
Abstract
Purpose
Soft tissue sarcomas are associated with a poor prognosis and low chemotherapeutic efficiency. Pazopanib is an orally available multi-tyrosine kinase inhibitor that was explored in patients with non-adipocytic advanced soft tissue sarcomas. The aim of this retrospective study was to evaluate the real life data of single-agent pazopanib efficacy and safety for soft tissue sarcomas in the Turkish population.
Materials and methods
We evaluated a total of 103 patients (41 males, 62 females) who received pazopanib for advanced non-adipocytic soft tissue sarcomas diagnosis in eight centers of Turkey, retrospectively. The pazopanib dose was 800 mg once daily. Progression-free survival, overall survival, and adverse events were analyzed.
Results
The median age was 50 years (range, 38–58). Majority of the patients had leimyosarcoma (41%). Median progression-free survival was 4.3 months, and the median overall survival was 10.1 months. The main common toxicities were fatigue, anorexia, weight loss, nausea, hypertension, and grade ≥3 toxicities were fatigue, anorexia, weight loss, and liver disorder.
Conclusion
Pazopanib is an efficient and tolerable agent and is well tolerated in good performance status patients with relapsed, advanced non-adipocytic soft tissue sarcomas.
Introduction
Soft tissue sarcomas (STS) are a group of rare mesenchymal cancers and account for 1% of all adult malignancies. STS are a heterogeneous group of tumors that include about 50 histological subtypes that exhibit great differences in terms of clinical behavior, pathogenesis, treatment response, and prognosis.1,2 They can arise almost anywhere in the body, about 43% occurs in the extremities; 34% occurs in and around the internal organs; 10% occurs in the trunk; and 13% occurs in other locations. 3 The primary treatments of STS are surgery and radiotherapy. However, in approximately 40% of patients, tumor recurrence is seen and survival rate is poor, with a median overall survival (OS) of less than 12 months. Risk factors for recurrent disease are described as incomplete resection, high-grade, aggressive histology, larger than 5 cm of tumor size and deep location. 4
First-line treatment for advanced STS other than gastrointestinal stromal tumors is an anthracycline (usually doxorubicin), either as monotherapy or in combination with ifosfamide. The development of new systemic treatments for patients with STS has been limited in the last decade, with the exception of treatments for gastrointestinal stromal tumors. Paclitaxel has shown efficacy and good tolerability in angiosarcoma. 5 Gemcitabine with dacarbazine or docetaxel has demonstrated activity in uterine leiomyosarcoma (LMS).6,7 Trabectedin was approved in Europe in 2007 for patients with STS as second- or third-line chemotherapy; 8 however, trabectedin plus doxorubicin did not show superiority over doxorubicin alone as first-line treatment of advanced STS. 9
Focusing on targeted therapies for STS subtypes has been started as a result of imatinib success of producing a dramatic improvement in disease control by targeting KIT and platelet-derived growth factor (PDGF) in gastrointestinal stromal tumors. 10 Pazopanib is an orally available, multitarget tyrosine kinase inhibitor with activity against vascular endothelial growth factor receptor 1 (VEGFR-1), VEGFR-2, VEGFR-3, and PDGF receptor a (PDGFR-a), PDGFR-a, and c-kit. 11 Several studies have demonstrated that high levels of vascular endothelial growth factor (VEGF) and PDGF receptor signaling are also involved in tumor angiogenesis.12,13 Pazopanib was tested for its efficacy in a phase II study and, subsequently, was approved in a placebo-controlled phase III study (PALETTE) in patients with pretreated, advanced, non-adipocytic STS. PALETTE trial has shown that pazopanib significantly increases progression-free survival (PFS) by a median of three months compared with placebo, showing the activity of pazopanib after second-line treatment. 14
The aim of this multicenter retrospective study was to evaluate the efficacy and tolerability of pazopanib in patients with advanced STS.
Materials and methods
Patients
Data were evaluated for 103 patients with advanced STS who were given pazopanib retrospectively in a total of eight centers in Turkey. Patients’ data were obtained from clinical and histopathological diagnostic records. All of the patients had STS diagnosis histopathologically. Clinicopathological characteristics such as age, sex, STS histological subtype, stage, Eastern Cooperative Oncology Group performance status (ECOG PS), prior treatments, metastatic sites, treatment side effects, and patient survival were recorded. Majority of patients had ECOG performance score of 0–2 (only three patients with ECOG 3).
Treatment and follow-up
Pazopanib was administered at a dose of 800 mg/day orally. According to the type and severity of the observed adverse events, pazopanib was reduced to 600 or 400 mg. Treatment was discontinued in patients with disease progression and in those experiencing severe toxicity even after sufficient dose modification. Adverse events were graded according to the Common Terminology Criteria for Adverse Events version 3.0.
A computed tomography (CT), magnetic resonance imaging, or positron emission tomography CT was performed at baseline and after the institution of treatment periodically to assess the response according to the response evaluation criteria in solid tumors version 1.0.
Statistical analyses
PFS was calculated as the time from initiation of pazopanib therapy to disease progression demonstrated with an imaging method or to death from any cause. OS was calculated as the time from initiation of pazopanib therapy to the date of last follow-up or to death from any cause. PFS and OS estimates were analyzed using Kaplan–Meier plots, factors related with PFS and OS were compared with the log-rank test, and related 95% confidence intervals (CIs) were also calculated. All statistical analyses were completed using the SPSS 24.0 software (SPSS Inc., Chicago, IL). The safety analyses were performed by descriptive statistics. A p value of <0.05 was considered statistically significant.
Results
Patient characteristics
We analyzed 103 patients (42 males, 61 females) and the median age was 50 years (range, 38–58), Table 1 shows the demographics and patients’ baseline characteristics. Seventy-two out of 103 patients (70%) had a good performance status (ECOG: 0 or 1). Previous adjuvant or neoadjuvant anthracycline-based therapy was present in medical history of 42 (41%) patients. Thirty-two (31%) patients were metastatic at the time of diagnosis. Among these, 65 patients (63.1%) had received anthracycline-based treatment, 31 (30%) gemcitabine + docetaxel combination, and 7 patients (8.9%) were utilized other types of treatment as the metastatic first line therapy. Pazopanib was the second-line treatment for 53 patients (51%), third line of treatment in 40 patients (39%), and fourth or later line for 10 patients (9%).
Patients’ characteristics.
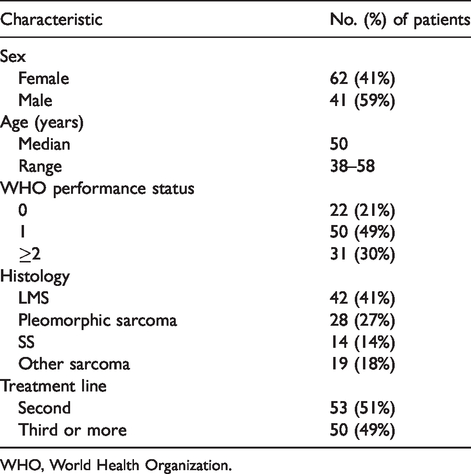
WHO, World Health Organization.
The histologic subtype was as follows: LMS (n:42), undifferentiated pleomorphic sarcoma (UPS) (n:28), synovial sarcoma (SS) (n:14), and others (n:19) (myxofibrosarcoma) (n:6), malignant peripheral nerve sheath tumor (n:5), epithelioid sarcoma (n:2), solitary fibrous tumor (n:2), rhabdomyosarcoma (n:2), angiosarcoma (n:1), and alveolar soft-part sarcoma (n:1)).
The primary tumor locations in decreasing frequency were the extremities (n:38), uterus (n:26), intra-abdominal (n:25), trunk (n:7), head and neck (n:6), and lung (n:1). The distribution according to metastasis sites was as follows: lung (n:73), lymph node (n:38), liver (n:24), bone (n:18), and local recurrence (n:32).
Adverse events
Pazopanib initially was administered orally once daily at a dose of 800 mg in 103 patients. The median treatment duration was 3.8 months (0.6–29.4). Grade ≥1 adverse events occurred in 99 patients (96.1%), whereas Grade ≥ 3 adverse events were reported in 30 (29%) patients. Dose reduction was done in 32% of patients. The treatment was interrupted in 18.4% of patients.
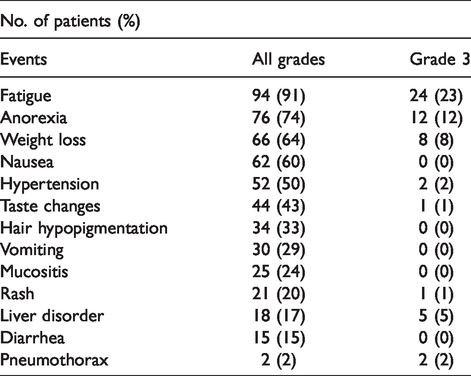
The main common toxicities were fatigue (n:94), anorexia (n:76), weight loss (n:66), nausea (n:62), hypertension (n:52), taste changes (n:44), hair hypopigmentation (n:34), vomiting (n:30), mucositis (n:25), rash (n:21), liver disorder (n:18), diarrhea (n:15), and pneumothorax (n:2). The main common grade ≥3 toxicities were fatigue (n:24), anorexia (n:12), weight loss (n:8), liver disorder (n:5), hypertension (n:2), and pneumothorax (n:2). Table 2 represents the common adverse events.
Common adverse events.
Common Grade 3–4 adverse events observed in patients of ECOG PS 0-1 versus ≥2 were 18.1% (n:13/72) and 54.8% (n:17/31), respectively (p < 0.0001). Dose reductions and/or treatment interruptions because of the occurrence of an adverse event were required in 40 patients (39%).
Treatment was interrupted in 19 patients (18.4%) receiving pazopanib while dose reductions occurred in 33 (32%). The main reasons for an interruption or reduction in dosage of pazopanib treatent were fatigue (n:29), liver disorder (n:6), and hypertension (n:5). The frequency of dose modifications, either interruption or reduction, was 30.5 and 58% in ECOG 0-1 and ECOG ≥2, respectively (p:0.015).
Outcome
Median follow-up time was 36 months (2–169). At the data cutoff date of 5 May 2017, seven patients were still on pazopanib treatment and 81 (79%) patients had died. Two (2%) patients achieved complete response (CR), 19 (18%) patients had partial response (PR), 22 (22%) patients had stable disease (SD), and 60 (58%) patients had progressive disease (PD) (Table 3).
Best overall response for pazopanib treatment.
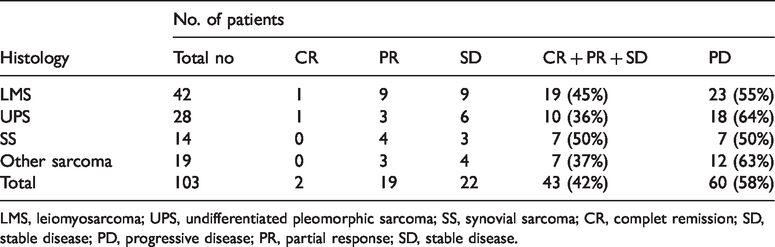
LMS, leiomyosarcoma; UPS, undifferentiated pleomorphic sarcoma; SS, synovial sarcoma; CR, complet remission; SD, stable disease; PD, progressive disease; PR, partial response; SD, stable disease.
Median PFS was 4.3 months (95% CI, 0.6–29.4 months). The median PFS in patients who had LMS, UPS, SS, and others was 5.3, 3.1, 3.8, and 3.6 months, respectively (p:0.59). The median PFS of patients with ECOG: 0–1 was 7.2 months (1–29.4) whereas it was 2.3 months (0.6–6.6) in those with ECOG ≥ 2 (p < 0.0001) (Figure 1).
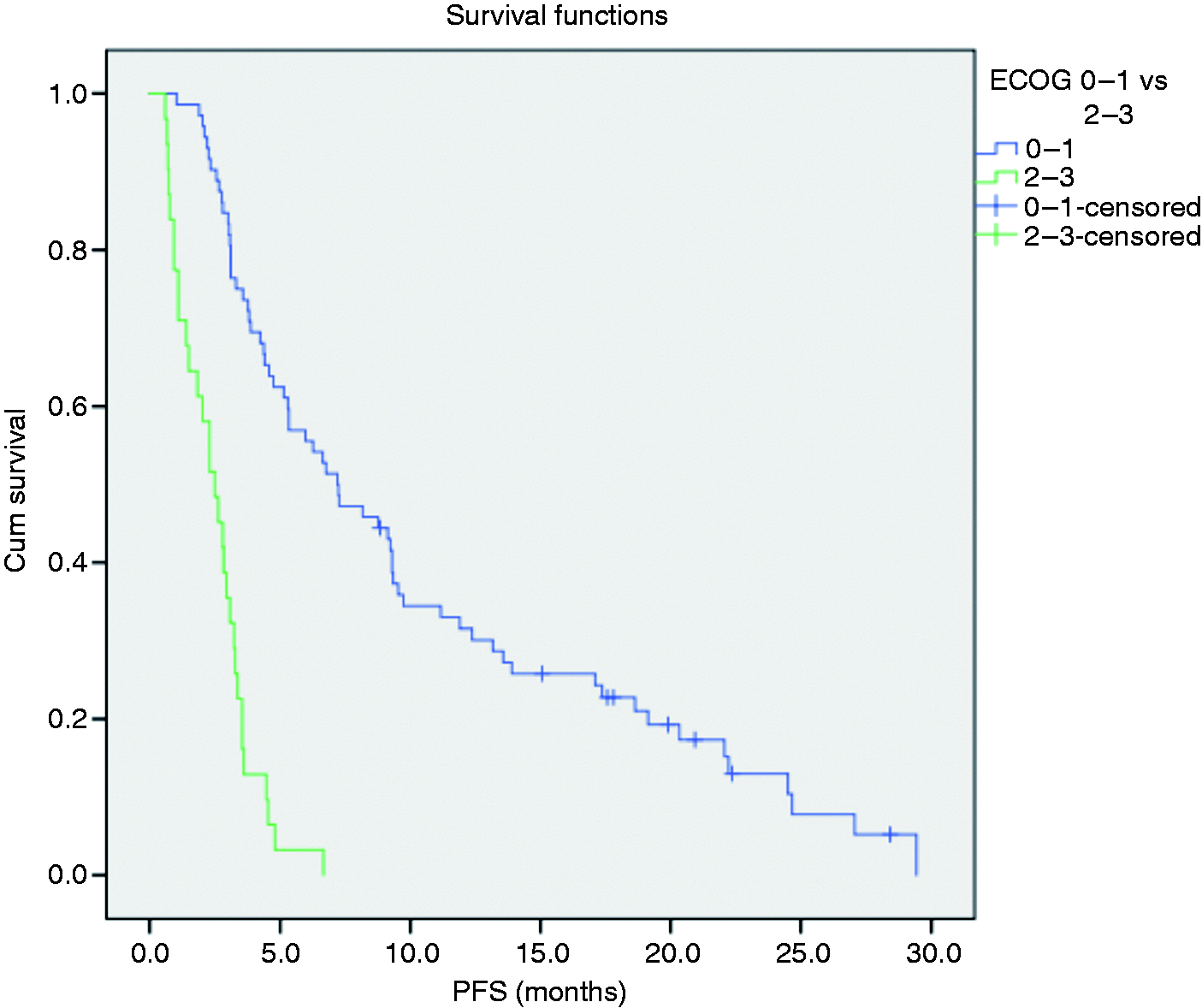
Progression-free survival according to ECOG performance status.
The median OS was 10.1 months (95% CI, 0.7–50.8 months). We also analyzed the OS of patients based on their histologic subtypes. The median survival for patients with LMS, UPS, SS, and others was 11.9, 6.7, 4.5, and 12.5 months, respectively (p: 0.24). The median OS of patients with ECOG: 0–1 was 14 months (2.4–50.8), whereas it was 3.4 months (0.7–26.7) in those with ECOG ≥ 2 (p < 0.0001).
Univariate analysis revealed that presence of necrosis, histological grade 3, ECOG PS ≥ 2, Ki 67 > 20% were all poor prognostic features for OS. In the multivariate analysis, while necrosis (p = 0.785), ki67 ≥ %20 (p = 0.054), histological grade 2 (p = 0.409), and histological grade 3 (p = 0.760) did not found to be associated with poor OS, ECOG PS ≥ 2 (p < 0.001), was the only variable significantly related to a decreased survival.
Discussion
Pazopanib, an oral multikinase inhibitör, is a new treatment option for patients with relapsed or metastatic non-adipocytic STS after chemotherapy, that has been approved based on the randomised, placebo-controlled phase 3 PALETTE study results. 14 In this multicenter retrospective study, pazopanib was revealed to be a promising therapy with regard to efficacy and tolerability in a daily practice population of STS.
The median PFS in all patients was 4.3 months which is similar to that in PALETTE study (4.6 months for pazopanib group). But when divided into two groups according to ECOG performance status (PS) as PS 0-1 and ≥2, PS 0-1 group did better than those in PALETTE study (7.2 vs. 4.6 months) which did not include patients with poor performance status. The median OS of all patients was 10.1 months, which is slightly below the estimated 12.5 months in PALETTE study whereas the OS in the PS 0–1 subgroup was 14 months which is better than that of PALETTE study. We excluded lipogenic sarcomas so did PALETTE study, even so, the mild superiority of our outcome data might be attributed to the different contribution of other histological subtypes with different inherent biological aggressiveness as measured by grade.
Nakamura et al., 15 in their retrospective analysis involving 156 patients, found a median PFS of 15.4 weeks and OS of 11.2 months which closely resembled our own findings. The study, contrary to our patient population, involved a considerable proportion of liposarcoma patients, and as expected, the tumor responses and corresponding survival outcome for those patients were found to be low. However, more patients (84.6%) compared to those in our study (70%) were of ECOG PS 0-1. This might neutralize the negative effect of the lipogenic-type sarcoma on survival and be the reason of two studies to point toward similar survival rates. In multivariate analysis, they reported that good ECOG performance status, female sex, none, or one previous chemotherapy line and a longer duration of pazopanib treatment as to be favorable prognostic markers. Among these, our study confirmed only an OS advantage for ECOG PS ≥ 2. They involved upfront pazopanib treatment for some patients who were appreciated as ineligible for chemotherapy. However, in the present study, pazopanib was offered at second or later lines of therapy which may be responsible for the statistically insignificance of the previous treatment line-effect, on survival. In a recent study, SPIRE, pazopanib was commenced to the heavily pretreated STS patients. 16 The authors, similar to our study, did not include patients using pazopanib at first line and found a similar median OS with no additional safety concerns noted.
Regarding adverse events, in the current study, the most frequent adverse events were fatigue, anorexia, weight loss, nausea and hypertension, and the most common grade ≥3 toxicities were fatigue, anorexia, weight loss and liver disorder. No toxic deaths occurred but adverse events reaching grade ≥3 were reported in 29% of patients which were similar that of the analysis carried out by Nakamura et al. 15 although the proportion of toxicities differed. In their study, hypertension was the main toxicity followed by liver disorder and pneumothorax. Due probably to this difference, the rate of treatment discontinuation was lower in the current study, as the toxicities like fatigue and anorexia were more likely for physicians to afford rechallenge of the treatment. The high incidence of pneumothorax, in some studies, was suggested to be related to marked amount of lung metastases.17,18 In contrast with this data, despite the high number of lung metastasis (approximately 70%), in the present study, the pneumothorax rate was relatively low (2%). Likewise, pneumothorax (3%) was remarkably low in PALETTE study. In general, ECOG PS 0-1 subgroup similar to that in PALETTE study, compared with PS 2 did better in all grades of adverse events, generating the data that pazopanib, was well tolerated in this patient population.
Due to the rarity of STS relative to other common malignancies, prospective trials are limited. In this setting, retrospective well-performed data can yield very useful information on clinical decision making in daily practice. In a more recent study by Seto et al., 19 investigating the real-world experiences on pazopanib, patients with adipocytic tumors and bone sarcoma were not excluded, not unexpectedly, median PFS was found to be relatively low. It is noteworthy that our study is comprised of a homogeneous population in terms of involving only non-adipocytic STS and represents a real-world data by means of not excluding patients with poor performance status.
Selection bias might be a limitation of the study given the retrospective nature. In addition, our population is relatively small not allowing the comparison between histological sarcoma subgroups and other potential prognostic characteristics. Another limitation is the potential subjectivity among institutions in the response assessment and follow-up that can lead to artifacts.
In conclusion, this multi-center study investigating pazopanib for non-adipocytic STS patients revealed that the treatment is efficacious and tolerable. We hope that future trials will contribute to the challenges about heterogeneity and molecular complexity of STS to identify distinct subgroups that will benefit more from the treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.