
Abstract
Purpose
Proteinuria monitoring is required for patients receiving bevacizumab. Nonetheless, the frequency of monitoring is not specified in the package insert. A 2014 quality improvement study performed at Yale New Haven Health System (YNHHS) found that proteinuria occurred in 15% (all grade) of the 162 patients evaluated. These results led to decreasing the frequency of proteinuria monitoring from every treatment to every other treatment. The objective of this study is to assess the safety of the extended interval for urine protein (UP) monitoring.
Methods
Patients receiving at least four bevacizumab treatments at YNHHS from January to June 2017 were randomly selected and retrospectively reviewed. The following data were collected: baseline patient characteristics, comorbidities, medication history, and proteinuria monitoring. The grade, prevalence and management of proteinuria were evaluated. The minimum necessary sample size was determined to be 384 treatments to achieve a 95% confidence interval.
Results
Fifty-five patients and 388 bevacizumab treatments were evaluated. Urine protein was assessed in 52.5% of treatments. The incidence of proteinuria among patients was 7.2% (grade 2) and 0% (grade 3). Cumulative dose and the number of total bevacizumab doses did not affect the timing for onset or severity of proteinuria. Two patients with UP ≥ 2+ were further monitored using a 24-h urine collection test with negative results. No treatments were held due to proteinuria.
Conclusion
Monitoring proteinuria every other treatment does not increase the frequency of adverse events. Urine protein is now monitored prior to every third bevacizumab treatment, reducing unnecessary labs and chair time.
Keywords
Introduction
Bevacizumab is a humanized monoclonal antibody vascular endothelial growth factor (VEGF) inhibitor, which inhibits angiogenesis. 1 This results in the regression of existing tumor vasculature and inhibition in formation of new vasculature. Bevacizumab plus chemotherapy is approved for a number of different solid tumor malignancies such as colorectal cancer, non-small cell lung cancer, renal cell cancer, gynecologic malignancies, and glioblastoma. 2
Proteinuria is a dose-related class side effect associated with VEGF inhibitors, which can infrequently lead to nephrotic syndrome. Inhibition of VEGF affects vascularization in the glomerulus and kidney. These agents compromise the integrity of the kidney’s repair of glomerular vessels through the anti-VEGF mechanism. This causes increased permeability of the glomerulus, allowing for the escape of high-molecular weight proteins into the urine. 3
An assessment of the overall risk for severe proteinuria with bevacizumab showed that patients who received bevacizumab combined with chemotherapy in comparison to chemotherapy alone had an increased risk of high-grade (grade 3–4) proteinuria. The relative risk of high-grade proteinuria in patients receiving bevacizumab plus chemotherapy was calculated to be 4.79 versus chemotherapy alone. 4 This correlation with the addition of bevacizumab to chemotherapy suggests that the monitoring of proteinuria is critical.
Proteinuria management is critical in delaying disease progression in patients. The reduction of proteinuria by > 30% of baseline within the first 6 to 12 months of treatment has shown to predict long-term renal and cardiovascular outcomes. 3 All patients should be monitored prior to the start of bevacizumab for existing kidney disease, checking for proteinuria and estimated kidney function. 3
Based on the package insert and clinical trials, the incidence of proteinuria was reported 5–20% (all grade) and 0.7–7% (grade 3–4).2,5 Nephrotic syndrome occurs in <1% of patients in trials. 2 The manufacturer recommends routine proteinuria monitoring by dipstick and a 24-h urine collection follow-up if urine dipstick results are > 2+. However, the frequency of proteinuria monitoring is not specified during bevacizumab therapy. Additional recommendations include to hold dose of bevacizumab if > 2 g of proteinuria/24 h, resume dose when < 2 g proteinuria/24 h and discontinue bevacizumab if nephrotic syndrome occurs. 2
A prior quality improvement study at the Smilow Cancer Care Centers of Yale New Haven Health System (YNHHS) evaluated bevacizumab monitoring. Proteinuria was found to be 15% among 162 patients (all grade). These results led to decreasing the frequency of proteinuria monitoring from every treatment to every other treatment. Implementing an extended interval for urine protein (UP) monitoring saves unnecessary tests and waiting times for patients.
The purpose of this study was to assess the safety of the extended interval for UP monitoring for bevacizumab treatment.
Materials and methods
Study design
This study was a retrospective chart review of all adult patients over 18 years old receiving bevacizumab treatments at Smilow Cancer Hospital Care Centers of YNHHS from 4 January 2017 to 31 June 2017. Patients were randomly selected, and those who received at least four bevacizumab treatments were included.
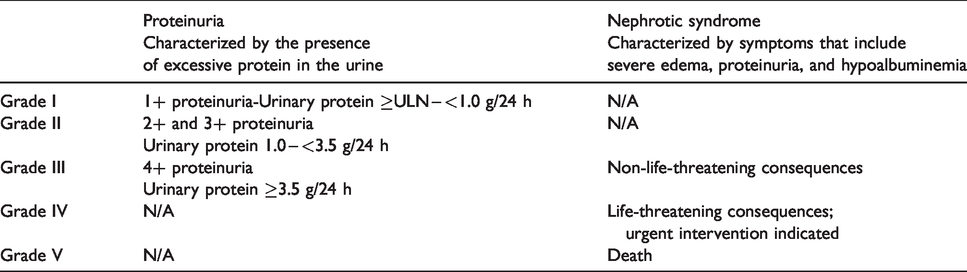
Medical records of patients who received bevacizumab during this time were reviewed. The following patient data were collected: baseline patient characteristics, comorbidities, medication history, and proteinuria. The frequency of UP dipstick and the incidence of grade 2-4 proteinuria were collected. The classification of proteinuria according to the Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0 (shown on Table 1) was used for proteinuria grading. 6
Classification of proteinuria and nephrotic syndrome according to Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. 6
Study end points
The primary outcome of this study was to evaluate the incidence of grade 2–4 proteinuria. The secondary outcomes of this study were to evaluate the frequency of UP dipstick monitoring and the number of treatment interruptions due to proteinuria.
Data analysis
Using the standard equation for calculating minimum sample size for discrete data, a sample size of 384 treatments was required to deliver a 95% confidence level of accurate assessment.
Results
Patient characteristics
A total of 388 bevacizumab treatments among 51 patients were evaluated during the study period. The patient demographics are listed in Table 2. The median number of bevacizumab treatments each patient received was six (range 4–13). The population was primarily female (63.4%), and co-morbidities among the patients were pre-existing hypertension (38.2%), pre-existing diabetes (23.6%), and pre-existing renal dysfunction (3.6%). A number of different malignancies among the patient population were included in the study with the majority being breast, colon, rectal, glioblastoma, lung, and gynecologic malignancies.
Baseline patient characteristics.
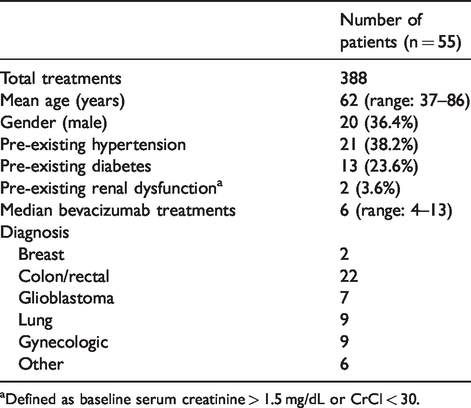
aDefined as baseline serum creatinine > 1.5 mg/dL or CrCl < 30.
Primary outcome
Overall, the incidence of grade 2 proteinuria was 7.2% and grade 3–4 proteinuria was 0% as defined by CTCAE criteria (Figure 1). There were 10 instances among four different patients whom had a (UP) ≥2+. Two of these patients performed a 24-h timed urine test based on manufacturer recommendations. The UP result of the two patients who did not perform a 24-h timed urine test was acknowledged by the provider who permitted dosing of bevacizumab and further follow-up on UP. Cumulative bevacizumab doses and total number of doses were two variables assessed for severity and onset of proteinuria. Patients with grade 2 proteinuria ranged in onset from cycle 1 to cycle 13; therefore, there was no consistent correlation.
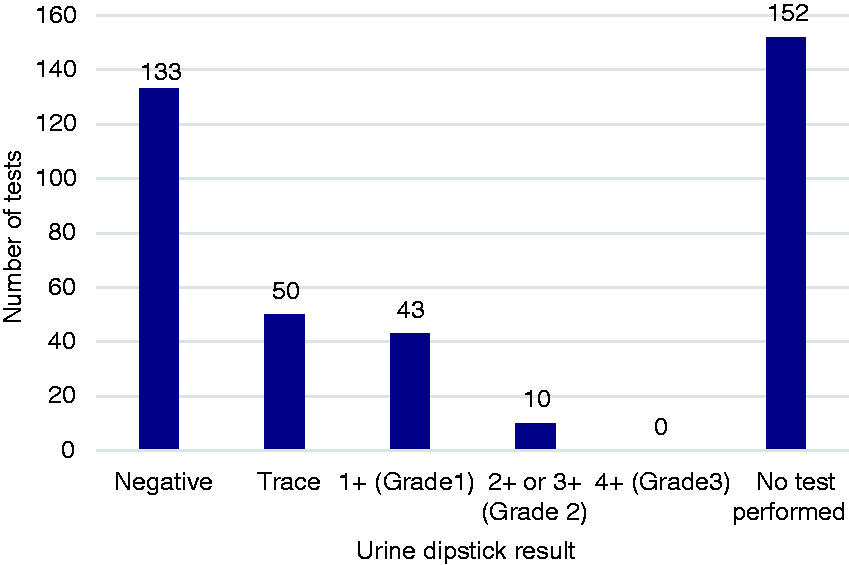
Incidence and severity of proteinuria (n = 388).
Secondary outcomes
Among the 388 treatments, 206 (52.5%) bevacizumab treatments were monitored for proteinuria every other treatment and 126 (33%) were monitored every treatment. Fifty-five (14.4%) of treatments were not monitored at all despite patients being due for urine protein. During assessment of those patients who were monitored with every bevacizumab treatment, 21.8% were for UP ≥1+.
UP ≥2+ was detected in 10 treatments, of which two treatments were further monitored using a 24-h urine collection test. Neither collection test resulted with UP ≥2 g. All patients continued with subsequent bevacizumab treatments, and no treatments were held due to proteinuria despite elevated UP without any adverse events.
Among the four patients with UP ≥2+, one of these patients had pre-existing diabetes and none of them had pre-existing renal dysfunction. There was no apparent association amongst the patients’ baseline characteristics and the incidence of proteinuria.
Discussion
In this analysis, the incidence of grade 3–4 proteinuria observed was 0% compared to 0–1.8% in a number of randomized controlled trials.7–11 The few patients that developed grade 2 proteinuria were closely monitored and underwent 24 h urine collection to rule out nephrotic syndrome.
According to the bevacizumab package insert, data from a post marketing safety study showed poor correlation between UP/creatinine ratio and 24-h UP; therefore, it seems pertinent to continue using UP dipstick as a tool for monitoring proteinuria development while on VEGF therapy. 2 Evaluating albumin excretion is thought to correct for any differences in urine dilution which makes it preferred over urine creatinine. 3
Based on this internal study, bevacizumab UP monitoring has been extended to every third dose. Across the health system, it is now recommended to monitor proteinuria before every third treatment or as ordered by provider. If result is greater than 2+ by urine dipstick or urine analysis, it is essential to notify the provider and checking proteinuria with 24-h urine collection may be considered. It is recommended to hold bevacizumab for proteinuria ≥ 2 g per 24 h and resume when less than 2 g per 24 h. It would be at the discretion of the provider to determine the risks versus benefits of extending the frequency of UP monitoring in patents with history of greater than 2+ proteinuria while on treatment.
A study performed by Lee et al. retrospectively evaluated 89 patients for the development of proteinuria while on bevacizumab therapy. Grade 3 proteinuria was only observed in two patients (2%). While our study found that proteinuria was independent of cumulative dose, this study by Lee et al. did find a trend toward increased grade of proteinuria with increasing cycles of therapy. It was concluded that monitoring the UP to creatinine ratio may not be necessary with every dose of bevacizumab due to the low prevalence of proteinuria, similar to the results of our analysis. 12
In an exploratory meta-analysis, patients from seven randomized clinical trials were evaluated for the development of proteinuria while on bevacizumab therapy. Grade 2–4 proteinuria occurred in 5% of patients and resolved in 75% of these patients. Among the group of patients that experienced proteinuria, 42% of them were resumed on bevacizumab; however, about half of them had a second episode of grade 2–4 proteinuria. 2
While we had a smaller patient population, it was observed that the incidence of proteinuria was quite rare and development of 2 g UP after a 24 h urine collection was non-existent.
In a majority of these studies, patients are on a combination of bevacizumab with other chemotherapy agents. It is unclear exactly how much the bevacizumab contributes to proteinuria compared to other nephrotoxic chemotherapy agents. Wu et al. analyzed 16 different studies to assess the incidence of grade 3 or 4 proteinuria with chemotherapy alone compared to bevacizumab in addition to chemotherapy. 3 This meta-analysis found that bevacizumab in combination with other chemotherapy agents significantly increased the risk for high-grade proteinuria (2.79%) compared to chemotherapy alone (0.4%). In addition, it is suggested that specific tumor types might put patients at higher risk for the development of high-grade proteinuria and nephrotic syndrome. This meta-analysis found that the highest incidence of proteinuria was in those with renal cell carcinoma (RCC) (11.9%) compared to those with a non-RCC malignancy (3.5%). Lastly, it is pertinent to consider nephrotoxic chemotherapy agents and their role in the development of proteinuria. A subgroup analysis was performed evaluating the occurrence of high-grade proteinuria in patients who received platinum agents; however, there was no significant difference found between platinum and non-platinum-based chemotherapy. 4 Overall, it is necessary to account for all patient variables when determining the appropriateness of extended frequency monitoring.
While we found no apparent association between patients’ baseline characteristics and co-morbidities, there has been evidence in some studies that co-morbidities such as hypertension, chronic kidney disease, and diabetes are associated with increased UP. A study conducted by Yeh et al. assessed patients with breast cancer, lung cancer, and gastrointestinal cancer. This retrospective study showed a significant association between incidence of proteinuria with hypertension, chronic kidney disease, and viral hepatitis. 13 In comparison, Lee et al. found no identifiable risk factors among this patient population that would predispose certain patients to the development of proteinuria during bevacizumab therapy. 12
Our study is not without limitations. First, the small sample size of 388 treatments and 55 patients makes it difficult to draw conclusions regarding risk factors. The nature of the study was a retrospective review using patient electronic medical records which allows room for error when collecting pre-existing patient characteristics. The retrospective nature of this study lacked randomization and could have the potential for selection bias. In addition, the low incidence of proteinuria in this patient population could be related to the six-month time frame in which patients were being evaluated for proteinuria. A longer period of assessment could have resulted in higher incidence of proteinuria, as patients received more bevacizumab doses. Lastly, there could have been other confounding reasons for patients to have elevated UP other than bevacizumab independently.
Further directions to consider are evaluating the safety and cost savings associated with this change in practice by extending proteinuria monitoring to every third bevacizumab dose. In addition, it is well established that proteinuria is a class effect; therefore, other VEGF inhibitors that require proteinuria monitoring (i.e. ramucirumab) could be evaluated for a similar approach in monitoring practices.
In comparison to our institution’s prior study, it can be concluded that the decreased frequency of monitoring proteinuria to every other treatment does not increase the frequency of proteinuria-related adverse events. Further extending UP monitoring to every third treatment has the potential to minimize laboratory costs, shorter chair time in the clinic and fewer resources.
Footnotes
Acknowledgements
The article was presented at 2018 Eastern States Conference for Pharmacy Residents and Preceptors, Hershey, Pennsylvania.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.