
Abstract
Introduction
Post-transplant lymphoproliferative disease (PTLD), a lymphoid proliferation observed after the solid organ transplantation or allogeneic stem cell transplant, is an important and mortal complication that can occur during the post-transplant period. Classical Hodgkin lymphoma-like PTLD is the least form of PTLD. We are presenting an adult case of classical Hodgkin lymphoma-like PTLD which was successfully treated with nivolumab.
Case report
A 31-year-old female was diagnosed with primary myelofibrosis and we performed allogeneic stem cell transplantation from her HLA fully matched brother in 2015. Two years after transplant, classical Hodgkin lymphoma-like PTLD was diagnosed. The patient was resistant to six cycles of ABVD chemotherapy and four cycles of brentuximab vedotin.
Management and outcome
After the failure of ABVD and brentuximab vedotin, we started nivolumab therapy at a dose of 3 mg/kg every 2 weeks. After six cycles, we achieved a PET negative complete remission. After 10 cycles of nivolumab, the patient is still followed with a complete remission. Still, there is no evidence of acute or chronic GvHD, and therefore no need for immunosuppressive treatment. No auto-immune complication was observed. It is planned to give nivolumab treatment to the patient until the progression.
Discussion
Our case has depicted that the classical Hodgkin lymphoma type PTLD may be resistant to the conventional treatments and anti-CD30 brentuximab vedotine. In such cases, nivolumab may be an effective and worth assessing agent in terms of both activity and safety profile.
Keywords
Introduction
Post-transplant lymphoproliferative disease (PTLD), a lymphoid proliferation observed after the solid organ transplantation or allogeneic stem cell transplant, is an important and mortal complication that can occur during the post-transplant period. Although it is generally seen in association with the deteriorated immune system functions and EBV reactivations related to the immune-suppression, EBV negative cases can also be observed. 1 It was first defined in 1968 in a patient with a renal transplant, and since 1984 it has been named as PTLD. 2
According to the WHO 2016 lymphoid neoplasm classification, PTLD is observed in six subcategories: Plasmatic hyperplasia PTLD, Infectious mononucleosis PTLD, Florid follicular hyperplasia PTLD, Polymorphic PTLD, Monomorphic PTLD (B- and T-/NK-cell types), and classical Hodgkin lymphoma PTLD. Classical Hodgkin lymphoma type PTLD is the least common form of PTLD. 3 However, due to the low number of the reported cases, clinical and physiopathological characteristics of classical Hodgkin lymphoma type PTLD could not be clearly identified.
After the solid organ transplants, the rate of PTLD cases can be up to 20% in especially multi-organ transplants, depending on the transplanted organ and the immune suppressive regimen whereas the rate is 2% after the allogeneic stem cell transplant. 4 In the largest series where 26,901 allogeneic stem cell transplant cases are examined, PTLD developed in 127 cases with a rate of 0.47%. In 105 of these 127 cases (83%) PTLD was diagnosed within the first year of the post-transplant period. The incidence rate of PTLD post allogeneic stem cell transplant is higher in such cases as unrelated or mismatched donors, those with T stem depletion, patients who had an ATG in the conditioning regimen, cases of a chronic Graft versus Host Disease (GvHD) that require a longer immune suppression, cases in ages >50 and multiple transplants. 5 Also, the risk is great in transplants from the EBV positive donors to the EBV negative recipients. 3
Nivolumab, which is an immune check inhibitor, blocks PD-1 (programmed cell death-1) selectively and is used in the treatment of numerous malign cases including lymphomas. It is approved by FDA for the treatment of the resistant Hodgkin lymphoma post autologous stem cell transplantation and brentuximab vedotin (BV). Its most common adverse effect is the auto-immune complications, such as pneumonitis, thyroiditis and hepatitis. Besides, there is sufficient evidence that its use before and after the allogeneic transplant, increases the graft versus host disease and the mortality related to the transplant. 6
Our case report aims to present a case of classical Hodgkin lymphoma type PTLD that occurred 2 years after transplant and treated with nivolumab which is resistant to the conventional treatment and BV in a patient who had an allogeneic stem cell transplant due to the primary myelofibrosis.
The case
A 31-year-old female patient was diagnosed with primary myelofibrosis in 2015 and her DIPSS score was 3 and her risk group was identified as intermediate-2. A mutation of 12.5% was found in JAK-2 617F. During the diagnosis, the spleen was 10 cm palpable below the costal margin. Hb: 8.5 g/dl, peripheral blast percentage was 1% and the bone marrow biopsy revealed diffuse fibrosis (3/3). In October 2015, we performed an allogeneic stem cell transplant, from an HLA fully matched brother. The patient received a conditioning regimen including fludarabine (180 mg/m2) + busulfan (0.8 mg/kg every 6 h for 3 days) + ATG (5 mg/kg every 12 h for 1 day). Graft versus host disease (GvHD) prophylaxis consisted of methotrexate and cyclosporine. The neutrophil engraftment occurred on day 19 and the platelet engraftment occurred on day 21. In both the donor and recipient, EBV VCA IgG was detected positive before the transplant, whereas EBV DNA PCR and VCA IgM were negative. On day 100, post-transplant, a full hematologic recovery was observed in the patient. JAK-2 mutation was negative. No palpable spleen below the costal margin and bone marrow biopsy revealed a minimal fibrosis (grade 1/3). A complete donor type chimerism was observed, and cyclosporine was withdrawn on the 180th day of transplant and the follow-up period was started.
In November 2017, 2 years after transplant, enlarged cervical and axillary lymph nodes were seen in the physical examination. The multiple cervical hypoechoic lymph nodes without an echogenic hilum were observed at level 5 in the ultrasonographic examination. The largest pathological lymph node was measured as 3.6 cm × 2.1 cm. The excisional cervical lymph node biopsy was performed and the pathology result was classical Hodgkin lymphoma type PTLD. The tumor cell was positive for CD15 and CD30, PAX-5 was negative for CD3 and CD45, CD20 was minimally expressed. EBV-EBER and EBV-LMP were negative. PET-CT was positive both for supra-diagrammatic and infra-diagrammatic disease, and no bone marrow involvement was found for Hodgkin, but minimally fibrosis (grade 1/3) was still available. JAK-2 was negative and the complete donor type chimerism was still available.
EBV VCA IgM was negative, EBV VCA IgG was positive and EBV PCR was negative. Stage IIIA classical Hodgkin lymphoma type PTLD was diagnosed, and ABVD (adriamycin, bleomycin, vinblastine, dacarbazine) therapy was started. After cycle 2, the interim PET CT scan showed Deauville score 3, and after the completion of six cycles of ABVD PET revealed a Deauville score 4. Re-biopsy was performed, and again the re-biopsy was positive for the classical Hodgkin lymphoma type PTLD and the same immunohistochemistry was observed. While the patient was receiving ABVD, prolonged neutropenia and thrombocytopenia were observed. (Total Naranjo Score: 9, definite adverse drug reaction, is summarized in Table 1) Due to the positivity of CD30, BV was started with a dose of 1.8 mg/kg in the patient who was resistant to conventional chemotherapy. After four cycles of BV, PET CT revealed a Deauville score of 5 with a progressive disease. So we started nivolumab therapy at a dose of 3 mg/kg once every 2 weeks. After six cycles of nivolumab, PET CT scan was negative and we achieved complete remission, continued to treat the patient with nivolumab. After 10 cycles of nivolumab, the patient is still followed with a complete remission. Still, there is no evidence of acute or chronic GvHD, and no need for immunosuppressive treatment. No auto-immune complication was observed and the complete donor type chimerism is still available. It is planned to give nivolumab treatment to the patient until the progression.
Naranjo algorithm of adverse drug reaction (prolonged neutropenia) with ABVD chemotherapy.
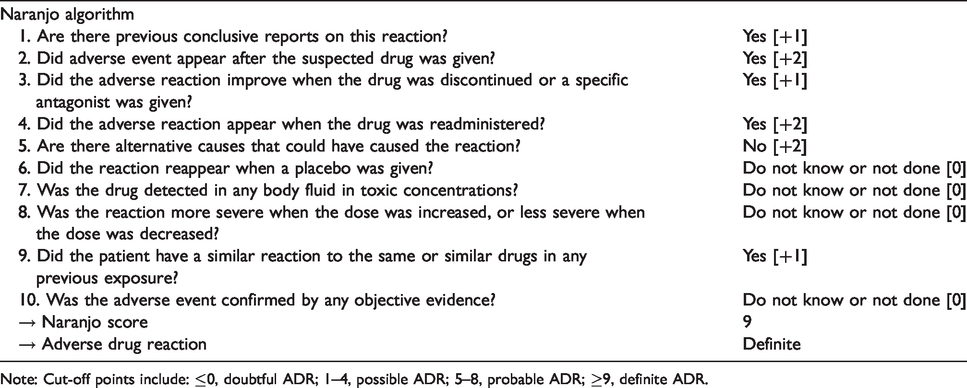
Note: Cut-off points include: ≤0, doubtful ADR; 1–4, possible ADR; 5–8, probable ADR; ≥9, definite ADR.
Discussion
PTLD after HSCT was frequently found to be <%2, but ranging from 1.16% to 8% in different settings and risk factors. 5 Classical Hodgkin lymphoma type PTLD is the least common form among PTLD subtypes. 7 It is generally reported post solid organ transplants during the childhood. There are also very rare cases reported in adulthood and post allogeneic stem cell transplant. Post-HSCT PTLDs are generally related to EBV positivity, yet EBV negative cases have also been reported.
According to WHO 2016 update, the criteria in the classical Hodgkin lymphoma panels were suggested for the diagnosis of the classical Hodgkin lymphoma type PTLD. In addition to CD15 and CD30 positivity, C20 positivity can also be seen in variable rates. In our case, a weak CD20 positivity was observed as well as CD15 and CD30 positivity. EBV-EBER and EBV LMP were detected as negative for EBV. In our case, the risk factor is defined as the use of ATG for the T cell depletion. PTLD in our case was diagnosed 2 years after transplant and 18 months after immunosuppressive therapy discontinuation, whereas 83% of the PTLD cases post HSCT are reported to develop within the first year.
In 17 cases of adult Classic Hodgkin lymphoma type PTLD in literature, only 3 were reported to develop post stem cell transplant: 1 case post autologous stem cell transplant due to the astrocytoma in the first 3 months, 8 1 case post umbilical cord allogeneic transplant due to the lymphoblastic lymphoma after 15 months 9 and the last case post unrelated allogeneic stem cell transplant due to the Chronic Lymphocytic Leukemia after 9 months. 10 In all three cases, CD15 and CD30 were found positive in the pathological examinations of the cases. Two cases were EBV positive while one case was EBV negative. Also, CD20 was negative in two cases while CD20 positivity was observed in one case. When the cases post solid organ transplant were examined, CD15 positivity with 82% (14/17), CD30 positivity with 100% (17/17) and the EBV positivity with 88% (15/17) were observed. 11
When the treatment of these cases is examined, 8 of 17 cases managed only with the cessation of immunosuppression. In others, in addition to the withdrawal of immunosuppression, if taken, a conventional chemotherapy ± rituximab has been started. The most widely used conventional chemotherapy scheme is ABVD. In most cases, a complete response was achieved. In literature, there is no reported relapse refractory Hodgkin type PTLD post allogeneic stem cell transplant.
In literature, the use of nivolumab for the PTLD post-HSCT was reported in one case. In this case of an 11-year-old girl with a diagnosis of chronic myeloid leukemia, resistant to tyrosine kinase inhibitors, the case had a haploidentical second transplant due to the lack of graft post allogeneic transplant from the 5/6 conformed umbilical cord. Diffuse large B cell lymphoma type PTLD with the CNS involvement developed in the third month after the second transplant. Nivolumab was started due to the resistance to cytarabine and high dose MTX, which was started with a low dose when the immune complications are taken into consideration (1.1 mg/kg), yet no response was achieved with a low dose. And an increased dose of 2.2 mg/kg was given 17 courses; a complete response was achieved with a negative PET-CT scan. In this case, no GvHD or auto-immune complications were observed during the period of treated with nivolumab. 12
Conclusion
Our case has depicted that the classical Hodgkin lymphoma type PTLD can also be seen in time periods other than the first year post allogeneic transplant in EBV negative cases without immunosuppressive treatment. Besides, it may be resistant to conventional treatments and anti-CD30 BV. In such cases, nivolumab may be an effective and worth assessing agent in terms of both activity and safety profile.
Our case has contributed to the literature as the first reported case of a relapsed refractory adult classical Hodgkin lymphoma type PTLD after allogeneic stem cell transplant with an excellent response to nivolumab.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.