
Abstract
Introduction
Hepatoid adenocarcinoma of the lung is an extremely rare type of the non-small cell lung cancer. Treatment principles and prognosis are similar to that of lung adenocarcinoma.
Case report
A 62-year-old female smoker presented with a huge mass in the left upper lobe. After diagnostic biopsy, she underwent left pneumonectomy and mediastinal lymph node dissection. A diagnosis of stage T4N1M0 hepatoid adenocarcinoma of the lung with positive surgical margins was made.
Management and outcome
After the operation, the level of serum alpha fetoprotein was 9010 ng/ml (N: <10). The level of serum alpha fetoprotein was decreased with concurrent chemoradiotherapy and chemotherapy. Disease progression was detected at 11 months after diagnosis. No response was obtained to other therapies. The patient died at 14 months from the time of diagnosis.
Discussion
Usually, patients with hepatoid adenocarcinoma of the lung are male smokers. Hepatoid adenocarcinoma tends to settle in the upper lobes of the lung. The most important prognostic factor of the hepatoid adenocarcinoma of the lung is the disease stage at the diagnosis and patients with metastatic disease have poor survival.
Introduction
Hepatoid adenocarcinomas (HACs) are prognostically poor extra hepatic tumors resembling the morphology of hepatocellular carcinoma (HCC). It was first described in stomach by Ishikura et al. 1 HAC of the lung is a rare entity. The most frequent locations for extra hepatic HACs are stomach (63%), ovaries (10%), lung (5%), gallbladder (4%), pancreas (4%) and uterus (4%). 2 There is no specific immunohistochemical markers to differentiate HAC from hepatocellular carcinoma. 3 Ishikura et al. reported the very first HAC case originated from lung in 1990. 4 After this report, there have been less than 30 cases reported in medical literature, in English language. In this paper, we present a female patient with HAC of the lung and provide a brief overview of the previously reported cases.
Case report
A 62-year-old female presented with back pain lasting for two months. Computed tomography (CT) scan showed a 6-cm mass lesion in the left upper lobe of the lung. A fluorodeoxyglucose positron emission tomography (FDG-PET) scan showed a hypermetabolic left hilar mass lesion with a standard uptake value (SUV) maximum of 12.27 and hypermetabolic left pleural effusion (Figure 1). The mass obliterated the left lower lobe bronchi and settled between the arcus aorta, pulmonary artery and brachiocephalic vein. Non-small cell lung cancer (NSCLC) was diagnosed via broncoscopic biopsy. There were no metastases on magnetic resonance imaging (MRI) of the brain. Mediastinal lymph node dissection and left pneumonectomy were performed on 10 May 2018. On gross examination, two masses measuring 8 × 7×7 cm and 3 × 2.5 × 2 cm were detected in the left upper lobe. Light microscopy examination revealed a tumor with trabeculated sinusoidal pattern similar to those seen in HCC of the liver and neoplastic cells with granular, eosinophilic cytoplasm, distinct cell boarders and prominent central nucleoli (Figure 2(a) and (b)). Mediastinal lymph nodes were free of metastasis; one hilar lymph node was positive. Surgical margin was positive on the parietal pleura. Immunohistochemistry stains were positive for pancytokeratine, arginase, alpha fetoprotein (AFP) and HepPar, but negative for cytokeratin 5/6, 7 and 20, thyroid transcription factor 1 (TTF 1, nuclear) and napsin (Figure 2(c) to (e)). The diagnosis of stage T4N1M0 HAC of the lung was made. Tumor was negative for EGFR and BRAF 600E mutation, anaplastic lymphoma kinase (ALK) gene rearrangement and ROS 1 fusion. After the operation, the level of serum AFP was 9010 ng/ml (N: <10). Other routine biochemical tests and complete blood count were unremarkable. She had a history of smoking 1 pack of cigarette daily for 45 years and gave up smoking 5 years ago. She had not used alcohol. She was on antihypertensives, anxiolytics and antidepressants (metoprolol, valsartan/hydrochlorothiazide, mirtazapine, clonazepam, escitalopram, pantoprazole) for years. Her performance score was 1. She received adjuvant chemoradiotherapy (CRT) (carboplatin 2 AUC plus paclitaxel 50 mg/m2 weekly with concurrent radiotherapy to tumor bed (50 Gy of intensity-modulated radiotherapy (IMRT) in 25 fractions)) and chemotherapy after CRT (two cycles of carboplatin 5AUC plus paclitaxel 175 mg/m2, every three weeks). After the treatment, serum AFP decreased to 99 ng/ml, and there was no detectable tumor on post-therapy PET CT imaging on October 2018, and the patient was scheduled for clinical and radiological follow-up every three months. Three months later, serum AFP increased to 640 ng/ml, but the patient was asymptomatic, and there was no clinical evidence of a relapse. A follow-up PET CT was done, which did not show an evidence of a recurrence or metastasis. On April 2019, progression of disease was observed and nivolumab (3 mg/kg, every two weeks) was started. After five cycles of nivolumab, disease progression occurred. Her performance status quickly deteriorated, weekly carboplatin plus paclitaxel was given again. Unfortunately, she died on 17 July 2019 due to disease progression.
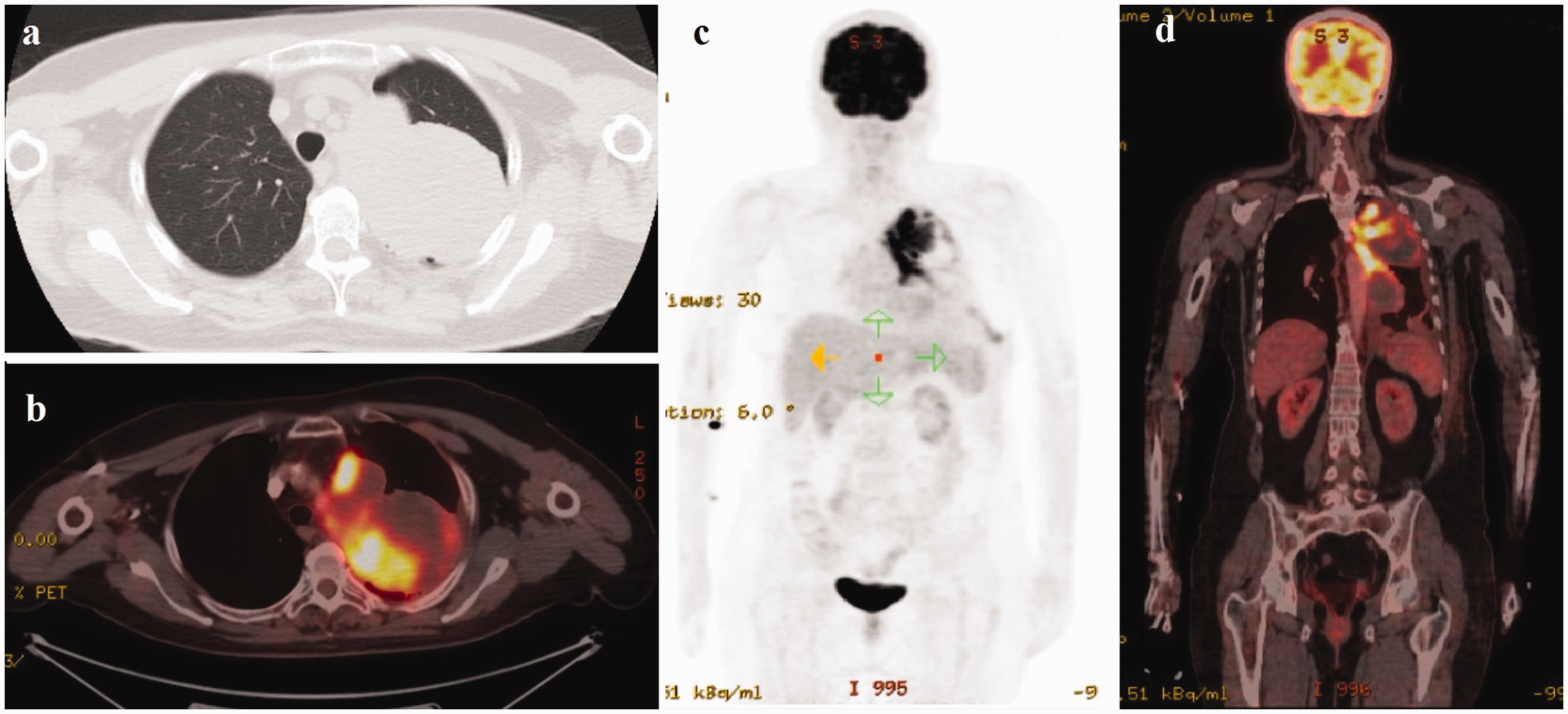
Fluorodeoxyglucose-positron emission tomography/computed tomography (FDG-PET/CT) scanning. (a) CT imaging of the chest showing a 7.7 × 9.4 cm mass adjacent the mediastinal pleura in the left upper lung. (b and d) Fused imaging revealing FDG uptake by the left upper lung lobe mass with hypodense and non-metabolic areas and left hypermetabolic pleural effusion. (c) FDG uptake by the left lung upper lobe mass and left pleural effusion.

(a) The tumor composed of solid sheets displaying trabeculated sinusoidal pattern similar to those seen in hepatocellular carcinoma of the liver (H&E, ×200), (b) the tumor cells have granular, eosinophilic cytoplasm, distinct cell boarders and prominent central nucleoli (H&E, ×400), (c) the tumor cells showing diffuse alpha-fetoprotein positivity (AFP immunostaining, ×400), (d) the tumor cells showing focal and weak positivity with arginase (arginase immunostaining, ×400), (e) the tumor cells showing focal and weak positivity with HepPar (HepPar immunostaining, ×400).
Discussion
Clinically, HAC of the lung has similar properties to that of pulmonary adenocarcinoma. Previously reported cases are summarized in Table 1. Median age at presentation was 56 years (36–82). Most of the patients were smokers and male. Our case is the third female patient reported in the literature. HAC of the lung usually involves upper lobes of lungs and presents as large masses. Only one patient with lower lobe involvement has been reported before. 5
Clinocopathological characteristics of patients with hepatoid adenocarcinoma of the lung.
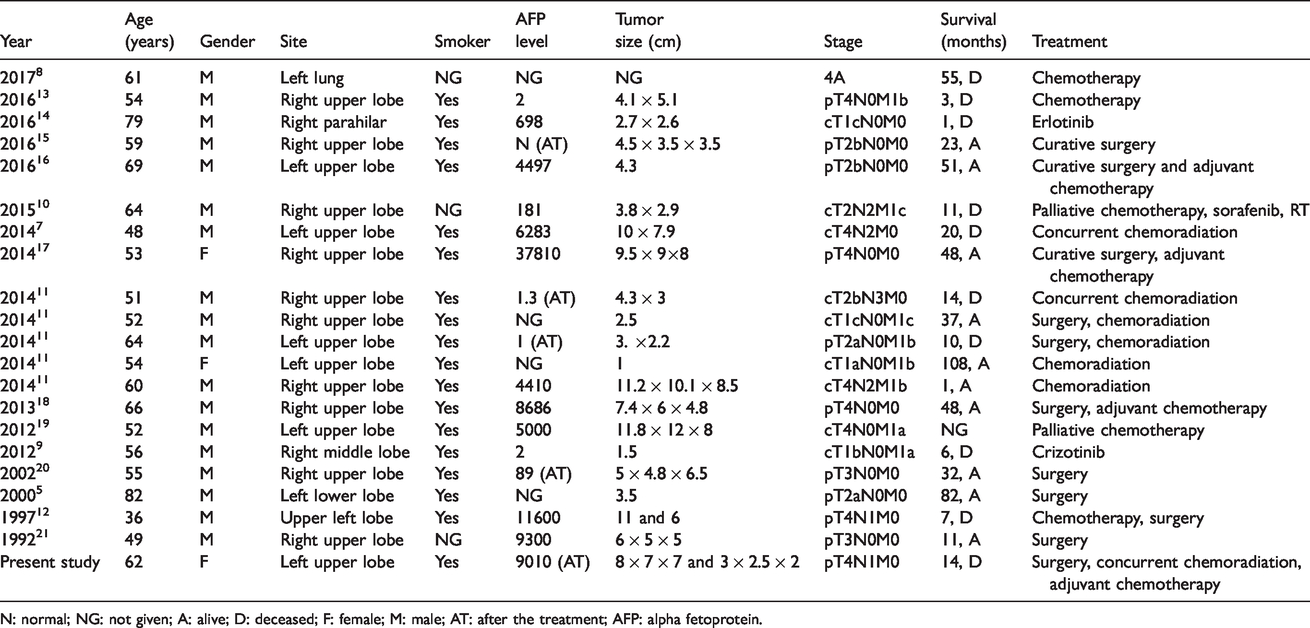
N: normal; NG: not given; A: alive; D: deceased; F: female; M: male; AT: after the treatment; AFP: alpha fetoprotein.
The most important prognostic factor is the disease stage at the diagnosis. 6 The range of the survival was between 1 and 108 months. Surgery is the only curative treatment option for early stage disease. Chemoradiation and chemotherapy can be used in later stages. In one case, paclitaxel and cisplatin were used as radiosensitizers in concurrent chemoradiation and partial response was obtained. 7 In a patient with stage 4 disease, front-line therapy with cisplatin and pemetrexed provided 55 months of survival. 8 Tyrosine kinase inhibitors can also be used in HAC of lung. In a patient with ALK-positive disease, crizotinib produced a partial response and seven months of survival. 9 In another case, a partial response was achieved with sorafenib addition to carboplatin and paclitaxel. 10 But it is not clear whether the benefit achieved is related with sorafenib or chemotherapy. In our patient, we gave adjuvant treatment with CRT followed by chemotherapy. After the therapy, an apparent decrease in AFP was detected.
According to Ishikura et al., 4 histologic findings of HAC of the lung are hepatoid cells with abundant, eosinophilic cytoplasm and centrally located nuclei that are usually round, but occasionally elongated. In cytoplasm, spicular bodies and PAS-positive, diastase-resistant hyaline globules can be seen. Immunohistochemical findings are variable in HAC of the lung. In a study with five cases, tumors expressed CK5/6 (1/5), CK7 (3/5), CK 19 (4/5), CK 20 (1/5), AFP (3/5), CEA (3/5), napsin A (1/5) with varying frequencies. HAC of the lung stains similar to HCC, HepPar (5/5), TTF 1 (cytoplasmic) (5/5), CK8 (5/5) and CK18 (5/5) and does not stain for CK14 (0/5). Unlike HCC, it expresses MOC31 (5/5) and HEA 125 (5/5). 11 Another study showed that in eight patients with hepatoid carcinoma, arginase 1 was positive in five. 3 Elevated serum AFP level does not necessarily indicate the diagnosis of HAC (Table 1). In our patient, elevated serum AFP level was detected after curative surgery, and immunostains of the tumor such as HepPar 1, arginase and AFP were positive (Figure 2(c) to (e)).
Differential diagnosis of HAC of the lung is similar to metastases of HCC, pulmonary large cell carcinoma and germ cell tumors. Imaging studies can exclude metastasis from HCC. Pulmonary large cell carcinoma does not usually secrete AFP. When an eosinophilic large cell tumor-secreting AFP is encountered, HAC should be considered, regardless of mucin secretion. If an AFP-secreting tumor was detected in the lung, a sheet-like growth of neoplastic cell with eosinophilic cytoplasm, specular bodies, tubular and papillary structure should be investigated. 4
In some cases, when an AFP-secreting thoracic mass is detected, germ-cell tumors first come to mind and treatment can be given without a biopsy. Arnould et al. reported a patient with AFP-secreting left upper lung mass mimicking germ cell tumor clinically. The patient was treated with three cycles of BEP chemotherapy (bleomycin, etoposide and cisplatin) and no response was seen. After the biopsy, the diagnosis of HAC of the lung was made. 12 Hence, in case of AFP-secreting thoracic masses, biopsy is mandatory before starting the treatment.
In conclusion, HAC of the lung should be considered in a smoker patient with AFP-secreting upper lung mass. Biopsy is necessary for definitive diagnosis. Disease stage at presentation is the most important prognostic factor. Approach and principles of treatment of HAC of lung are similar to that of lung adenocarcinoma, unless otherwise specified.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.