
Abstract
Introduction
Pharmacokinetic interaction of high-dose methotrexate (MTX) and other concomitantly administered renally secreted medicinal products may lead to insufficient methotrexate serum level decrease and significant MTX toxicity.
Case report
We report the case of an 18-year-old male patient treated with high-dose MTX for an osteosarcoma and with high-dose piperacillin-tazobactam at the same time. MTX serum levels were severely elevated 24 hours after the MTX infusion and did not decrease in accordance with the specific calcium folinate rescue protocol. The patient experienced renal failure accompanied by neurological symptoms, most consistent with MTX-related renal and CNS toxicity.
Discussion
Severe MTX-related toxicity, caused by drug-drug interaction, suggests that the concomitant use of high-dose MTX and high-dose piperacillin-tazobactam should be avoided generally.
Keywords
Introduction
Methotrexate (MTX) is an antineoplastic agent used at high doses for the treatment of lymphatic neoplasms and sarcomas. High-dose methotrexate (HD-MTX) treatment is associated with a risk for adverse drug reactions (ADR), such as aplastic anemia, renal impairment, hepatitis, and myelosuppression. MTX serum levels are therefore closely monitored and so-called calcium folinate (CF, leucovorin) rescue therapy is utilized to prevent the side-effects. In sarcoma treatment protocols, in which HD-MTX is administered over a period of four hours and CF is given in a dose of 15 mg/m2 every 6 hours, starting at 24 hours. Rescue therapy is continued until the MTX concentration is less than 0.1 µM. Pharmacokinetic monitoring of MTX at close intervals is important in order to avoid severe ADRs. Immediate protocol-guided adjustment of CF doses is initiated if elevated MTX concentrations occur.1–3
MTX is mainly eliminated renally, both by glomerular filtration and active tubular secretion. In order to enhance the water solubility of MTX (weak acid molecule), hyper-hydration and urine alkalinisation are used. Low pH values increase the risk of precipitation of the non-ionized MTX form in the renal tubules and renal damage. Concomitant use of non-steroidal anti-inflammatory drugs (NSAID), penicillin-derivatives, sulfonamides, ciprofloxacin or proton pump inhibitors can lead to elevated MTX serum levels due to the inhibition of tubular MTX secretion by the organic anion secretory system of the proximal renal tubule. Prolonged elevated MTX serum concentration may result in an increased risk of MTX toxicities, mainly renal, central nervous, dermatologic, gastrointestinal, hematologic, hepatic, and pulmonary toxicity. 1 Frequency and severity of MTX side effects vary by route and dosage. Most of the toxic effects occur dose related and are reversible if detected early and if CF rescue is adjusted accordingly. 1 Inadequate decrease of MTX serum levels in patients treated simultaneously with MTX and penicillin-derivatives has been described in few case reports,4–8 one describing a fatal outcome. 9
Case presentation
This article describes the case of an 18-year-old male patient suffering from osteosarcoma. He was treated according to the EURAMOS-1 protocol V4.02. Two neoadjuvant and four adjuvant cycles of MAP (MTX/Doxorubicin/Cisplatin) with high-dose MTX (12,000 mg/m2 BSA (body surface area)) courses in week 4 and 5 of each cycle were scheduled (in total 12 infusions over 4 hours). After the first MTX course in week 4, MTX serum levels decreased regularly but the patient developed unexplained severe paresthesia in both legs and paraparesis, most likely consistent with MTX-induced myelopathy. CF rescue therapy was intensified to 300 mg/m2 BSA CF every 6 hours for three days and all neurologic deficits disappeared quickly. The second HD-MTX course in week 5 was omitted due to the previous neurological complications. During the third HD-MTX course, the 24 hours post-infusion serum level (see Table 1) exceeded the expected level, and adjusted CF rescue therapy (300 mg every 6 hours) was administered over a four-day period. The patient suffered again from paresthesia in both lower extremities. The fourth MTX course of the second neoadjuvant cycle was therefore scheduled with the adjusted, intensive CF rescue scheme for three days. Neurological symptoms were not observed. The patient underwent successful complete surgical resection of his osteosarcoma (R0) after this cycle.
Overview of the patient’s MTX serum levels 24 hours post-infusion, adjustment of CF rescue therapy, type and grade of adverse events.
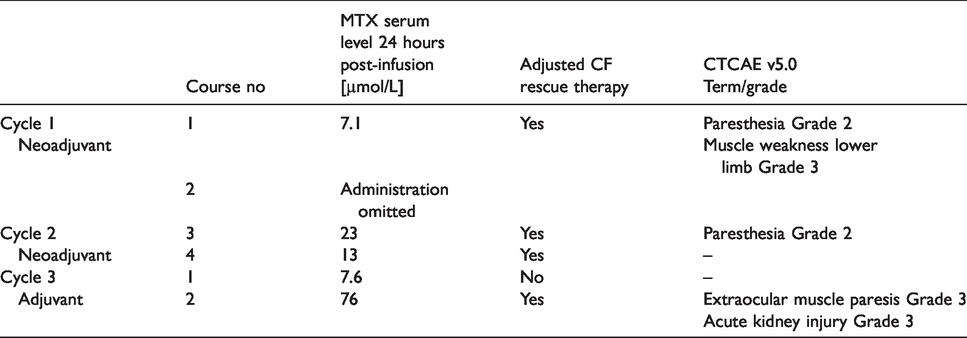
Four weeks after surgery, the first adjuvant MTX course was administered, and no elevated MTX levels or neurotoxicity were noted (compare Table 1). Serum creatinine remained within normal limits. However, during the second adjuvant MTX course, the 24 hours post-infusion MTX level amounted to 76 µmol/L, thereby exceeding the regular level according to the CF rescue protocol more than ten times. The patient complained of double vision, most likely consistent with MTX-associated neurotoxicity. In addition, the patient developed non-oliguric renal failure and serum creatinine increased. Intensified CF rescue therapy (300 mg/m2 BSA every 6 hours for two days) augmented by hyper-hydration (3 L/d) were started. MTX serum levels and serum creatinine declined during the following five days (compare Figure 1). The neurological symptoms diminished, and renal function recovered.
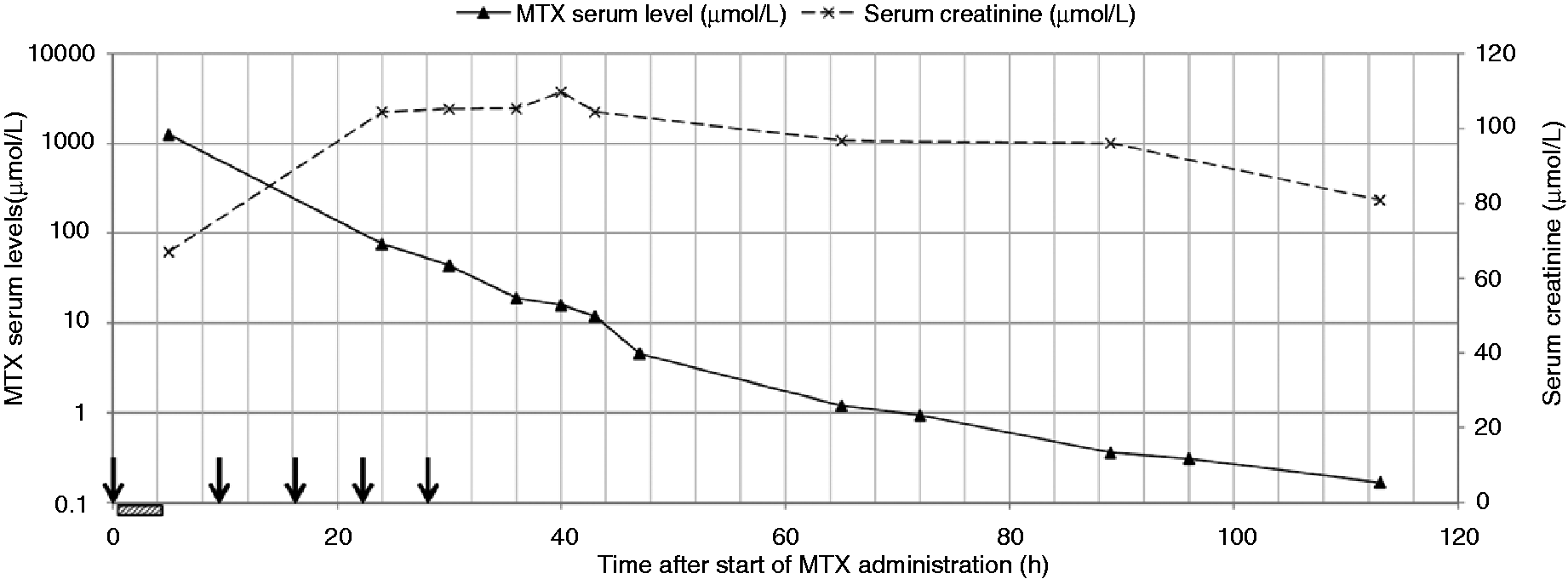
Development of MTX serum levels and serum creatinine after the second high-dose MTX course in MAP Cycle 3. Arrows: Time points of piperacillin-tazobactam administration; Hatched bar: Infusion of high-dose MTX over 4 hours; [h] = hours.
Due to a urinary tract infection and fever, the patient had received five doses piperacillin-tazobactam 4.5 g in parallel to the MTX course. The first dose of piperacillin-tazobactam was infused 30 minutes prior to the HD-MTX infusion. The fifth and last piperacillin-tazobactam 4.5 g dose was administered 28 hours after the start of HD-MTX administration (compare Figure 1). Antibiotic therapy with piperacillin-tazobactam was stopped near-term because of a suspected pharmacokinetic drug interaction, resulting in persistently elevated MTX serum levels.
The patient was discharged in stable condition six days after the MTX infusion. He received two further cycles of high-dose MTX followed by standard CF rescue therapy without showing signs of neurotoxicity or other severe toxicities.
Discussion
The 18-year-old osteosarcoma patient was treated in accordance with the EURAMOS-1 protocol. The MTX serum clearance was closely monitored as scheduled in the protocol and CF rescue doses were immediately adjusted if elevated MTX-levels occurred. According to best practice oncology, we always substitute proton pump inhibitors by H2 receptor blockers 10 and avoid the use of NSAIDs and other medication known to reduce MTX elimination. However, severe side effects related to high-dose MTX were recognized in this osteosarcoma patient. The patient experienced prolonged elevated MTX serum concentrations during two neoadjuvant courses and the second adjuvant course. In the latter course, the 24 hours post-infusion MTX concentration was elevated critically. Immediate root cause analysis by medication review revealed that the concomitant treatment with piperacillin-tazobactam likely contributed to the delayed MTX clearance and caused the symptoms of toxicity. A detailed literature research revealed a single case report describing the pharmacokinetic interaction between MTX and piperacillin-tazobactam. 8 The authors treated a lymphoma patient who was under long-term piperacillin-tazobactam therapy with high-dose MTX (3 g/m2 BSA) according to the CODOX-M protocol. In this case, the patient’s MTX serum levels failed to decrease appropriately until piperacillin-tazobactam infusion was stopped. During the next high-dose MTX cycle, piperacillin-tazobactam was discontinued and MTX serum levels decreased adequately. There was no other change in the medication of this female patient. 8 Therefore, we immediately discontinued the piperacillin-tazobactam treatment in our patient when the MTX serum levels failed to decrease appropriately.
There are a few other reports available describing a possible link between the delayed elimination of MTX and concomitant use of penicillin derivatives (amoxicillin, 6 mezlocillin, 5 oxacillin, 9 penicillin, 4 piperacillin 7 ) In addition, piperacillin was shown to reduce renal MTX clearance in rabbits. 11 There is no evidence available, that tazobactam, which is also a weak organic acid and eliminated by glomerular filtration und tubular secretion, impairs MTX elimination. 8 In the presence of piperacillin-tazobactam, the typical biexponential elimination of MTX was followed by a gamma-phase with a prolonged half-life of over 180 hours and persistent elevated MTX serum levels. 8 The total body clearance of MTX was significantly reduced by the concomitant use of piperacillin-tazobactam. 8
High-dose piperacillin-tazobactam (4.5 g every six hours) is a commonly used empirical antibiotic regimen in critically ill tumor patients (e.g. neutropenic patients with fever). 12 In the package insert of piperacillin-tazobactam is only given that the elimination of MTX may be reduced and MTX levels should be monitored. If so, the very high doses of piperacillin are associated with a significantly increased risk of reduced tubular MTX secretion. Fortunately, in our patient renal and neurological toxicity related to the elevated MTX serum levels were overcome by continued CF rescue and direct termination of the antibiotic therapy. Based on the here reported case and a comprehensive literature review, we conclude that piperacillin-tazobactam should generally not be used concomitantly in patients receiving HD-MTX treatment. Cephalosporins (ceftriaxone or ceftazidime) are reasonable alternatives as there is evidence from animal research that cephalosporins do not affect renal tubular secretion of MTX. 13 No interaction was observed between MTX and ceftazidime in a patient with delayed elimination of MTX associated with piperacillin administration. 7
High-dose MTX therapy is known to be associated with acute, subacute, and chronic neurotoxicity. The symptoms of our patient match with the subacute neurotoxicity symptoms for which the term ‘stroke-like syndrome’ is used. Most probably, neurotoxicity is a consequence of direct damage of the CNS and indirect damage by interference with folate, excitatory amino acids, and homocysteine pathways, among others. Patients usually recover spontaneously from the ‘stroke-like syndrome’ after a few days. 14
Information about the significant risk of MTX-piperacillin-interaction, clinical implications and management were added to the internal guidelines of our cancer center. In general, (haemato-)oncology patients are exposed to a high risk of drug interactions. To address this issue, we developed already some years ago a synoptic table of severe drug interactions for this patient cohort. 15 The table is used by the physicians to avoid severe interactions while prescribing and by clinical pharmacists while executing medication reconciliation. Caused by this incidence, we added the information about the risk of a severe interaction resulting from concomitant therapy of high-dose MTX and high-dose piperacillin-tazobactam to an updated version of the table. During continuing education sessions, the case is presented, and awareness raised.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.