
Abstract
Background
To describe the prognostic value of neutrophil–lymphocyte ratio and its effect on survival in in patients with advanced renal cell carcinoma.
Methods
We retrospectively analyzed 331 patients. The cut-off value of neutrophil–lymphocyte ratio was specified as “3” which is mostly close—and also clinically easily applicable—to the median neutrophil–lymphocyte ratio level of our study group. High group is identified as neutrophil–lymphocyte ratio >3 (n = 160) and low group is identified as neutrophil–lymphocyte ratio ≤3 (n = 163).
Results
A total of 331 (with 211 male and 120 female) patients were enrolled to study. The median age of the patients was 58. The International Metastatic RCC Database Consortium risk score is calculated for the 72.8% (n = 241) of the study group and among these patients, favorable, intermediate, and poor risk rates were 22, 45.2, and 32.8%. The total usage of tyrosine kinase inhibitors reached 78% of the patients. The median overall survival was 32 months versus 11 months in the neutrophil–lymphocyte ratio low and high groups, respectively (HR: 0.49 (95% CI 0.37–0.65), p < 0.001).
Conclusion
In conclusion, the pre-treatment value of elevated neutrophil–lymphocyte ratio might be a predictor of poor overall survival in advanced renal cell carcinoma patients.
Introduction
Renal cell carcinoma (RCC) has an increasing prevalence, and according to the USA statistics, the disease accounts for 5% of all cancer cases in men, 3% in women with an estimated 73,820 new cases and 14,770 deaths in 2019. 1 RCC has three major histologic subtypes which are clear cell (75–80%), papillary (10–15%), and chromophobe (4–5%). 2
The five-year survival rate was <10% until the 2000s, but the expanding treatment options with tyrosine kinase inhibitors (TKIs) and checkpoint inhibitors dramatically changed the survival expectancy. In 2019, CheckMate 214 announced 60% of 30-month overall survival (OS) rate in intermediate and poor risk groups of advanced RCC patients with nivolumab plus ipilimumab combination, as well as KEYNOTE-426 reported 60% of objective response rate with pembrolizumab plus axitinib combination.3,4 These studies—likewise so many prospective, randomized, phase III trials—used the Memorial Sloan-Kettering Cancer Center (MSKCC) and/or International Metastatic RCC Database Consortium (IMDC) scoring systems to stratified RCC patients.
In this context, increasing survival rates with growing alternatives to effective treatment agents raise the importance of prognostic tools. Moreover, these prognostic factors began to play an active role in the selection of treatment modalities and sequences by defining different patient populations according to risk groups. As a validated prognostic score, IMDC is calculated by six parameters which are Karnofsky performance status, time from diagnosis to treatment of less than one year, hemoglobin, neutrophils, platelets, and corrected calcium levels. Especially the levels of neutrophils and platelets were an addition to MSKCC score. The estimated two-year survival rates are 75, 53, and 7% for favorable, intermediate, and poor risk groups, respectively. 5
Thanks to advances in genetics and immunology, new parameters that may affect prognosis in renal cell cancer are identified increasingly on the verge of “individualized treatment age,” but at the end of the day the features of a clinically useful marker remain the same. 6 It should be cost-effective with high accuracy, locally feasible, internationally standardizable, as well as inclusive for most of the patients as a part of routine clinical practice.
Biomarker studies such as C-reactive protein, albumin, fibrinogen, cytokines, or different ratios generated with hematologic indices of neutrophils, platelets, lymphocytes, monocytes that can predict treatment response or prognosis in cancer patients are still ongoing.7,8 Since the relationship between inflammation and cancer has long been known, the role of inflammatory markers as biomarkers is often explored. It is well known that systemic inflammation has a significant role in almost every step of carcinogenesis, malignant transformation and beyond that, on the process of invasion and metastasis. It also affects responses to different therapies and immune-escape mechanisms. 9
As an indicator of systemic inflammation, the neutrophil–lymphocyte ratio (NLR) is defined as neutrophil counts divided by lymphocyte counts. The prognostic value of this ratio is demonstrated by recent data in a wide range of different cancer types such as colorectal, ovarian, breast, lung, pancreas, and bladder cancer.10–15 There is also growing evidence of the prognostic value of NLR in RCC patients. Moreover, some studies suggest the use of this ratio as a parameter in IMDC score instead of neutrophil count alone.16,17 But, there is still no consensus on what should be the cut-off point of this ratio.
In this multicenter study, we aimed to demonstrate the prognostic value of NLR and its effect on survival in advanced RCC patients.
Materials and methods
We retrospectively analyzed 331 patients diagnosed with advanced RCC in 2007–2017. Demographic characteristics and clinical data about patients and their diseases were gathered from hospital records and patients’ files. Inclusion criteria for the study included: pathologically confirmed diagnosis of RCC, and advanced tumor stage (primary or relapse) according to radiological evaluation with CT and/or MRI and/or PET/CT scan. OS for metastatic RCC was defined as the period from the date of diagnosis of advanced disease to death or last follow-up.
The cut-off value of NLR was specified as “3” which is mostly close—and also clinically easily applicable—to the median NLR level of our study group. High group is identified as NLR >3 (n = 160) and low group is identified as NLR ≤3 (n = 163).
IBM SPSS 20 is used for statistical analysis. Survival curves were obtained by the Kaplan–Meier method, and the log-rank test was used to compare survival differences. Differences were considered as significant if the p-value was <0.05. The tendency of results was assessed if the p-value was ≤0.10. Local Clinical Research Ethics Committee’s approval was obtained.
Results
Study population
A total of 331 (with 211 male and 120 female) patients were enrolled to study. The median age of the patients was 58. Most of the patients (73.1%) had prior nephrectomy, and most of the cases (76.1%) were clear cell histology as expected. The ECOG performance status was 0 or 1 in 75.5% of the entire population. Only three patients (0.9%) did not have a detectable metastatic site, and 7.6% of the patients had CNS involvement. The patient characteristics are summarized in Table 1.
The clinical and demographic characteristics of the patients.
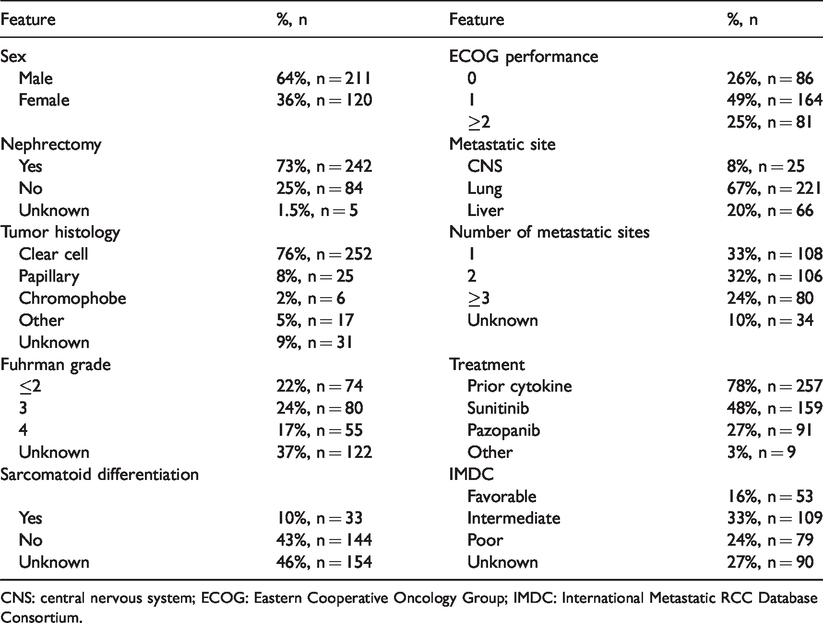
CNS: central nervous system; ECOG: Eastern Cooperative Oncology Group; IMDC: International Metastatic RCC Database Consortium.
The IMDC risk score was calculated for the 72.8% (n = 241) of the study group and among these patients, favorable, intermediate, and poor risk rates were 22, 45.2, and 32.8%, respectively.
The TKIs preferred for the 48% of the patients was sunitinib and for the 27% of the patients was pazopanib. The total usage of TKIs reached 78% of the patients.
Survival analysis according to NLR
There were 160 patients in the NLR high (>3) and 163 patients in the NLR low group. After median 27 months follow-up (defined as the time from diagnosis to death or the date of data cut-off for those who were alive), there were 93 events in the NLR low and 119 events in the NLR high group. The median OS was 32 months versus 11 months in the NLR low and high groups, respectively (HR: 0.49 (95% CI 0.37–0.65), p<0.001). (Figure 1)
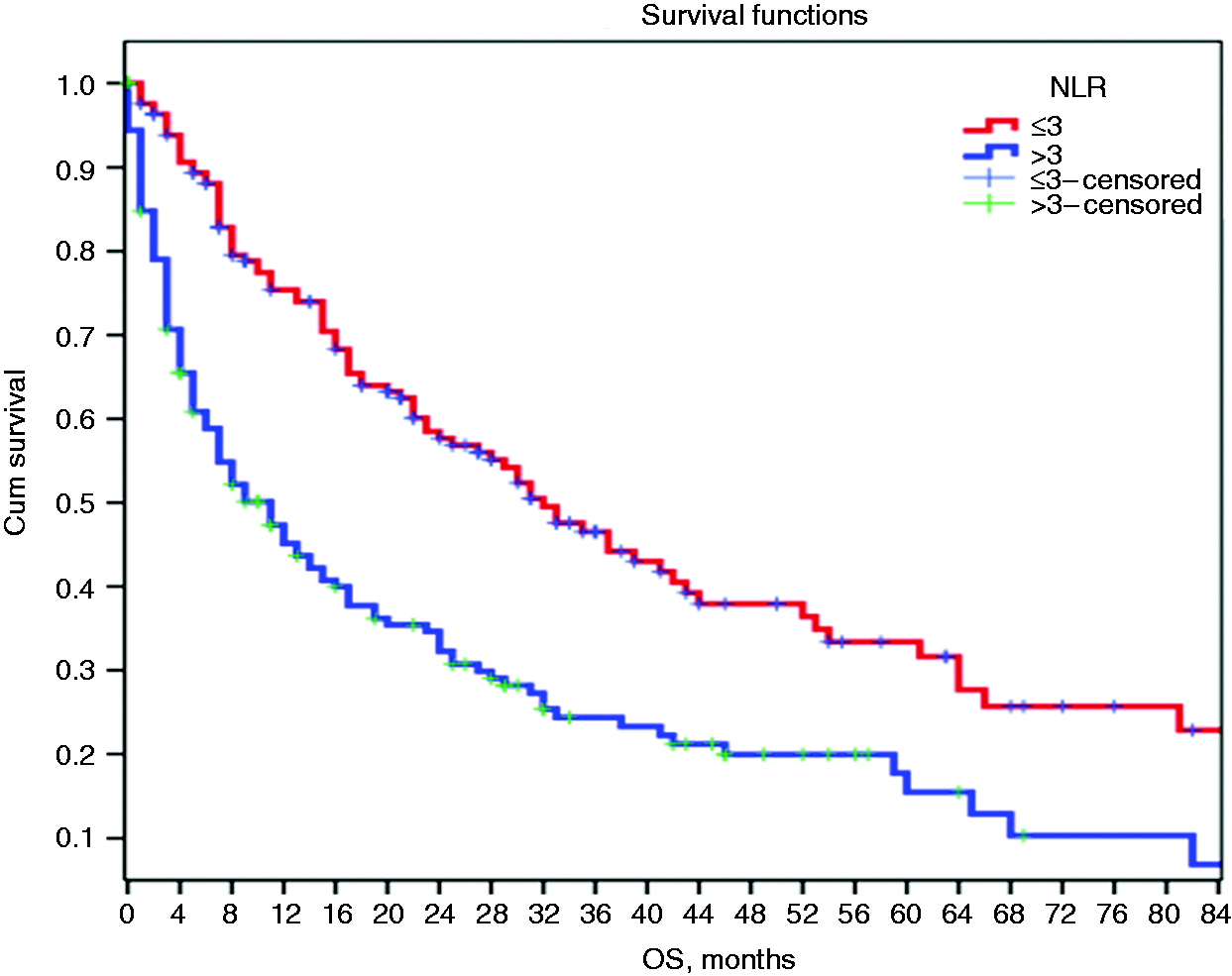
Survival analysis according to NLR.
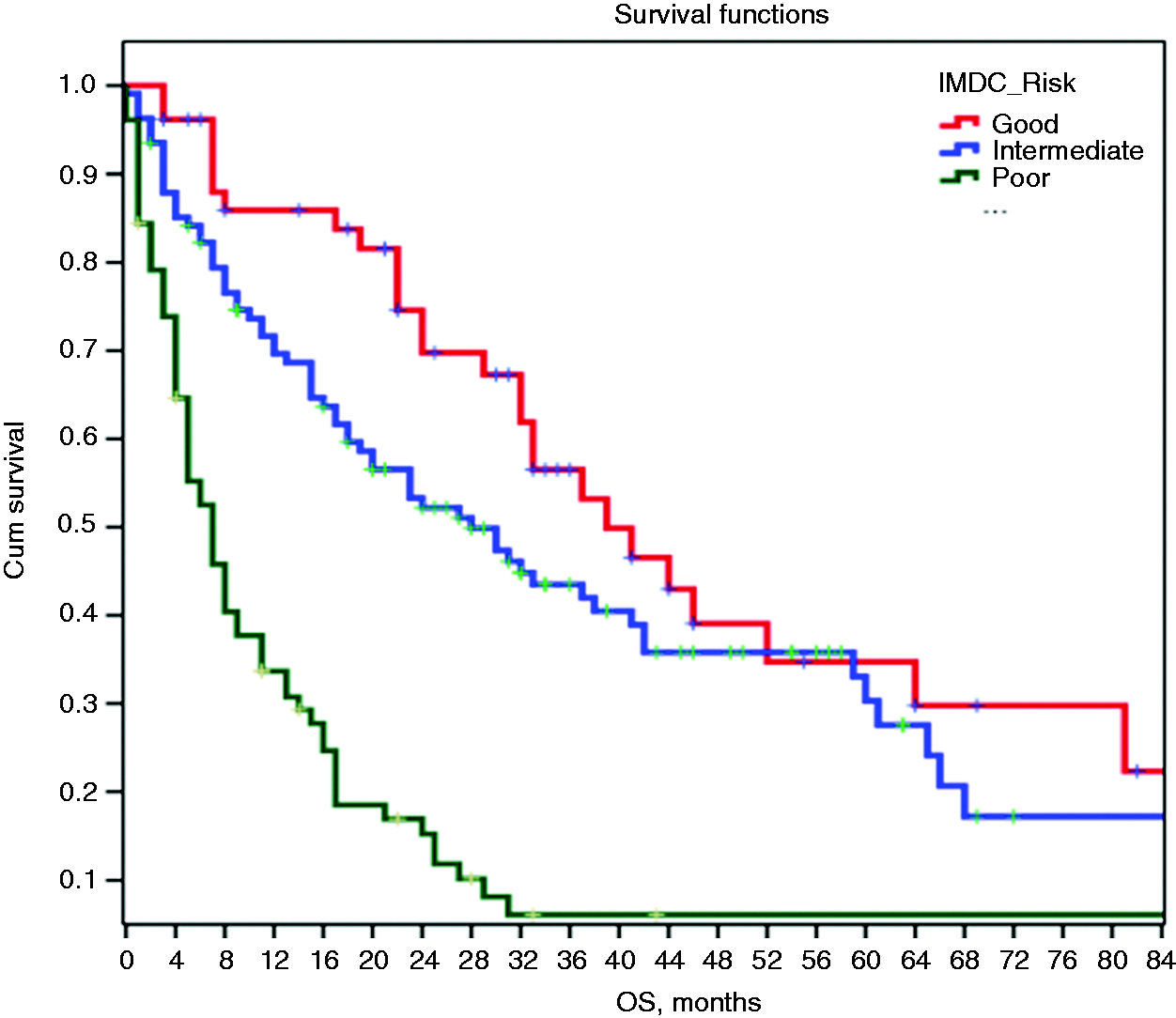
Survival analysis according to IMDC.
Survival analysis according to IMDC score
According to IMDC classification, there were 28 (n = 52), 68 (n = 108), and 67 (n = 77) events and the median OS was 39 versus 28 versus 7 months in the favorable, intermediate, and poor risk groups, respectively (p < 0.001) (See Figure 2).
Survival analysis of interferon population
Our data demonstrated that 78% of the patients (n = 257) received prior interferon-α treatment which is a very high rate compared with different regions of the world. But this situation is directly resulted by the local policy of health insurance coverage, and not related to the treatment choices of oncologists. As a natural consequence, only 86 patients received first-line IFN treatment for more than three months. There was no significant OS difference between NLR low (n = 60) and high (n = 26) groups of patients who received more than three months of IFN treatment (median OS 42 versus 32 months, p = 0.53).
Discussion
In the present multicenter study, as an easily applicable indicator in daily clinical practice, we investigated the prognostic effect of NLR in advanced RCC patients. The results showed that low (≤3) and high (>3) NLR levels had a statistically significant difference in terms of OS and this ratio might have prognostic significance in advanced RCC patients.
RCC has different disease characteristics with high somatic mutational burden. 18 These different genomic profiles are mostly responsible for the highly systemic inflammatory response of the host and present the disease as an “immunogenic tumor” with its well-known refractoriness to cytotoxic treatments. 19 The unique pathogenesis of the disease also represents an intersection for tumor immunology and cancer-inflammation relationship which are two growing fields of research. Especially for clear cell RCC, VHL-induced hypoxia, TNF-α, and STAT induce inflammatory signals which contribute to carcinogenesis and progression. Also, inflammatory cells (neutrophils, macrophages, lymphocytes) and cytokines (mainly TGF-β and IL-6) are well identified with their effects on transformation, proliferation, metastasis, and immune-escape mechanisms in RCC. 20 In this context, NLR may indicate prognosis in RCC patients, either increased inflammatory response or reduced immune response represented by elevated neutrophil count or decreased lymphocyte count, respectively.21,22
Our results are compatible with recent data. The study of Zhang et al. 22 also demonstrated a statistically significant OS difference between NLR high and low populations with median 28.8 versus 41 months. This study included 373 metastatic RCC patients who received targeted therapy similar to our study and pre-treatment NLR cut-off determined as 2.2, which was also numerically close to our study’s cut-off value. We clarify the wide range of the OS difference between our and Zhang’s research (median 11 and 28.8 months for high NLR, and median 32 versus 41 months for low NLR, respectively) with worse prognostic features of our study cohort. Compared with recent studies, the number of patients in the poor-risk group was higher in the present study.
Another retrospective study which collected the data of 141 metastatic RCC patients reported median OS 7.8 versus 36.1 months for high and low NLR groups which stratified according to 3.68 cut-off value. 8 Moreover, this study demonstrated that higher NLR was still an independent prognostic factor for shorter OS in multivariate analysis.
Although various studies which analyzed NLR in metastatic RCC included different cohorts with different demographic and prognostic features, the survival appears to be shorter at least quantitatively as the cut-off value for NLR increases.8,22 Nearly all studies used the NLR value between 2 and 4 and reached different results.
The effort to elucidate an acceptable, standard NLR value is still ongoing. In the meta-analysis conducted by Hu et al., 23 it has been shown that the predictive role is higher when NLR cutoff was ≤3. Another meta-analysis by Boissier et al. 24 reported that the prognostic value of NLR was stronger for advanced disease instead of localized RCC and a cut-off value of NLR = 3 predicted OS. There were also a few prospective trials in this area. One of them was a multicenter, randomized phase III trial which included 362 patients and again the threshold of 3 for pre-treatment NLR significantly (p = 0.008) predicted OS in advanced RCC patients. 25 Another prospective study assessed the NLR effect on survival and significant relationship achieved when the cut-off value was 4 instead of 3. 26 But this study did not include RCC patients. So, our results are consistent with recent data and support to use the cut-off value of 3 for NLR, in advanced RCC patients. But this result needs to consolidate with prospective trials.
Our study may have selection bias as a weakness like many other retrospective studies. But, the study cohort which tried to reflect real-life data with over 300 patients might overwhelm this difficulty. However, when we examine the survival of our cohort according to IMDC risk groups, the survival rates are very compatible with the published IMDC studies, which is one of the strengths of our study. The IMDC scoring system is universally accepted and used as a stratification factor in prospective phase III trials. It is also used to select treatment modalities. In a patient-based approach for daily clinical practice, its power to predict prognosis may not be as same as for every individual. There are wide ranges in terms of two-year OS between groups (75, 53, and 7%) according to IMDC. 5 The literature already has a trial that “proposed” to revise IMDC with NLR instead of neutrophil count. 16 Our study did not aim a modification like that; however, the threshold value of 3 was also virtually represented as a median NLR level of our cohort. This fact naturally resulted in two new survival plots between IMDC groups. In a manner of “subgroups,” NLR may have potential as an “additional tool” with IMDC to predict prognosis and better patient-selection. But this is just a future perspective which needs to be analyzed with further studies.
Most of our patients (78%) were treated with anti-VEGF targeted therapy. The percentage of patients who received sunitinib or pazopanib (which had shown non-inferiority to sunitinib with COMPARZ trial) was 75%. In another study which included 133 metastatic RCC patients who were treated with sunitinib reported that low NLR was associated with OS. 27 Similarly, the cut-off NLR value was 3 in this study, and the median OS was 29 versus 14 months (HR = 0.3, p = 0.043). The rationale mostly depended on the inflammatory effect of large amount of cytokines (mainly IL-1 and IL-6) produced by neutrophils and reduced immune response as a result of low CD4+ T lymphocyte counts. 28 However in cancer patients, granulocytes (mainly neutrophils) also secrete most of the VEGF (69% of the total circulating amount) which is essential for both RCC pathogenesis and targeted treatment strategies. 29
Interferon therapy for renal cell cancer has been mostly abandoned and is not recommended by the guidelines. Unfortunately, local health insurance policy still allows reimbursement of TKIs only after IFN treatment. The high rates of IFN usage in our study did not correlate with total IFN exposure because oncologists have strong tendency to discontinue this treatment in any grade of toxicity and/or clinical suspicion of disease progression, mostly in weeks and without radiological response assessment. Only 86 patients received IFN treatment for more than three months and there was no OS difference according to NLR in this subgroup. Our study may be the first in literature to assess NLR in RCC patients who received IFN treatment. However, the total effect of IFN exposure on to our results may be negligible.
Another point to consider are potential comorbidities that might have an impact on OS results because NLR might have been associated with a wide range of disease spectrum such as cardiovascular diseases, hypertension, diabetes, chronic kidney disease, and some gastrointestinal conditions which any of them easily “shorten” survival. 30 On the other hand, a Korean study clarified this situation with demonstration of NLR as an independent prognostic factor on cancer-specific survival in metastatic RCC patients. 31
In the last decade, new treatment strategies developed with checkpoint inhibitors and treatment algorithms have changed for advanced RCC patients. A study reported the prognostic value of NLR in patients treated with checkpoint inhibitors, but this trial included mainly melanoma and non-small cell lung cancer as well as 38 metastatic RCC patients. 32 As a future perspective, NLR will be a potential prognostic candidate also for RCC patients who will be treated with immunotherapy.
To the best of our knowledge, with 331 advanced RCC patients, our study has one of the largest cohorts between similar trials evaluated for the prognostic effect of NLR. In conclusion, pre-treatment value of elevated NLR (>3) might be a predictor of poor OS in advanced RCC patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.