
Abstract
Purpose
In order to detect cancer therapeutics-related cardiac dysfunction (CTRCD) early, we identified which drugs were to be monitored using signal detection and the package insert, and created and applied a protocol to address this.
Methods
Adverse event data recorded in the Japanese Adverse Drug Event Report (JADER) database between April 2004 and January 2018 were used. Among small molecule tyrosine kinase inhibitors that are not described in the serious side-effects section of the package insert despite signal detection, tyrosine kinase inhibitors with severe side-effects in the background of cases reported by JADER database were selected to be monitored in clinical practice. We applied our findings clinically by creating a protocol to detect CTRCD early. All cases at Tosei General Hospital where the target tyrosine kinase inhibitors were administered from when they were first released in November 2019 were included. We compared the results from before and after we began the protocol to clarify its effects.
Results
We found that CTRCD was not described in the serious side-effect section of the package inserts for Bosutinib, Alectinib, and Osimertinib even though CTRCD signals were detected for them. Therefore, it is possible that we may have previously overlooked CTRCD. When we applied our protocol using Osimertinib as the target drug, we were able to detect CTRCD early in 5/21 (24%) patients.
Conclusions
It was clarified that the drug identification method used in this study for early detection of adverse events leads to early detection of adverse events when applied clinically.
Keywords
Introduction
Advances in the early diagnosis and treatment of cancer have significantly improved the prognosis of cancer patients. In particular, in the field of oncology, advances in the understanding of the molecular biology of cancer are revealing the mechanisms of cancer cell growth and metastasis at the molecular level. Targeted molecular therapies have become widely used based on this knowledge. Among them, small molecule tyrosine kinase inhibitors (TKIs) are administered orally; however, ensuring treatment compliance can be a challenge, especially with certain cancer types like chronic myelogenous leukemia. 1 With that said, this treatment contributes to the patient’s quality of life (QOL), e.g. by decreasing the need for invasive procedures such as securing infusion routes in addition to reducing the burden of having to visit the hospital. As such TKIs are developed and applied clinically, and it has become clear that related adverse events with a profile different from that of conventional drugs occur. The reason is that TKIs act at the signal transduction stage leading to cell proliferation and affect organs and tissues depending on the signal transduction pathway. In recent years, there have been many reports of adverse events related to cardiotoxicity and the cardiovascular system (cancer therapeutics-related cardiac dysfunction: CTRCD). 2 -- 4 The expression of CTRCD is rare, but is sometimes a life-threatening or fatal adverse event. In addition, when it is necessary to discontinue chemotherapy due to CTRCD, the prognosis and QOL of cancer patients may be significantly impaired, so early detection and response is vital.
Adverse events identified at the time of clinical trials are described in the package insert, but the trials only include a limited number of cases with simple backgrounds and are only conducted for a limited time. TKIs for which the risk of CTRCD is known from clinical trials such as nilotinib and ponatinib, and for which careful monitoring is recommended in package inserts and other reports, are monitored in clinical practice. 5 However, since they are also used in clinical practice with patients with complicated backgrounds, we were concerned that CTRCD may occur even if it is not described in the package insert, and that it could be overlooked in clinical practice. Therefore, we identified TKIs for which CTRCD may be overlooked using the Japanese Adverse Drug Event Report (JADER) database, and constructed a protocol for the early detection of CTRCD and applied it clinically. The purpose of this paper is to reveal its effects.
Methods
Identifying drugs with possible overlooked CTRCD association
We targeted TKIs that had been released in Japan up until December 2017 that were used in the treatment of cancer and that used monotherapy in principle to avoid the effects of concomitant medications.
Standardized MedDRA Queries (SMQ) and their base language (PT).
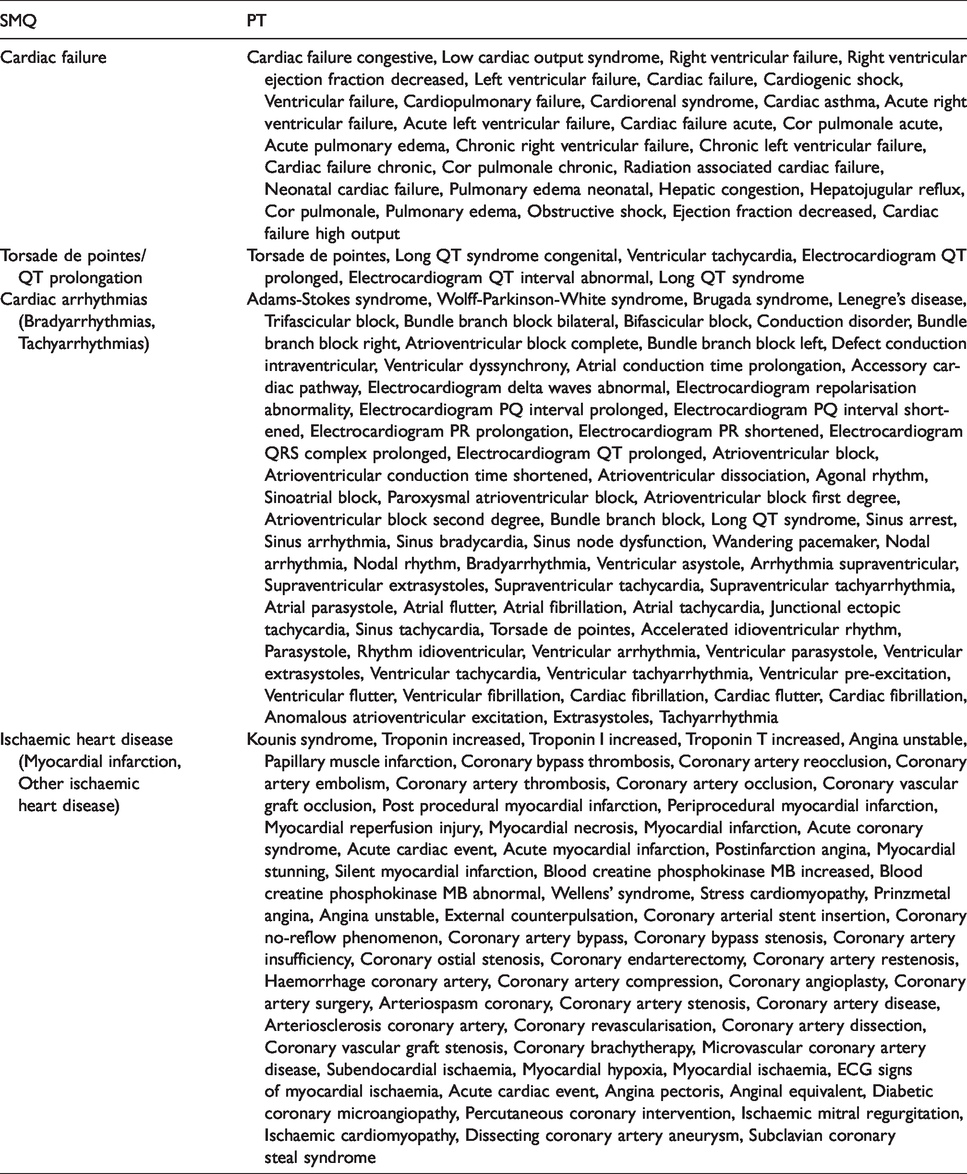
Package inserts are the most familiar source of information for confirming adverse events. Therefore, in order to confirm the current status of CTRCD alerts, we investigated descriptions of cardiac failure, QT prolongation, arrhythmia, and ischemic heart disease in the serious side-effects section of the package inserts, and examined whether or not they were present for the TKIs for which the CTRCD signal was detected.
TKIs where signals for CTRCD were detected, but where cardiac failure, prolonged QT, arrhythmia, ischemic heart disease were not described in the serious side-effects section of the package insert were identified as drugs that where CTRCD risk may have overlooked in clinical practice. To determine the severity of the adverse events for these drugs, we examined patient background, such as: age, gender, primary disease, dose given, adverse events, outcomes, and time to onset of adverse events in the reported cases of adverse events in the JADER database. We selected TKIs where severe adverse events such as fatalities occurred after administration based on our JADER database findings from the TKIs where CTRCD is not described in the serious side-effects section of the package insert despite signals being detected to monitor in clinical practice.
Construction and operational effects of protocol for early detection of CTRCD
CTRCD was defined as cardiac failure, prolonged QT, arrhythmia, and ischemic heart disease. We constructed a protocol for monitoring CTRCD by referring to a position paper published in 2016 by the European Society of Cardiology.
7
We performed echocardiography and electrocardiogram (ECG) as pre-treatment in addition to conventional blood pressure measurements, chest X-rays, and blood tests. Since CTRCD may have already become serious by the time subjective symptoms appear, we decided to perform echocardiographies and ECGs as appropriate (for example every two to three months) to monitor for it during medication administration. If the left ventricular ejection fraction (LVEF) was <50% on the echocardiography and QTc was >500 ms, we decided to withdraw the medication. Because this protocol is intended for early detection, if an echocardiogram shows a decrease of more than 10% from the baseline value of LVEF and a prolongation or abnormal value of more than 60 ms from the baseline value of ECG it is considered to be an early sign of a CTRCD. In that case, we decided to consider drug withdrawal at the discretion of the attending physician (Figure 1
Monitoring protocol for early detection of CTRCD.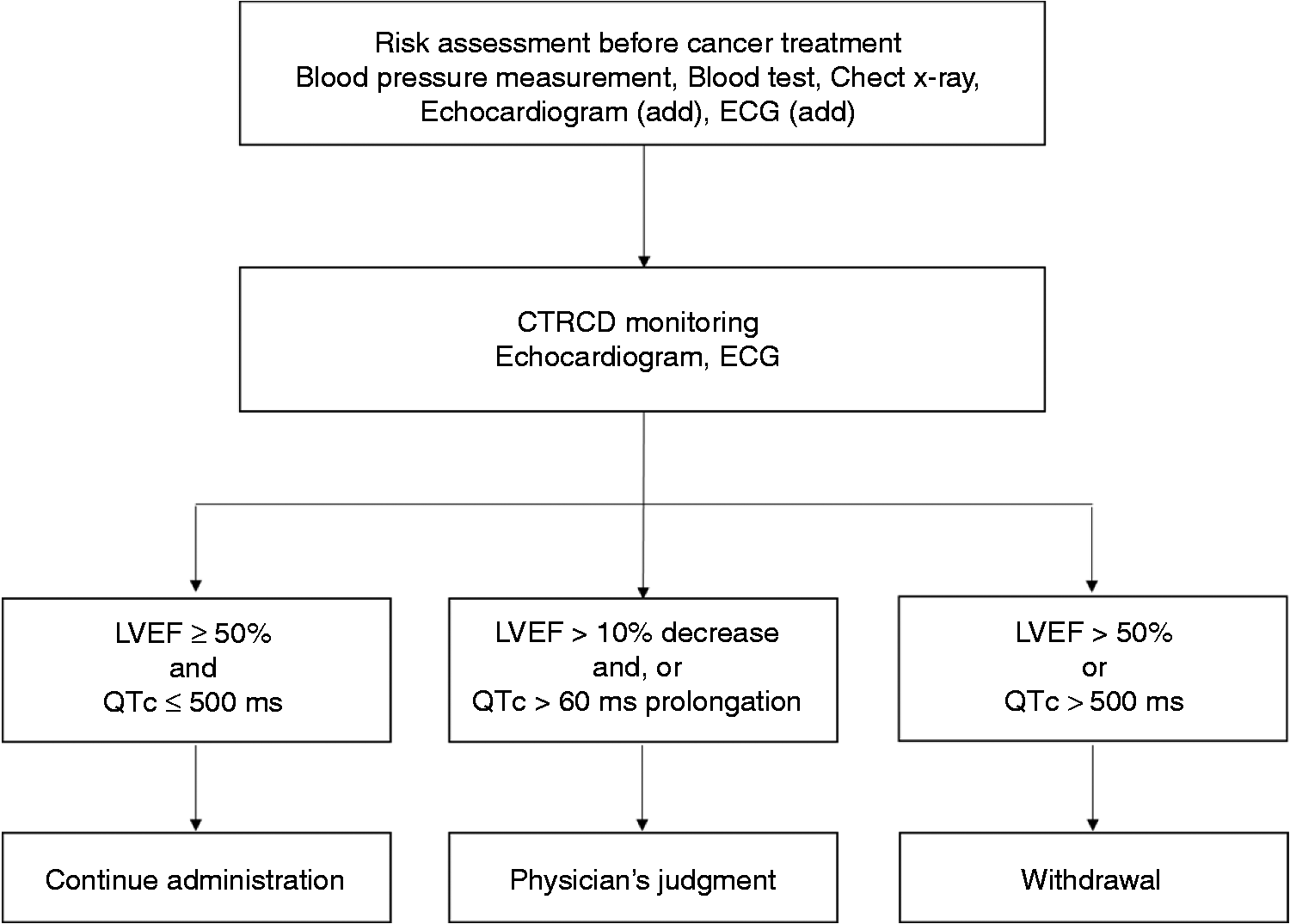
All cases where the target TKIs were administered at Tosei General Hospital (633 beds) from the time they were first administered to November 2019 were included in our study. We compared overall results before and after our protocol was implemented to clarify its effects. The observation period before the protocol was enacted was set as the period from when the target TKIs were first administered to either when administration was discontinued or July 2018. The observation period after we began the protocol in August 2018 was set as the time the target TKIs were first administered to either their discontinuation or November 2019. Cases where treatment was continued before and after we began the protocol were included in the “after protocol” group from August 2018. We used the medical information in this study with the approval of the Tosei General Hospital ethics committee (accession number 822).
We used electronic medical records to retrospectively investigate each patient’s gender, age, performance status (PS), tobacco, and alcohol use. Additionally, we retrospectively investigated their primary diseases, the presence of metastasis and/or gene mutation, risk factors for cardiac dysfunction, initial dose given, treatment line, and observation period. We defined risk factors for cardiac dysfunction as heart disease, hypertension, diabetes, dyslipidemia, and chronic kidney disease. 7 Finally, we did not establish exclusion criteria.
The primary endpoint was the number of CTRCD events found. CTRCD is the occurrence of cardiac failure, prolonged QT, arrhythmia (without prolonged QT), and ischemic heart disease. The occurrence of cardiac failure was assessed by an LVEF of <50%, a decrease of more than 10% from the baseline value of LVEF or by physician diagnosis. The occurrence of QT prolongation was assessed by a QTc > 500 ms, prolonged of more than 60 ms from the baseline value of the ECG. The occurrence of arrhythmia (without prolonged QT), and ischemic heart disease was assessed by detection of abnormal values with an ECG or was diagnosed by a doctor. We conducted a retrospective survey using electronic medical records.
Secondary endpoints included TKI discontinuation, withdrawal, reduction and the reasons for those things, echocardiographic values, ECG values, and subjective symptoms of cardiac dysfunction such as palpitations, shortness of breath, dyspnea, swelling, and the presence of chest pain. These subjective symptoms conducted a retrospective survey using electronic medical records.
Sunitinib, which is considered to have the highest frequency of CTRCD out of all TKIs, has a maximum frequency of left ventricular dysfunction at 19%. 7 Therefore, we assumed that the CTRCD discovery rate before we began the protocol was 0%, and that the discovery rate would increase by about 20% after it began. The sample size was calculated with a one-sided α error of 5%, a detection rate of 80%, and an allocation of 1:2. From the results of our calculations, we thought that we needed 22 patients before the protocol started, and 44 patients after it began.
We examined the independence between groups using the Student’s t-test or the Mann–Whitney U-test for continuous variables and Fisher’s exact test for categorical data. Statistical analysis was performed using SPSS v25 (IBM Japan, Tokyo).
Results
Identifying drugs with possible overlooked CTRCD associations
The total number of TKI reports made in the JADER database during the analysis period was 504,407.
Relationship between signal detection and description of serious side-effects in the package inserts.
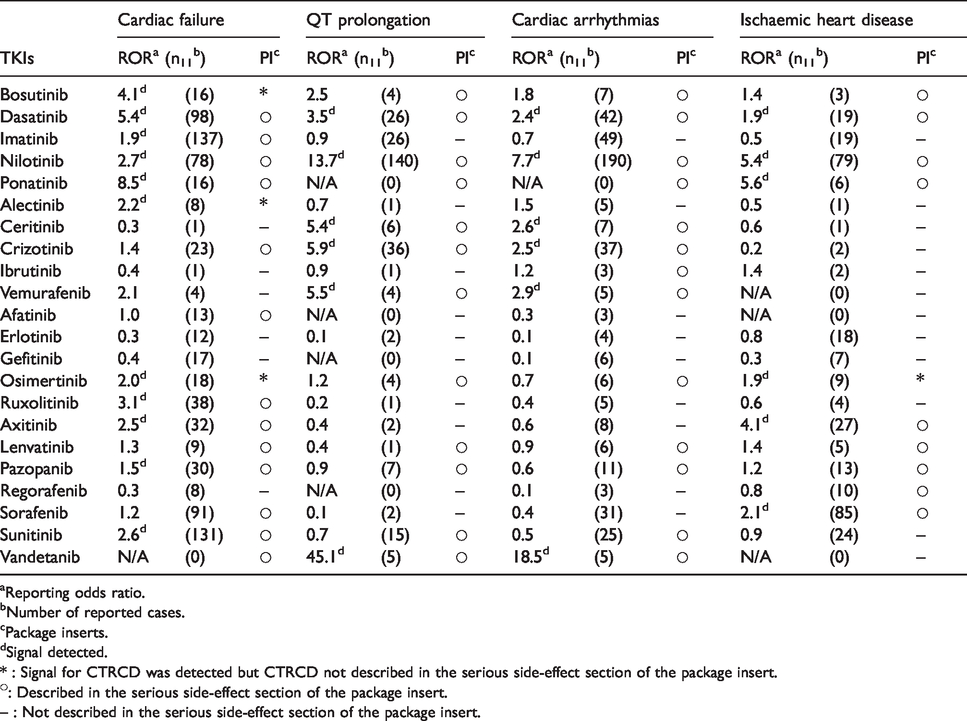
Reporting odds ratio.
Number of reported cases.
Package inserts.
Signal detected.
* : Signal for CTRCD was detected but CTRCD not described in the serious side-effect section of the package insert.
: Described in the serious side-effect section of the package insert.
– : Not described in the serious side-effect section of the package insert.
Details from JADER database reports on Bosutinib where cardiac failure occurred.
Details from JADER database reports on Alectinib where cardiac failure occurred.
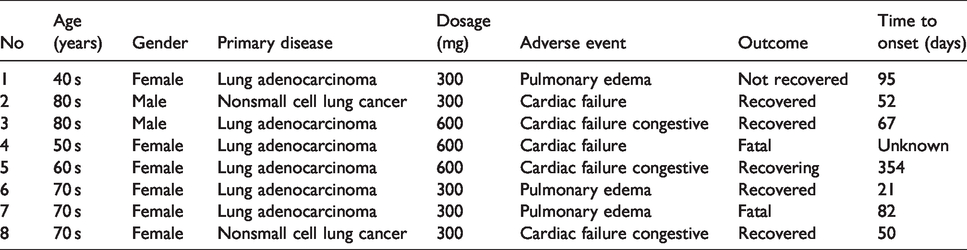
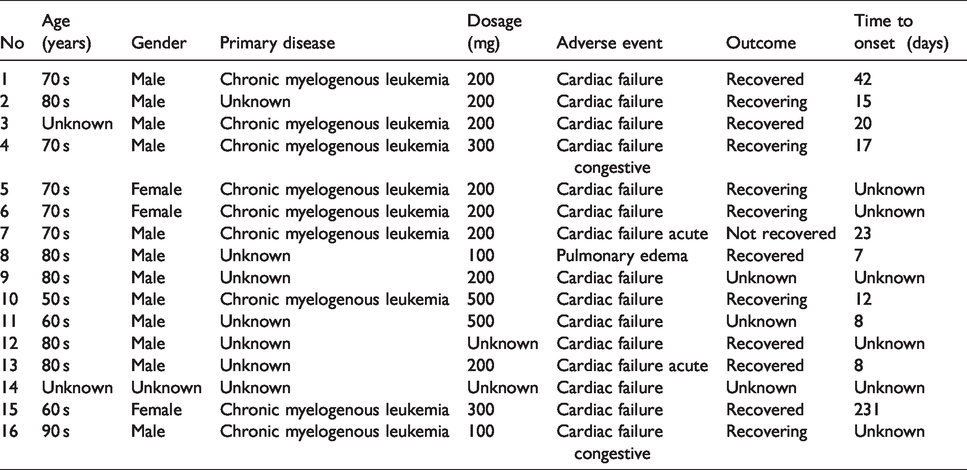
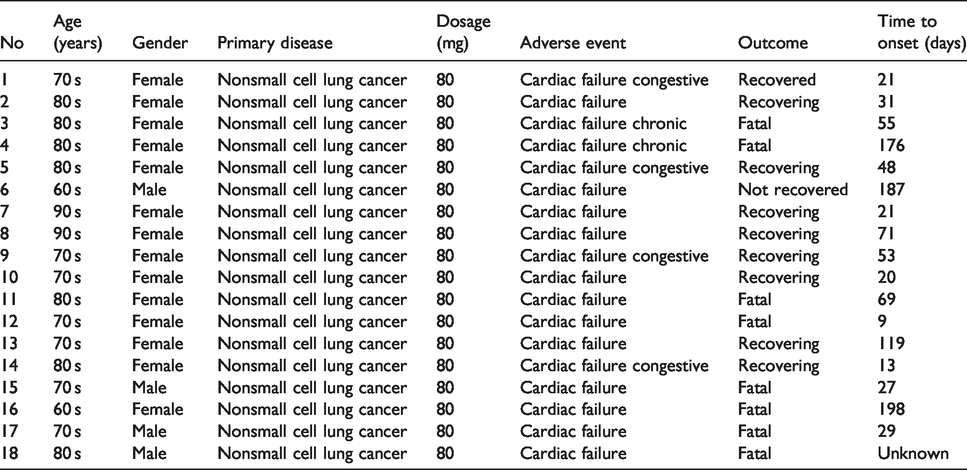
Details from JADER database reports on Osimertinib where cardiac failure occurred.
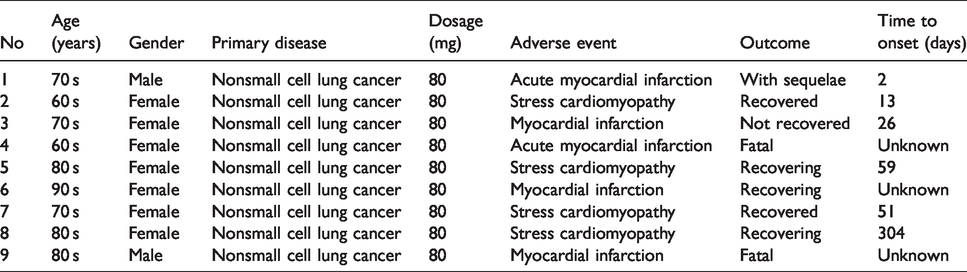
Details from JADER database reports on Osimertinib where Ischaemic heart disease occurred.
Application and effects of protocol for early detection of CTRCD
Patient population and characteristics
Patient characteristics.
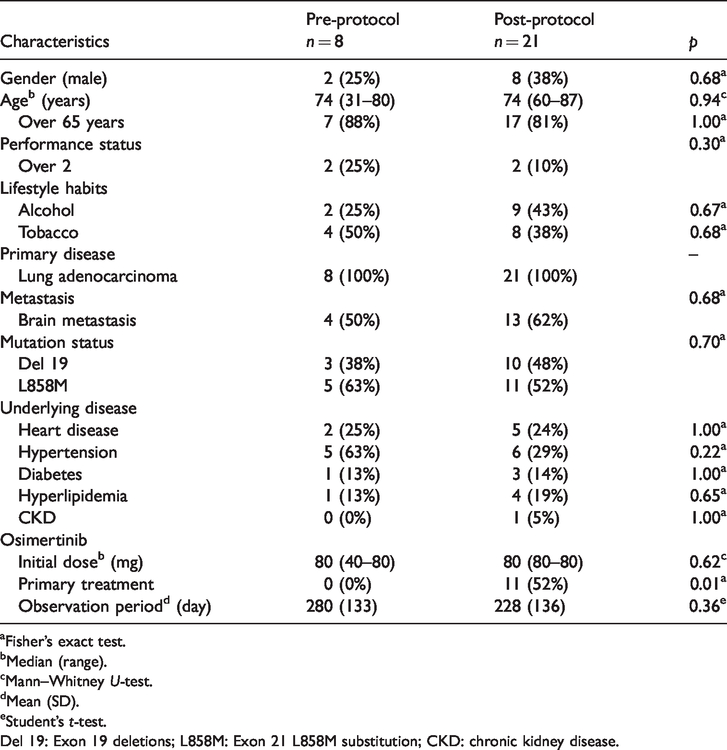
Fisher’s exact test.
Median (range).
Mann–Whitney U-test.
Mean (SD).
Student’s t-test.
Del 19: Exon 19 deletions; L858M: Exon 21 L858M substitution; CKD: chronic kidney disease.
Primary endpoints
Number of CTRCDs found with osimertinib.
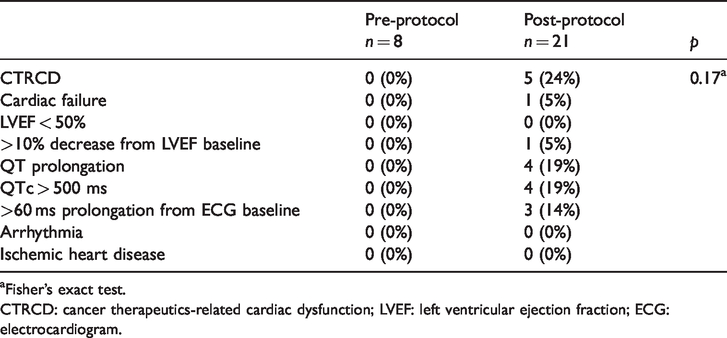
Fisher’s exact test.
CTRCD: cancer therapeutics-related cardiac dysfunction; LVEF: left ventricular ejection fraction; ECG: electrocardiogram.
Secondary endpoints
Effects of protocol.
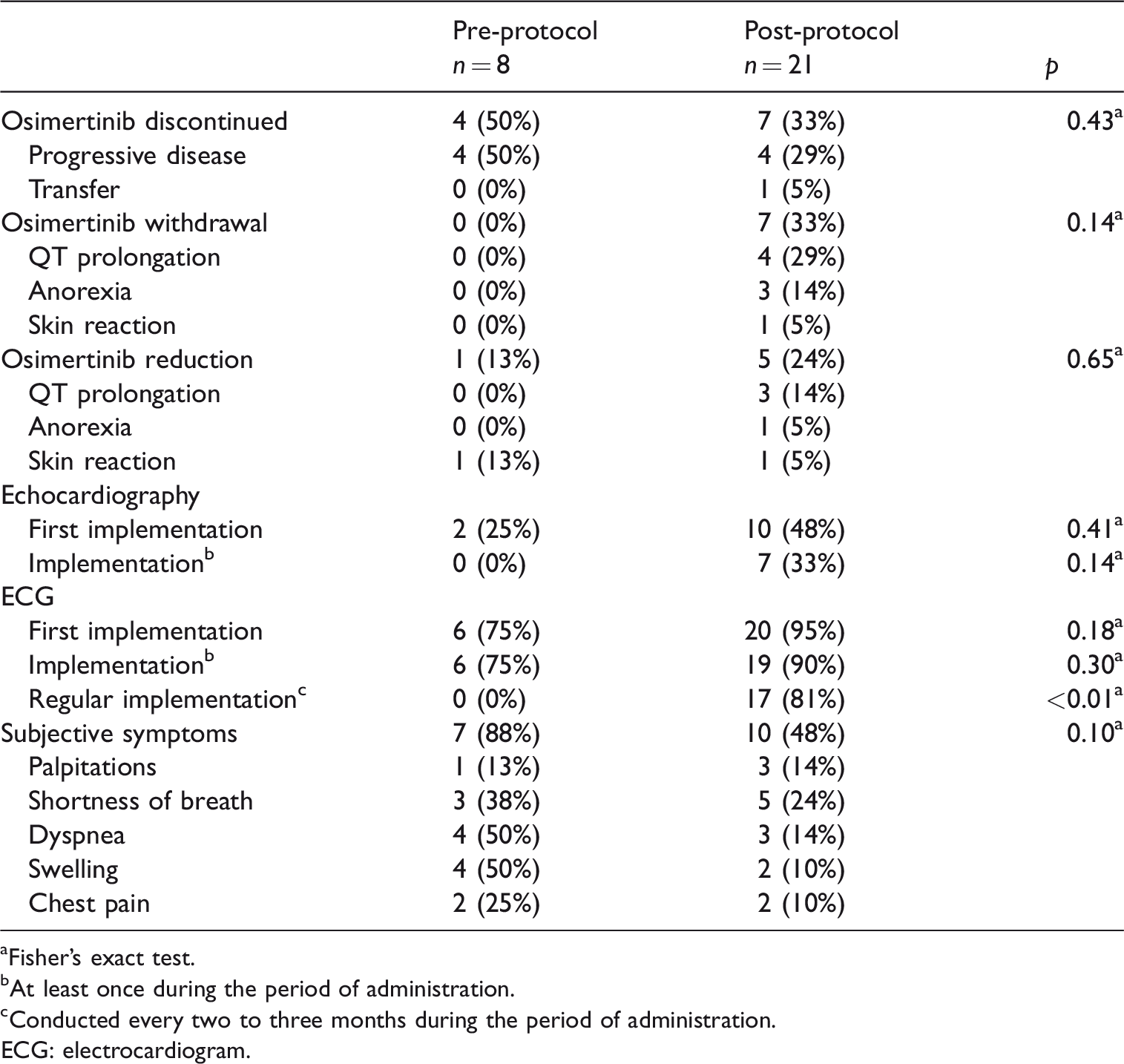
Fisher’s exact test.
At least once during the period of administration.
Conducted every two to three months during the period of administration.
ECG: electrocardiogram.
Discussion
With the aging of the population and considering that cancer is the first most common cause of death in Japan and cardiovascular disease the second, it can be assumed that many patients have cancer and cardiovascular disease at the same time. As various new TKIs are developed and clinically applied, CTRCD rates are expected to increase in the future. Against this backdrop, an interdisciplinary field called Onco-Cardiology (or Cardio-Oncology) has recently been established, and its system is being rapidly developed, mainly in Europe and the United States. In addition, it is expanding not only in clinical practice but also as a comprehensive academic field involving basic and clinical medicine.7,>8 However, the number of cardio-oncologists and the referral process are still far from sufficient.
In clinical practice, package inserts created from clinical trial data are the most familiar source of information. In recent years bridging tests have been conducted before new drugs are approved, and there is a tendency for information about Japanese patients obtained before approval to be limited. Therefore, whether in regard to CTRCD or not, the package insert alone is not sufficient to identify drugs that may need early detection of adverse events, and it is considered necessary to also consider the clinical use results and their severity.
The indication for Osi, which was identified by this study as primary treatment, was expanded from August 2018. In fact, primary treatment accounted for about half of 11/21 patients (52%) after the protocol began, and the number of cases increased compared to prior to the protocol which used to only be applicable if the T790M mutation was positive. Since the number of patients taking Osi is expected to increase in the future, we need to monitor signs of CTRCD carefully in clinical practice.
Signals for cardiac failure that were not described in the serious side-effects section of the package insert were detected for Osi. Therefore, we worked on putting a protocol in place to address this in clinical practice. As a result, we found an adverse event that was not identified in clinical trials where the LVEF decreased by more than 10% from the baseline value. Osi also has an inhibitory action on HER2 (ErbB2), 9 a subfamily of EGFR, suggesting the possibility that it causes left ventricular dysfunction by the same mechanism as Trastuzumab. 10 In addition, since the case report of the onset of cardiac failure due to the use of Osi have been reported in recent years, 11 we believe that it is necessary to evaluate cardiac function by echocardiography as appropriate. In our study, we found that although the LVEF decreased more than 10% from the baseline value, it did not reach <50%, and thus Osi was not withdrawn. However, if we had overlooked this, it is possible that severe cardiac failure might have occurred, so the protocol led to early detection of an unknown adverse event, cardiac failure.
QT prolongation and arrhythmia are noted in the serious side-effects section of the Osi package insert; however and no signals of them were detected despite being noted as important identified risks in the Risk Management Plan. QT prolongation and arrhythmia have few subjective symptoms in their early stages, and are difficult to detect unless an ECG is taken. Therefore, we may not have been able to report them due to the lack of regular ECG monitoring in clinical practice, and they were likely to have been overlooked until serious conditions such as cardiac failure occurred. Although the results are from a single facility, the rate of regular ECGs being taken every two to three months was low before the protocol began. Considering that more than half of the cases of cardiac failure, an unknown adverse event, occurred within three months of Osi administration according to the JADER database reports, it was suggested that we may not have been adequately monitoring ECGs. After the protocol began, the implementation of regular ECGs every two to three months increased significantly. As a result, QT prolongation was discovered. These facts suggest that we were able to detect and respond early to side-effects before more serious adverse events such as cardiac failure occurred. In addition, the frequency of QT prolongation was noted as 6.1% on the Osi package insert, but was found in 19% of the cases we studied after the protocol was put into place. This suggests that the frequency of CTRCD expression in clinical practice is high, and the possibility that CTRCD, including QT prolongation, occurred before the protocol began cannot be denied. Therefore, the importance of using our protocol in clinical practice was suggested.
A signal for ischemic heart disease was detected for Osi, although it was not described in the serious side-effects section of the package insert, but we did not see ischemic heart disease during the observation period. Since about half of the reports from the JADER database could not be judged to be coronary artery disease such as stress-type cardiomyopathy, we need to accumulate more cases in clinical practice in the future.
Although there was no significant difference in the data during the discontinuation of Osi, there was a tendency to withdraw it after our protocol began. Echocardiography, especially regular ECG monitoring, was significantly improved after our protocol was put into place, suggesting that the early detection of CTRCD while utilizing the protocol may have led to early responses such as withdrawal or reducing the dosage of Osi. Because the subjects are patients with lung adenocarcinoma, shortness of breath and dyspnea may simply be the result of worsening disease, and the possibility that those symptoms were common before we utilized our protocol, which is only for nonprimary treatment, cannot be ruled out. However, we cannot deny the possibility that CTRCD was lurking due to insufficient monitoring before our protocol began. Therefore, it was suggested that early detection and early response before the adverse event occurred could have led to a reduction in subjective symptoms after the protocol was enacted.
It was clarified that the drug identification method used in this study for early detection of adverse events may lead to early detection of adverse events when applied clinically. Therefore, it was suggested that the results obtained by this research method could be used in clinical practice to supplement the package insert.
However, there are limitations to consider regarding the results obtained in clinical practice. In this study we actually discovered an unknown adverse event, cardiac failure. Additionally, in December 2019 the package insert of Osi was revised, and congestive cardiac failure and reduced LVEF were added to the serious side-effects section. For these reasons, we stopped observation without waiting for a certain number of cases undergoing our protocol to be completed. Therefore, we could not show the superiority of our protocol. However, the revised package insert supported the usefulness of our research method, and we think that this research method should be published early and extended to other fields. It is a single center, comparative study. However, it is only applicable if the T790M mutation is positive before the protocol begins, and it is difficult to collect more cases. Conducting a cohort study was also considered to be challenging because the efficacy of the protocol is clear. In this study, echocardiographies and ECGs were used for CTRCD monitoring, but the use of serum biomarkers for early detection should be considered in the future. However, we were able to use the protocol to detect CTRCD early. These results suggest that not only could serious adverse events in patients receiving Osi be prevented, but also that appropriate chemotherapy withdrawal and reduction could prevent unnecessary interruption of chemotherapy. Therefore, it was suggested that it may contribute to the improvement of the life prognosis and QOL of cancer patients.
Conclusions
In this study, we identified TKIs that needed to be monitored to help detect CTRCD early using signal detection and by matching the signals detected with the serious side-effects noted in the package insert. Osi was identified as one such drug with this research method. Because the Osi package insert was later revised to include CTRCD it became clear that this research method may be able to quickly identify unknown and serious adverse events and lead to their early monitoring in clinical practice. In addition, by selecting target drugs and target adverse events, we can identify drugs that may need to be monitored to help detect various adverse events early, and are they expected to have clinical applications thereafter. Therefore, our research has led to the construction of new information.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.