
Abstract
Introduction
Blinatumomab is a CD19/CD3 bispecific T-cell engager (BiTE) antibody that simultaneously binds CD19 on the surface of B-cells and CD3 on the surface of T-cells, resulting in tumor cell lysis. It is approved for the treatment of patients with relapsed/refractory B-cell acute lymphoblastic leukemia (B-ALL) and in patients with minimal residual disease after intensive induction chemotherapy. Relapse patterns after treatment with blinatumomab have not been well characterized.
Methods
We reviewed patients treated with blinatumomab with relapsed, refractory or minimal residual disease-positive B-ALL from 1 December 2014 to 31 December 2018 at a single academic medical center. Patient demographics, blast percentage prior to blinatumomab initiation, prior lines of therapy, blinatumomab treatment duration, sites of relapse, progression free survival, and overall survival were collected.
Results
A total of 20 patients were identified. Four (20%) patients developed extramedullary relapse following blinatumomab. The median time from treatment initiation to extramedullary relapse was 179 days (range 47–241). Sites of extramedullary relapse included the pancreas, adrenal gland, kidneys, liver, parotid gland, and brain.
Conclusion
Extramedullary relapse occurs frequently following treatment of B-ALL with blinatumomab. Further studies aimed at preventing extramedullary relapse following blinatumomab treatment are warranted.
Introduction
Blinatumomab is a CD19/CD3 bispecific T-cell engager (BiTE) antibody that binds CD19 on B lineage cells to CD3 on the surface of T cells. 1 This mechanism activates cytotoxic T cells to redirect its target for CD19 malignant cells, resulting in the lysis of tumor cells.1,2 In 2014, the Food and Drug Administration (FDA) granted blinatumomab accelerated approval for the treatment of relapsed or refractory B-cell acute lymphoblastic leukemia (B-ALL). Approval was based on a multicenter phase II study, which demonstrated a complete response (CR) or partial hematological recovery (CRh) in 43% of patients with at least two cycles of single-agent blinatumomab. 3 The subsequent phase III trial later demonstrated a significantly longer median overall survival (OS) with blinatumomab compared to standard-of-care chemotherapy in heavily pre-treated B-ALL patients. Rates of CR/CRh, event-free survival, and duration of remission were also significantly higher in the blinatumomab arm. 4
More recently, blinatumomab was granted approval for treatment of B-ALL in adults and children who are in remission but still have minimal residual disease (MRD). 5 MRD, defined as the presence of ≥ 0.01% leukemic cells, occurs in approximately 30–50% of patients in CR after combination chemotherapy and is associated with a high risk for relapse.5,6
Although outcomes for B-ALL patients have improved over the past several decades due to the introduction of novel therapeutics, relapse still occurs in a large proportion of adult patients despite allogeneic stem cell transplantation (allo-SCT). 7 Studies have reported relapse rates ranging between 30% and 70% following allo-SCT.8,9 The majority of relapses occur in the bone marrow; however, extramedullary (EM) relapse has also been reported in B-ALL and can occur as isolated sites or in combination with marrow relapse. While EM relapse data in adult B-ALL are limited, available literature demonstrates that most EM disease occurs following allo-SCT.9,10 Previous retrospective studies report a cumulative incidence of EM relapse ranging from 6% to 23% following allo-SCT, either as isolated relapse or with bone marrow involvement.9–11 EM relapse following allo-SCT is thought to be due to immune invasion by leukemic blasts.11–13 Cytotoxic CD8 T-cells are responsible for the graft-versus-leukemia effect in the post-transplant setting; however, in immune privileged sites, these cells are reduced, allowing for EM relapse to occur. 13
Several case reports have described unusual relapse patterns following blinatumomab to uncommon sites including the lungs, lymph nodes, kidney, and spleen.14–16 Only one study has presented a detailed analysis of EM relapse, treatment failure, and resistance patterns after blinatumomab treatment at a single institution. Aldoss et al. 15 reported EM relapse in 40% of their patients who subsequently relapsed after blinatumomab. The purpose of this study is to further characterize the clinical patterns of EM relapse after blinatumomab treatment for B-cell ALL.
Methods
The electronic medical record was reviewed for patients with relapsed/refractory or MRD-positive B-cell ALL treated with blinatumomab at the University of California, San Diego Health (UCSDH) between 1 December 2014 and 31 December 2018. Patients receiving blinatumomab for indications other than relapsed/refractory or MRD-positive B-ALL and patients who received blinatumomab combined with other agents were excluded. Patient demographics, blast percentage prior to blinatumomab initiation, prior lines of therapy, blinatumomab treatment duration, EM relapse location, allo-SCT type (if applicable), chimeric antigen receptor T-cell (CAR-T) therapy (if applicable), progression free survival (PFS), and OS were collected. Patient demographics and disease characteristics were analyzed using descriptive statistics. The study was approved by the Institutional Review Board (IRB).
Results
Twenty eligible patients with relapsed/refractory or MRD-positive ALL who were treated with blinatumomab were identified. Patients were excluded from analysis for the following reasons: one received blinatumomab for diffuse large B-cell lymphoma (DLBCL), two patients received blinatumomab as part of upfront B-ALL treatment, and one patient received concurrent treatment with blinatumomab and pembrolizumab as part of a clinical trial (Figure 1). The median age at the time of treatment was 57.5 years (range 22–80). At the time of data censoring, 10 of 20 (50%) patients were deceased. The median overall survival was 61.5 days (range 13–607). Patient demographics are summarized in Table 1.
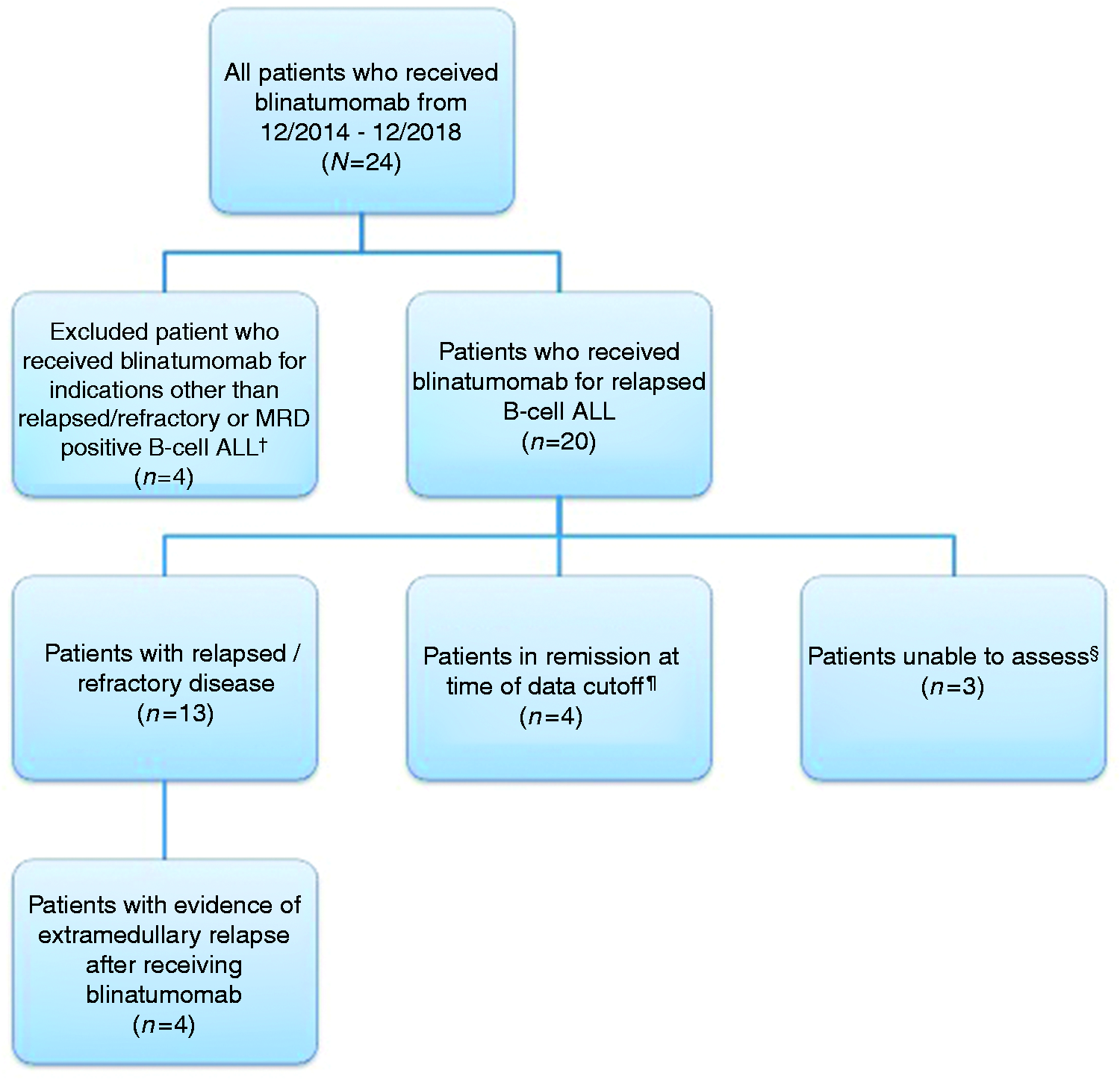
Flowchart of patient study selection.
Patient demographics.
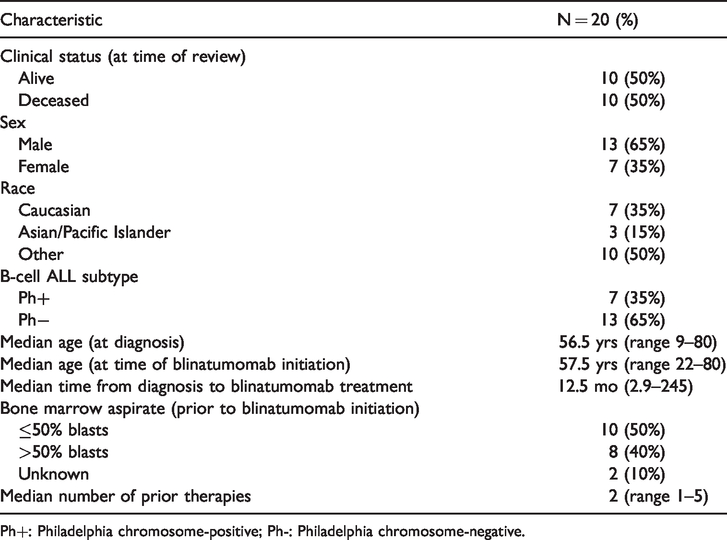
Ph+: Philadelphia chromosome-positive; Ph-: Philadelphia chromosome-negative.
Two patients did not have available blast count information from bone marrow biopsies prior to blinatumomab initiation. Among the 10 (50%) patients with ≤50% blasts prior to blinatumomab treatment, five patients were MRD-positive. Five (25%) of the 20 patients discontinued blinatumomab shortly after treatment initiation and remained in relapsed/refractory disease. Reasons for treatment discontinuation included the following: deceased (n = 1), neurotoxicity (n = 1), leukocytosis (n = 2), and patient preference (n = 1) (Figure 1).
Relapsed or refractory disease occurred in 9 (45%) of the 20 patients. The median time from blinatumomab initiation to time of relapse was 47 days (range 13–342). We were not able to assess three patients for evidence of relapsed disease due to loss of follow-up. Four (20%) patients currently remain in remission at the time of data censoring, with a median remission time of 349 days (range 208–637 days).
EM relapse occurred in 4 (20%) of our total 20 patients. The median time from blinatumomab initiation to evidence of EM disease was 179 days (range 47–241). The most common site of relapse was the lymph nodes, which occurred in three of the patients. These patients did not have lymph node involvement prior to blinatumomab. Other sites of EM relapse included the parotid gland and parenchyma of the brain. One patient with EM disease in the lymph node was found to also have involvement in the parotid gland seven months later. Patient characteristics with EM relapse are summarized in Table 2.
Patients with extramedullary relapse.
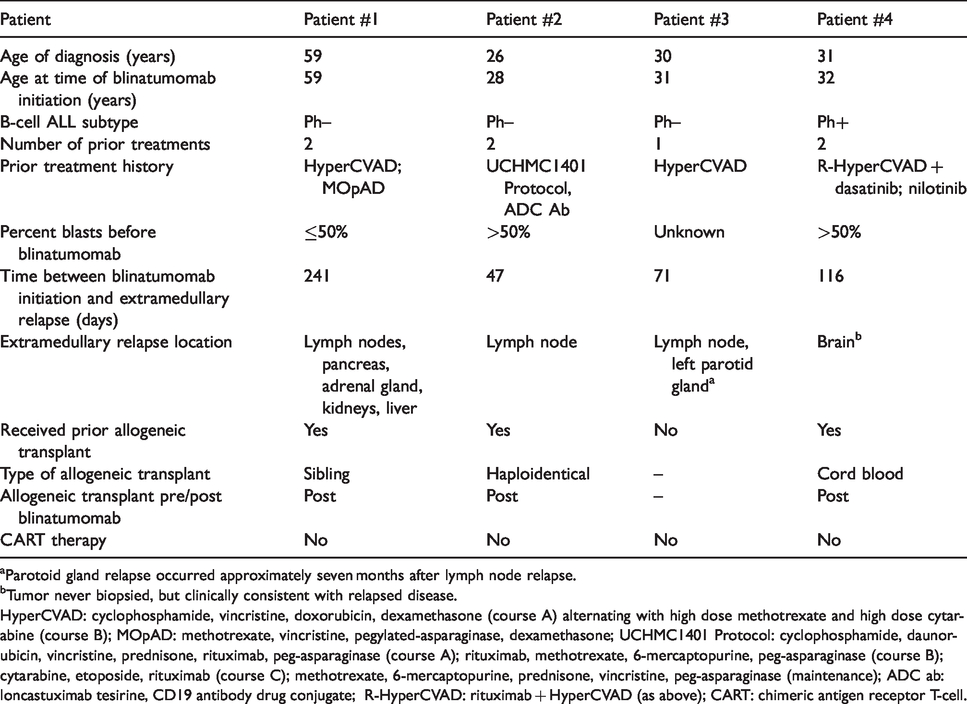
aParotoid gland relapse occurred approximately seven months after lymph node relapse.
bTumor never biopsied, but clinically consistent with relapsed disease.
HyperCVAD: cyclophosphamide, vincristine, doxorubicin, dexamethasone (course A) alternating with high dose methotrexate and high dose cytarabine (course B); MOpAD: methotrexate, vincristine, pegylated-asparaginase, dexamethasone; UCHMC1401 Protocol: cyclophosphamide, daunorubicin, vincristine, prednisone, rituximab, peg-asparaginase (course A); rituximab, methotrexate, 6-mercaptopurine, peg-asparaginase (course B); cytarabine, etoposide, rituximab (course C); methotrexate, 6-mercaptopurine, prednisone, vincristine, peg-asparaginase (maintenance); ADC ab: loncastuximab tesirine, CD19 antibody drug conjugate; R-HyperCVAD: rituximab + HyperCVAD (as above); CART: chimeric antigen receptor T-cell.
Discussion
This analysis demonstrates a 20% risk of EM relapse in patients receiving blinatumomab for relapsed/refractory or MRD-positive B-ALL. EM relapse following blinatumomab treatment has been described in a limited number of reports (Table 3).14–18 Aldoss et al. found EM relapse in 21 (32%) of 65 patients in a retrospective analysis, which included 13 of 32 (41%) patients refractory to treatment and 8 of 20 (40%) patients who responded but eventually relapsed to blinatumomab. Sites of relapse included the kidney, central nervous system (CNS), lymph node, muscle, chest wall, and nasopharynx. 15
Literature summary of patients with EM relapse after blinatumomab for B-ALL.
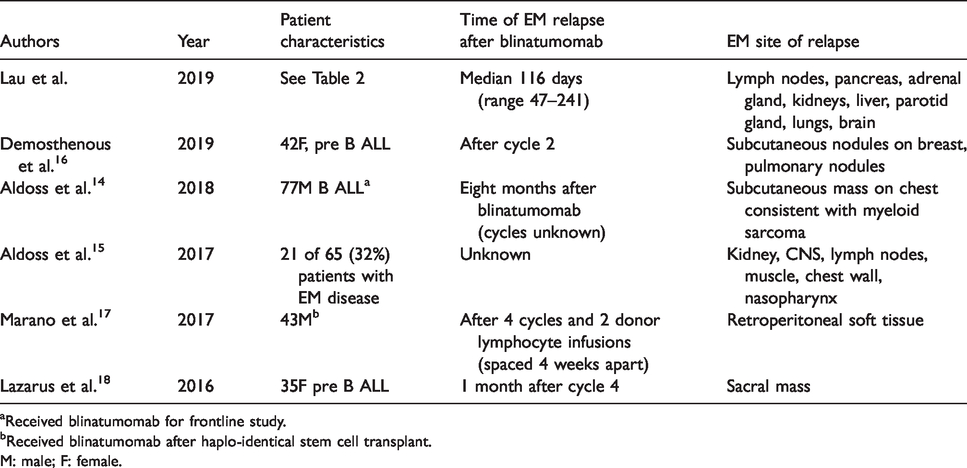
aReceived blinatumomab for frontline study.
bReceived blinatumomab after haplo-identical stem cell transplant.
M: male; F: female.
EM relapse following allo-SCT has been extensively described in the literature, but reports of this phenomenon following blinatumomab are less characterized. In the allo-SCT setting, cytotoxic CD8 T-cells are responsible for the graft-versus-leukemia effect but are reduced or not able to penetrate in some tissues.11–13,16 There have been literature reports demonstrating a lack of donor cytotoxic T cells at sites of EM relapse post allo-SCT. 16 The exact mechanism of immune evasion remains unknown, but postulated theories include T-cell energy, preferential T-cell homing, or reduced costimulatory molecules.13,16 The mechanism of EM relapse post blinatumomab also remains poorly understood. However, it is likely that a similar type of immune evasion occurs. As T-cells may be reduced in specific tissue sites, blinatumomab cannot engage CD19 malignant cells with CD3 T cells to direct cell death. The lack of anti-tumor activity in these areas may possibly result in EM relapse or progression later on.
Of the four patients who demonstrated EM relapse in the present analysis, one patient presented with Philadelphia chromosome-positive (Ph+) disease. Ph+ B-ALL has been associated with poor prognosis, but it is unknown whether this high-risk subtype predicts EM relapse in patients who received blinatumomab. However, in patients with relapsed disease post allo-SCT, Lee et al. 11 found a significant correlation between Ph+ acute leukemia and EM relapse. Further studies are needed to identify risk factors for EM relapse after blinatumomab.
This study has several limitations. First, it is a retrospective, single center study, with a limited number of patients. In addition to a few patients loss to follow-up, some of our patients discontinued blinatumomab shortly after treatment initiation and remained in relapsed/refractory disease. These patients were grouped with the relapsed/refractory during data analysis. Given the short time frame on this treatment, some of these patients may not have been considered truly refractory to blinatumomab therapy. Our population was also heterogeneous and included both MRD-positive and refractory patients. It remains unknown if EM relapse is more likely in relapsed disease vs. MRD-positive disease. Finally, we did not assess for loss of CD19 expression at relapse. This mechanism of relapse has been observed after CD19-directed targeted therapies that include blinatumomab and chimeric antigen receptor (CAR) T-cell therapy.19,20 Aldoss et al. found a significantly greater reduction in CD19 expression at the time of relapse in responders compared to refractory cases. The expression of CD19 among patients with EM disease was not reported. 15 Another recent case report described discordant CD19 expression in a patient who developed EM relapse on the left breast and lung. At the time of EM relapse, a bone marrow aspiration showed CD19-negative cells; however, CD19 expression later reappeared after chemotherapy was given to the patient. 16
Our findings further confirm that EM disease can occur after treatment with blinatumomab. Our EM relapse rate of 20% was lower than the rate reported previously. Aldoss et al. found EM progression in 41% of refractory B-ALL cases. In responders, they found 61% of patients subsequently relapsed, among which EM disease occurred in 40% of patients. 15 Further studies to elucidate the mechanism behind blinatumomab associated EM and decreasing this risk in B-ALL patients are warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Goodman receives speaking fees from Seattle Genetics and consulting fees from Daiichi Sankyo, Kyowa Kirin, and EUSA Pharma.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.