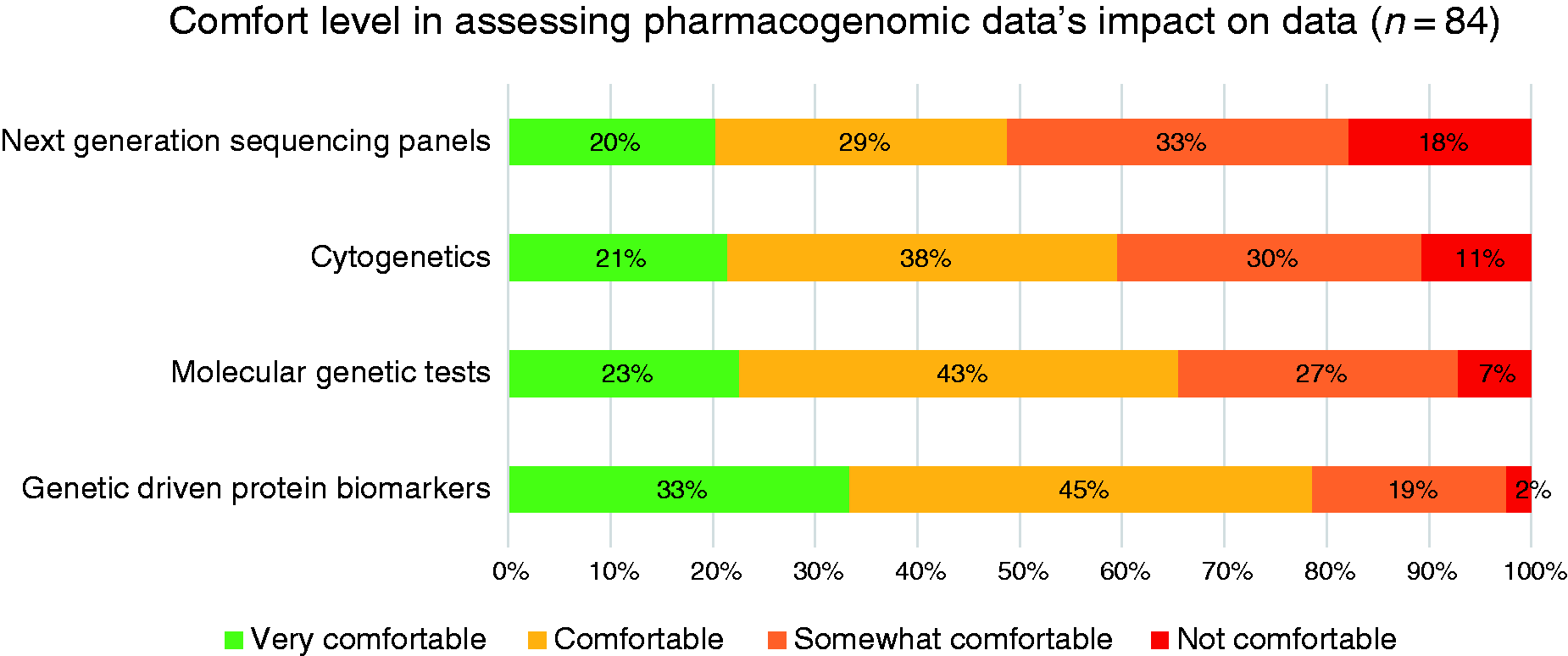
Comfort level in assessing pharmacogenomic data’s impact on treatment.
Association with comfort level in assessing pharmacogenomic data.

Note: FTE: full-time employment; MTB: molecular tumor board; PGY: post-graduate year.
Survey respondents noted that there are significant challenges in implementing a pharmacogenomic program (Figure 2). Poor visibility of pharmacogenomic information within the EMR was cited as the most challenging aspect (64% challenging or very challenging). The least challenging aspects reported were variation in utilization and interpretation of pharmacogenomic testing and inventory management for low use pharmacogenomic-driven medications (both variables: 32% challenging or very challenging). As reported in Table 4, pharmacists in health systems without FTE dedicated to pharmacogenomics noted significantly more difficulty as 55% of composite pharmacogenomic implementation responses were challenging/very challenging versus only 28% for those with FTE (p = 0.001). Those who practice at institutions where pharmacists were not involved in creating internal pharmacogenomic policies also reported more difficulty (38% vs. 52%, p = 0.001).
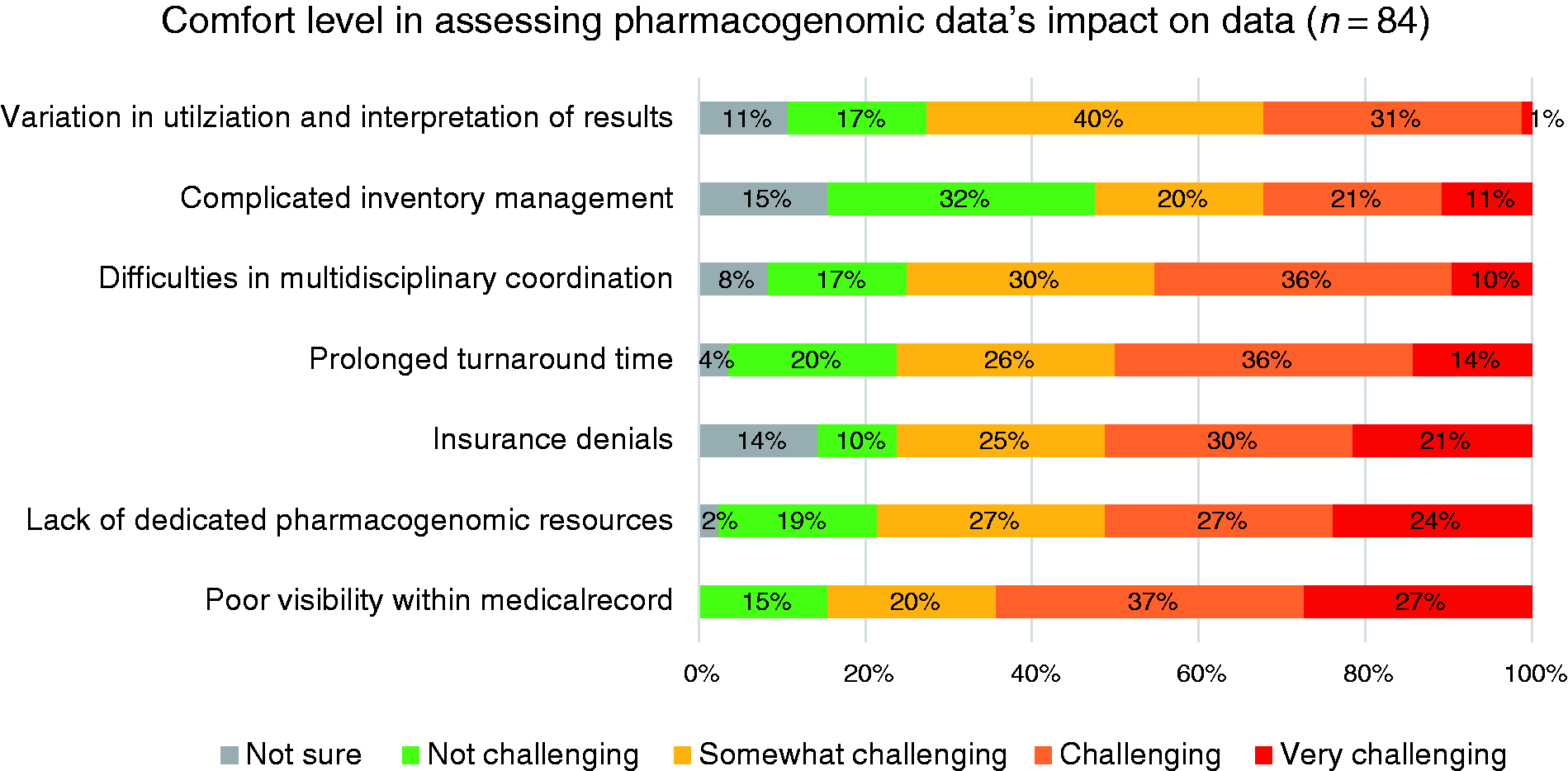
Challenges related to pharmacogenomic program implementation.
Composite score of challenges in implementing pharmacogenomic program.
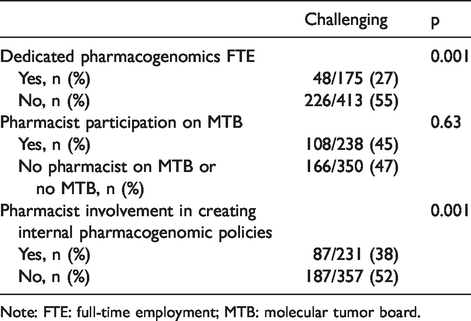
Note: FTE: full-time employment; MTB: molecular tumor board.
Discussion
As displayed by the results of this survey, implementation of a pharmacogenomic program within oncology has many challenges. These include lack of clinical decision support tools to assist clinicians’ application of pharmacogenomic information, prolonged turnaround time of genetic results, insurance denials of pharmacogenomic-driven medications, and the visibility of pharmacogenomic results within the EMR. These represent a significant barrier to providing optimal care for patients as clinicians may unknowingly miss, unintentionally disregard, or misinterpret pharmacogenomic information. Pharmacists are currently assisting in key roles to help overcome many of these issues as part of multidisciplinary efforts.
Oncology pharmacists who have practiced for greater than 10 years were more likely to be comfortable assessing pharmacogenomic data. Differences in clinician demographics were also reported in a recent survey conducted by Freedman et al. among physician oncologists, which demonstrated that those between the ages of 30 and 39 years were most likely to utilize pharmacogenomics in practice. 12 Our finding regarding pharmacists with greater than 10 years of experience suggests that pharmacists’ pharmacogenomic education has largely come from work experience. Pharmacists with PGY-2 or fellowship training in oncology were also more comfortable assessing pharmacogenomic results indicating that this has become a focus of post-graduate oncology training. 12 Although rates of pharmacogenomic education have increased in pharmacy schools across the nation, 13 fourth-year pharmacy students have reported that they are not confident utilizing pharmacogenetic data when they begin to practice. 9
There is recent precedent for rapid adoption of a new healthcare paradigm in the setting of low numbers of trained specialists. Similar to pharmacogenomics now, a scarce number of pharmacy informatics specialists were available to support the rapid adoption of EMRs. 10 From 2006 to 2016, pharmacists reported health system EMR adoption improved from 38.1 to 99.1%. 14 This initiative was also driven by federal money with almost $2 billion in funding provided via the Health Information Technology for Economic and Clinical Health Act of 2009. 15 A possible reason for the lack of clinical pharmacogenomics residency growth is difficulty in obtaining funding and in allotment of enough preceptors to establish a credentialed curriculum. 16 It is imperative for pharmacogenomic specialists to share the value they provide to patient care with health system leadership so that future pharmacogenomic programs are established. In the absence of more pharmacogenomics residencies and fellowships, genomics training should be incorporated widely into all pharmacy residency training programs with robust supporting goals and objectives. Pharmacy schools should at a minimum dedicate multiple lectures to pharmacogenomics and provide training on continuously updated pharmacogenomic resources such as the Clinical Pharmacogenetics Implementation Consortium (CPIC), PharmGKB, and the Food and Drug Administration to insure all new graduates understand how to utilize these to interpret pharmacogenomic results.1,17,18
As expected, pharmacist comfort level with pharmacogenomic practice is higher if their institution has pharmacists serving on MTBs or creating local pharmacogenomics policies (Table 3). Pharmacists in health systems without FTE dedicated to pharmacogenomics noted significantly more difficulty with almost double the amount of challenging/very challenging pharmacogenomic implementation responses compared to those with FTE. Interestingly, MTB presence alone did not decrease the composite of challenging encounters associated with implementing a pharmacogenomic program. This could be because some MTBs are currently constructed with more experts to determine genomic drivers of disease and therapy recommendation than on therapy procurement and implementation. Multiple published MTB reports cite problems not with genomic interpretation and patient-specific therapy recommendations but with patients actually starting a recommended targeted medication therapy.19,20 Of the institutions included in this survey, only 66% reported pharmacist involvement on MTBs. Pharmacy departments are well positioned to assist with third-party insurance approvals, medication access programs, specialty pharmacy procurement, pharmaceutical clinical trial support, and literature evaluation to support potential off-label drug gene targets.6,21 Our survey suggests that initiatives to decrease significant challenges with insurance approvals would be especially impactful on promoting pharmacogenomics adoption. Standardized pharmacogenomics prior authorization paperwork across third-party payors would be helpful.
Respondents at institutions where pharmacists contributed to local pharmacogenomic policies also reported fewer challenges with pharmacogenomic implementation, but creation of this content is time-consuming and difficult. Our health system’s acute myeloid leukemia pharmacogenomic document required five meetings and dozens of emails with three hematologists, two pathologists, two pharmacists, a nurse case manager, an evidence-based medicine policy expert, and an administrative policy member. 22 National guideline bodies such as the NCCN must continue to be leaders on pharmacogenomic guidance and are encouraged to standardize their pharmacogenomic recommendation grading, include pharmacists on their panels, and find a mechanism to cite disease-specific pharmacogenomic database tools with clear notation regarding their regulatory status. Pharmacists reported that their lowest comfort level was with next-generation sequencing, and guideline bodies are encouraged to educate and inform clinicians on this pharmacogenomics platform.
Despite being the most commonly available institutional process to support pharmacogenomics, participants in this study reported pharmacogenomic result visibility as the most challenging aspect of pharmacogenomic implementation with 64% of respondents noting this aspect as challenging/very challenging. The most recent widely influential ASHP Pharmacy Forecast strategic planning publication argues that EMR pharmacy leaders should support improving pharmacogenomic pharmacy informatics infrastructure. 23 Examples of clinical decision support programs from Bielinski et al. and Owusu-Obeng et al. have described methods to create pop-up alerts that are linked to actionable orders and/or additional information regarding the pharmacogenomic results.5,24 Efforts moving forward should incorporate design for broad scalability given the increasing reach of pharmacogenomic impact. At UW Health, pharmacists have begun using a standardized oncology pharmacogenomics flowsheet that allows documentation of a patient’s genetic results from a multitude of sources in a single visible EMR location. Anecdotally, this flowsheet has improved efficiency of cycle-to-cycle treatment verification, tracking of mutation-driven medication use for research and budgetary planning, documentation of prior authorization requests, and decreased time spent writing progress notes given genomic data prepopulating functionality. Institutions should explore what options are available within their EMR and determine what is best for their current workflows. Genomic modules within EMRs also have potential to improve many issues described though adoption rates are currently low at this time with 9% of institutions reporting use. Genomic module adoption rates might also benefit from a variation of “meaningful use like” regulation and potentially fines to EMR vendors for those not meeting information transfer and interoperability standards. 25
There are several limitations with this survey. First, only 58 institutions were represented, which may not reflect the pharmacy practice of hospitals nationwide; however, many NCI designated cancer centers were represented in the study. The challenges noted are likely also occurring at community and rural health systems, which may face additional barriers to implementing pharmacogenomic programs. Other listservs may have more adequately captured this audience; however, we either did not have access to these listservs or they had strict limitations on the number of survey questions. Survey participants were likely to be interested and well versed in pharmacogenomics; however, we were able to temper this by utilizing objective questions about their institutional practice. Additionally, we did not inquire how often participants assess pharmacogenomics in their everyday practice, which may have influenced respondents’ comfortability with pharmacogenomics. Despite this, there was an overall high rate of comfortability assessing pharmacogenetic results, especially with pharmacogenomics that are commonly utilized in practice such as genetic-driven protein biomarkers. Another barrier of this survey is that only pharmacists were included. Physicians and advanced practice providers also routinely utilize pharmacogenomics, and their input along with senior leadership support is key to the implementation of a pharmacogenomic program.
Conclusions
Pharmacogenomics is a rapidly evolving field, and front-line pharmacists frequently encounter questions regarding the genetic result’s implications on potential treatment choices. Our survey revealed that pharmacists face many challenges implementing pharmacogenomics programs in hematology/oncology practice. Future efforts to assist in the appropriate utilization of pharmacogenomics should focus on increasing pharmacist involvement in local pharmacogenomics implementation (i.e. dedicated FTE, guideline authorship, MTB involvement, etc.), establishing and promoting more pharmacogenomic specialty training programs as well as incorporating pharmacogenomic goals and objectives into all pharmacy residencies, and encouraging pharmacy informatics leadership to support coordinated efforts between EMR vendors, health systems, and national guideline bodies to provide enhanced clinical decision support tools.
Key points
Pharmacogenomics is a rapidly evolving field that drives treatment decisions and substantial challenges exist when implementing a pharmacogenomic program. Generally, pharmacists were comfortable with assessing pharmacogenomic data; however, those who had more work experience or dedicated institutional resources reported more success in implementing pharmacogenomics programs. Future efforts to assist in developing pharmacogenomic efforts should focus on increasing pharmacist involvement, expanding education and training, and improving clinical decision support tools.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.