
Abstract
Objective
The purpose of our study was to evaluate the contribution of an automated drug dispensing system in securing cancer chemotherapy production process at the pharmacy of the National Institute of Oncology in Rabat.
Methods
The failure modes and effects analysis method was applied to the chemotherapy production process in two phases: Phase 1, using an open shelf for storage then phase 2, using an automated drug dispensing system. The failure modes were defined and their criticality indexes was calculated on the basis of the likelihood of occurrence, the potential severity for the patients and/or the impact on the process and the detection probability. The criticality indexes of the two phases were prioritized and compared.
Results
We identified 35 failure modes for phase 1 and 37 for phase 2. The sum of criticality indexes was 5957 and 4586, respectively, for phase 1 and phase 2, corresponding to a criticality reduction of −23%. The greatest improvements concerned that the needed drug is missing during the picking, storage of potential expired drugs, and double compounding.
Conclusion
Our study highlighted the contribution of automated drug dispensing system in risk minimization. The use of automated drug dispensing system is a part of security improvement in chemotherapy production unit.
Keywords
Introduction
Chemotherapy cancer process is a complex process. 1 In general, it is formed of three main steps: protocol prescribing, chemotherapy production and administration. 2 Chemotherapy production step appears to be crucial in the care of cancer patients, both for the effectiveness of care and patient safety. However, the chemotherapy production process is not immune to medication errors (ME). ME is defined as a deviation from what should have been done during the therapeutic drug management of the patient.3,4 It is used to refer to an unintentional omission or completion of a medication act which may cause a risk or an adverse event for the patient. By definition, ME is avoidable.3,4 Many errors are made in the production step of chemotherapy process. 5 According to Ashokkumar et al., 6 chemotherapy MEs ranged from 0.40% to 0.50% in the production step. These errors can be for example incorrect volume or type of diluent, incorrect drugs, wrong patient-specific drug label. 7 They can lead to ineffective treatment or serious damage to patient’s health.
Risk reduction in the cancer chemotherapy process has become a major objective for all hospitals. 8 In fact, the number of cancer cases worldwide is constantly increasing.9,10 In Morocco, the annual national cancer incidence rate is estimated at 30,500 new cases of cancer per year, including 16,775 new cases for women and 13,725 new cases for men. 11 The more the number of cancer patients increases the more the quantity of chemotherapy compounding increases and the risk of error increases.12,13 To deal with this situation, the National Institute of Oncology in Rabat (NIO) after centralizing the chemotherapy production process at the centralized chemotherapy production unit (CCPU) of the pharmacy in 2012 14 and computerizing the process introduced an automated drug dispensing system (ADS) in December 2019. Many studies were interested in the contribution of centralization and computerization in the risk minimization of chemotherapy production process.8,15,16 Some studies showed that the centralization of chemotherapy production process at the pharmacy allowed risk reduction of the process around 25%.4,15,16 The use of technology information (computerized prescription, code bar for each patient) allowed risk reduction around 20% compared to the centralized non-computerized system. 16
The aim of our study is to evaluate the contribution of ADS in the risk minimization of chemotherapy production process through risk analysis using the failure modes and effect analysis (FMEA) method.
Materials and methods
Setting of the study
Our study is a comparative risk analysis in two phases. The study took place at the hospital pharmacy of NIO in Rabat. NIO is a reference center for the treatment of cancer in Morocco and Africa. On an average, 3000 cytotoxic preparations were made per month in the CCPU. 14 The risk analysis concerned the chemotherapy production step in the chemotherapy process.
Phase 1
In phase 1, the pharmaceutical validation and the labelling were computerized using the medical software named ENOVA. The storage and picking of raw materials are done using an open storage shelf. Drugs were stored according to the frequency of use. Compounding operations are carried out in two laminar flow hoods extemporaneously for workdays and in advance for weekends. A final control by a visual double check was done before the delivery of the product to care service. Figure 1 describes the chemotherapy production process at NIO.
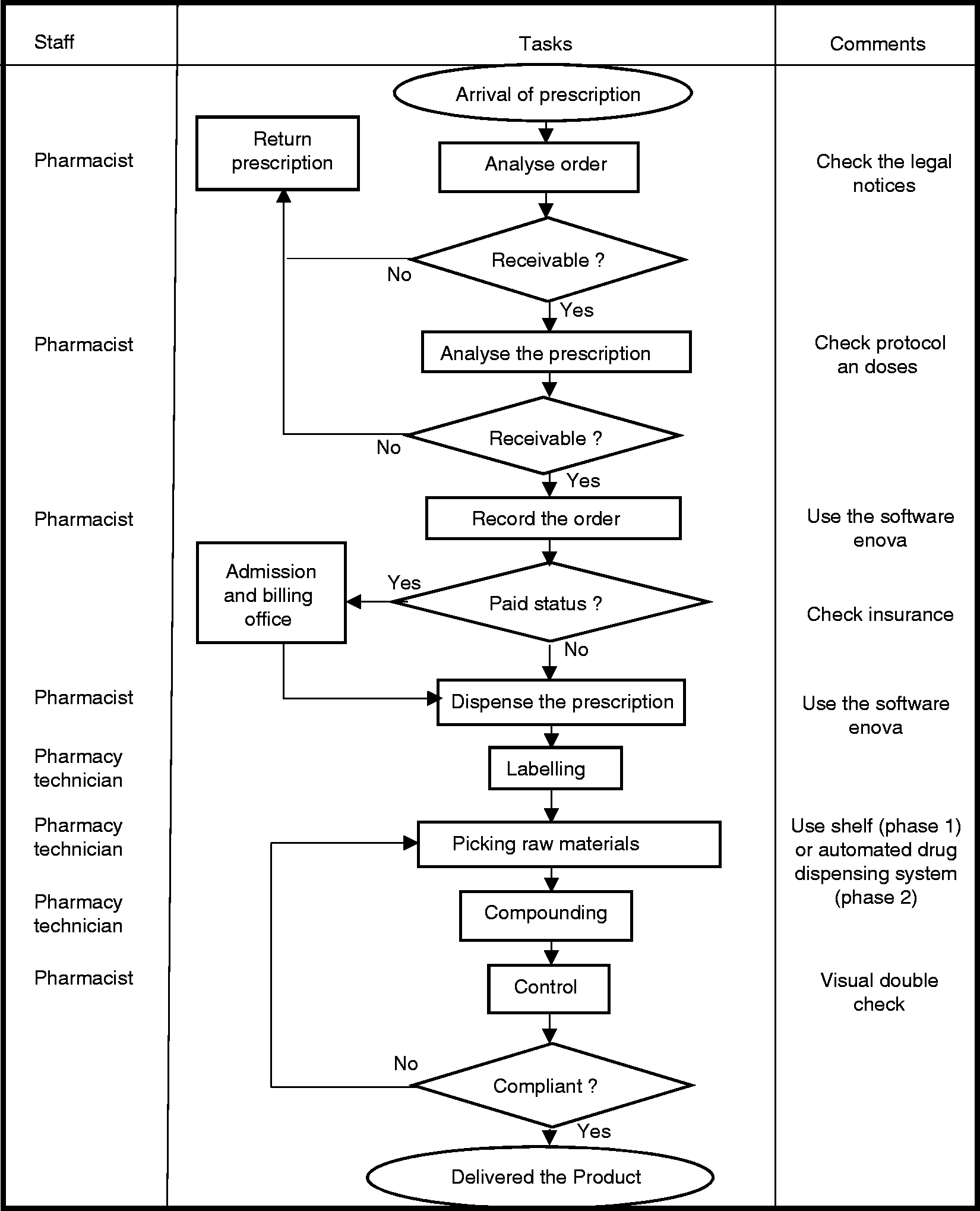
Chemotherapy production process at the National Institute of Oncology in Rabat.
Phase 2
In phase 2, the process was the same (Figure 1), it was computerized with instructions on ADS, and compounding operations and control were done with the same organization. The major difference was the use of ADS in this phase instead of the shelf. The ADS of our CCPU was STOCKART type. The ADS was interfaced with the patient’s barcode and with the software (ENOVA) for prescription, pharmaceutical validation and stock management. Several access levels are configured according to the user’s authorization (pharmacist, pharmacy technician, pharmacy resident, maintainer). Users can access their session after recognition of their personal code or fingerprints.
The pharmacist predefined a list of drugs to be configured according to the chemotherapy protocols used at NIO.
The pharmacy technician responsible for loading the ADS, consulted the server daily and defined the list and the quantities of drugs below the stock threshold defined. The ADS was loaded on average three times a week. During restocking, the pharmacy technician entered the expiry dates of drugs into STOCKART. During validation, the pharmacist followed the stock status of different drugs specialities present in the ADS and their batches. During drugs picking, the pharmacy technician selected for a given patient (according to the validated protocol), the drugs one after the other, respecting the trade name and the quantity validated. In addition to the expiration date (close or far), he was informed of the specific terms of use of the selected product by messages configured by the pharmacist such as the dilution solvent, the storage conditions after dilution. Upon request, the drawers and shelves opened one after the other, with light-emitting diodes indicating the location of drugs to be withdrawn.
Choice of the method used
Our analysis was conducted by the FMEA method. FMEA is applied to the analysis and evaluation of the criticality of all the potential failures of a product caused by the processes it underwent. 17 FMEA is an inductive quality tool. Its objective is to identify steps where additional preventive measures may be appropriate to minimize the risks. 18 The FMEA method is described by the ISO 31000, 2009 standards and is one of the tools adapted by the Institute of Healthcare Improvement to help hospitals improve patient safety by optimizing their own organization. 16 This method was chosen due to its practicality and its relative ease of implementation in addition to allowing risk quantification.
Failure modes, effects and criticality analysis
To carry out this analysis, a multidisciplinary team of six persons w was formed. This team was constituted of: a professor of pharmacotechny, a hospital pharmacist (head of chemotherapy production process and quality control), an oncology clinical pharmacist, pharmacy resident, a pharmacy technician, and a nurse.
Four work sessions of approximately 90 min were carried out with the aim to:
Describe the steps of the chemotherapy production process. Identify through brainstorming possible failure modes during these steps that could harm the patient by asking the question “what could possibly go wrong with this step’’? It was not necessary for a participant to have witnessed the occurrence of a failure mode to include it. Consensually rate the likelihood of occurrence (from 1 to 10), the severity of the potential effect on patient (from 1 to 10) and the likelihood to detect the failure (from 1 to 10). The evaluations were carried out on the basis of explicit criteria published by Boulé et al.
19
The frequency is an estimate of the number of cases per unit of time. We determined potential causes and consequences of the failure modes, which allowed us to rate the severity and the detection scores. To rate the severity, we took into account the possible consequences for the patient and/or the impact on the process. For detectability, we estimate the probability of failure detection by control measures. To be considered detected, the failure mode must be perceived before it has an impact on patient. We took into account the chance of detection in the others steps of the process. Calculate the criticality index (from 1 to 1000): The CI of each failure mode was calculated by multiplying the frequency, the severity and the detection scores. Suggest improvement measures: Identify and make recommendations on steps where additional preventive measures may be appropriate to minimize the risks.
Results
Description of the chemotherapy production process
Chemotherapy production in our CCPU takes place in several steps: Storage of raw materials; pharmaceutical validation; labelling; raw materials picking; compounding and final control. Our comparative risk analysis focused on these steps.
Failure modes definition
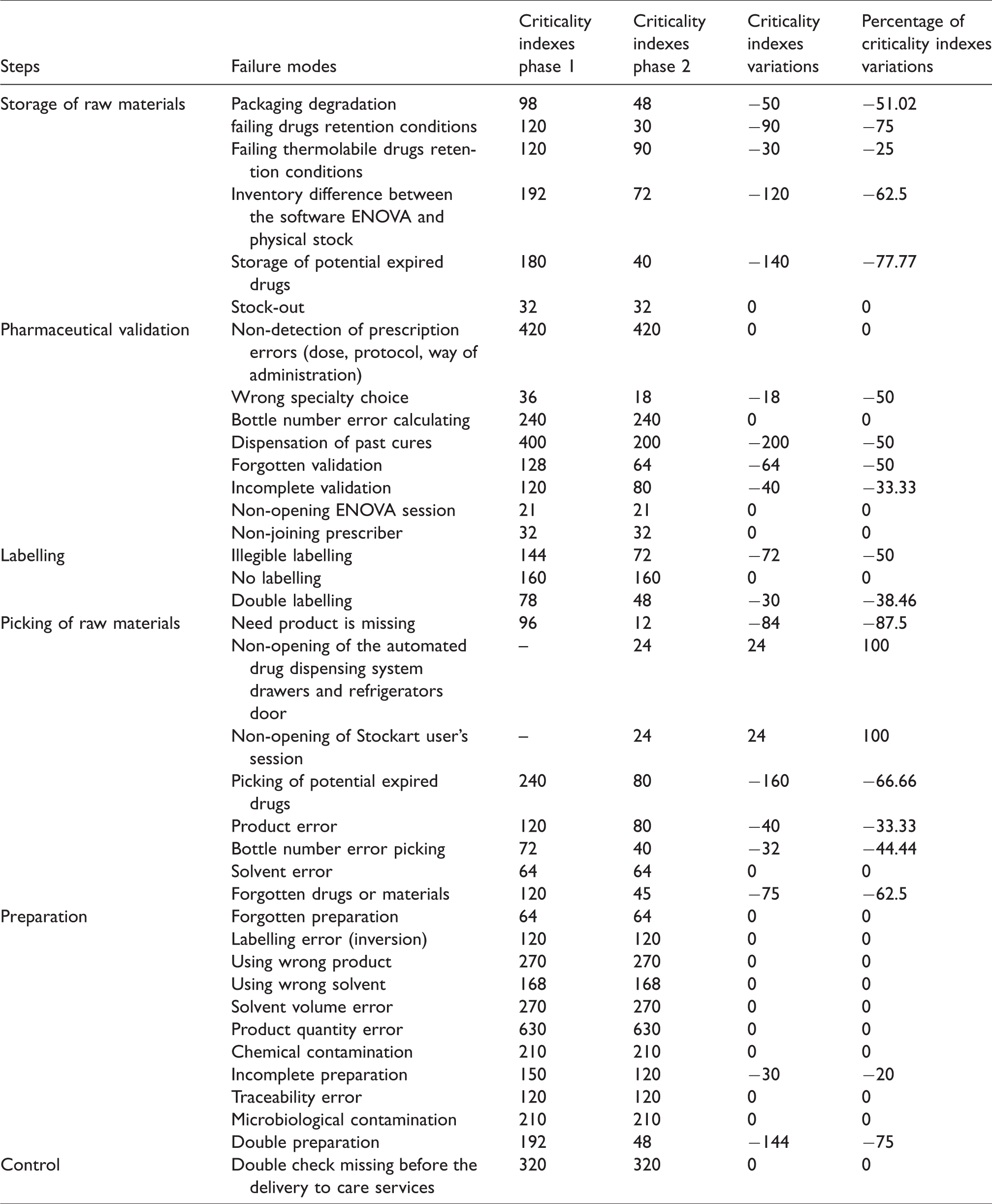
In phase 1, the work team identified 35 failure modes in the six steps of the production process – including 6 failure modes at the raw materials storage step; 8 failure modes at the pharmaceutical validation step, 3 failure modes at the labelling step; 6 at the raw material picking step;11 and 1 failure modes respectively at the compounding and final control steps. In phase 2, we identified in addition to failure modes of phase 1, two failure modes specific to the use of ADS. These failure modes were the non-opening of the user’s session and the non-opening of the ADS drawers and the ADS refrigerator door (Table 1).
Failure modes, their criticality indexes in phases 1 and 2 and their criticality indexes variations from phase 1 to phase 2.
Criticality indexes analysis
In phase 1, the sum of CIs for the 35 failure modes was 5957. The average CI was 170. In phase 2, we found a sum of CIs = 4586 for the 37 failure modes, with an average CI = 124, corresponding to a sum of CIs reduction of −1371 (−23%) from phase 1 to 2.
In phase 1 as in phase 2, the major critical steps in chemotherapy production process were the compounding step (CI = 2404 in phase 1 and 2230 in phase 2) and the pharmaceutical validation step (CI = 1397 in phase 1 and 1075 in phase 2). The sum of CIs at the storage of raw materials step was 742 in phase 1 and 312 in phase 2. At the picking raw materials step, it was 712 and 369, respectively, in phases 1 and 2. At the labelling step, the sum of CIs was 382 in phase 1 and 280 in phase 2. At the final control step, CI still remains 320 in phase 2 as in phase 1. The CI variation from phase 1 to phase 2 were −430 (−58%) for the storage of raw materials step, −322 (−23%) for pharmaceutical validation step; −102 (−27%) for the labelling step; −343 (−48%) and −174 (−7%), respectively, for the raw material picking and compounding steps. At the final control, there was no CI variation (Figure 2).
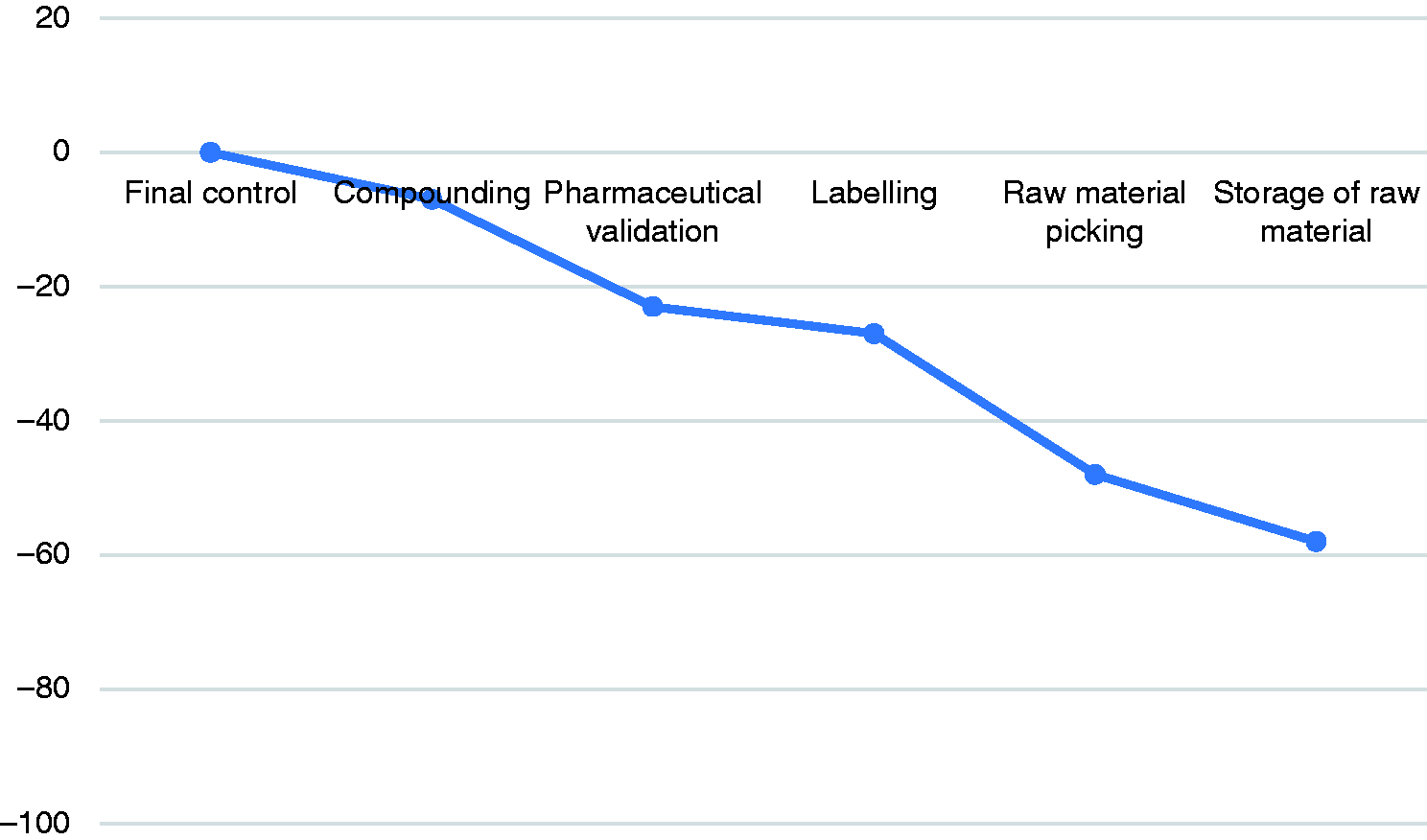
Percentage of criticality indexes variation at the chemotherapy production steps from phase 1 to phase 2.
From phase 1 to phase 2, 18 failure modes saw their CI decrease, whereas the risk remained unchanged for 17 and 2 failure modes specific to the use of ADS appeared. The most remarkable CIs reductions concerned: the needed product is missing −84 (−87%); storage of potential expired drugs −140 (−77%); and the double compounding −144 (−75%). The details of CIs variation of the failure modes are shown in Table 1.
Discussion
Our study showed a total CI reduction to −23% by using an ADS in the chemotherapy production process. Eighteen failure modes saw their CI decrease and two failure modes specific to the use of ADS appeared. The highest steps of CI reduction concerned the storage of raw materials step (−58%) and raw material picking (−48%) step. These results showed that the ADS has an important impact in the risk minimization of chemotherapy production process.
Our analysis demonstrated that the use of ADS improves the management of the stock of drugs reserved to chemotherapy production by the interface with ENOVA software. It reduced the stock-outs during the picking (−87%) and reduced the inventory difference between ENOVA and the physical stock (−62%). According to Kheniene et al., 20 the use of ADS can reduce the stock-outs and reduced the stock value of drugs by 56% in an intensive care unit. Chapuis et al. 3 showed that the storage errors were drastically decreased by ADS (−96%) in an intensive care. The ADS allowed the reduction of criticality of incomplete validations (−33%), dispensing of past treatments (−50%) and double labelling (−75%). Indeed, the ADS is equipped with a barcode reader that allows the pharmacy technician to scan the patient ID during drugs picking. The patient's treatments validated are preselected allowing additional control.
Our results suggest that ADS reduced considerably the confusion risk between the drugs which have similar packaging (−33%); the risk of bottle number errors (−44%); forgotten drugs or materials (−62%). These results lead to the same conclusion as a study in Wales which showed that the ADS improves efficiency (+43%) and the rate of avoidable dispensations errors. 21 Cousein et al. 22 suggested a 53% reduction in the risk of ME during the picking before drugs administration. In such a process, we cannot avoid all errors; nevertheless, it is clear that the risk of making wrong chemotherapy compounding was markedly reduced.
Some failure modes still had high CI in phase 2 and two news failure modes appeared. The CI of the double check missing before the delivery to care services remains unchanged. Moreover, the visual double checking has limits. According to Carrez et al., 23 it did not improve the accuracy of final production. It is difficult for an operator to accurately distinguish low volume and doses variations. Improving the final control could certainly improve the detectability of certain failure modes in our CCPU. Different methods of chemotherapy production control are available. Gravimetric control allows the detection of large compounding errors such as forgetting or doubling doses. 24 Bonnabry et al. 8 showed that the gravimetric control assisted by computer (CATO® software) allowed CI reduction to −13%. The method of video analysis (Drugcam®) allows to control 100% of the production without additional need for staff or premises. 25 However, this latter method is expensive for developing countries. Improving the safety of the compounding step requires other important approaches such as a training program for chemotherapy manipulators (pharmacy technicians) to respect good manufacturing practices. 26 Concerning the failure modes specific to ADS using, their frequency could be further reduced by repeating user training and improving ADS maintenance.
We should note that in such a process, errors cannot completely be eliminated. Continuous risk assessment is required to improve the safety of the process. A study carried out in the Netherlands 27 showed that 0.4% of dispensing errors remain in pharmacies equipped with an ADS.
The major limitation of our study is human intervention in the FMEA method, generating a degree of subjectivity in the rating of each risk. To reduce this subjectivity, our team was large and multidisciplinary. In addition, we used an explicit scoring grid as recommended by Boulé et al. 19 Another limitation of our study is that it did not include an economic assessment. The cost of the ADS and its interfacing has been evaluated at USD 61.700. Considering its impact on reducing drug expiration and optimizing stock management on the one hand, and the high prices of anti-cancer drugs on the other hand, we estimate the return of investment after two years of use.
Conclusion
This study allowed to highlight the impact of ADS on securing the chemotherapy production process. With the FMEA method used, the analysis of the six steps suggested a reduction in criticality of −23%. Like the centralization and computerization, of chemotherapy production process, the implementation of ADS should be a part of the quality assurance policy in CCPU. FMEA is one of the traditional methods of risk analysis applied in the health field. It has the advantage of being able to be implemented throughout the life cycle of a system. It would be interesting to do it again after the implementation of corrective measures.
Footnotes
Acknowledgments
We would like to thank the work team and all the pharmacy staff at the National Institute of Oncology for their collaboration
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.