
Abstract
Background
Although oral anticancer medications (OAM) provide opportunity for treatment at home, challenges include prescription filling, monitoring side effects, safe handling, and adherence. We assessed understanding of and adherence to OAM in vulnerable patients.
Methods
This 2018 pilot study defined vulnerable patients based on Chinese language, older age (≥65 years), and subsidized insurance. All participants had a cancer diagnosis and were taking an OAM filled through the hospital’s specialty pharmacy. Participants reported on OAM taking (days per week, times per day, special instructions) and handling (handling, storage, disposal). The specialty pharmacist classified patient-reported responses about OAM taking and handling as adequate or inadequate. OAM regimens were classified by complexity.
Results
Of 61 eligible patients, 55 participated. Mean age was 68 years (standard deviation [SD] = 12) and 53% were female. Patient subgroups were: 27% Chinese, 64% ≥65 years, and 9% subsidized insurance. Forty-nine percent were on frontline therapy and median time on OAM was 1 year (Quartile 1 = 0.4, Quartile 3 = 1.7). Adequacy of OAM taking (30%) and handling (15%) were low; 15% had adequacy in both. Adequacy of OAM taking and handling did not vary by patient subgroup or regimen complexity. Mean patient-reported adherence was high (5.4, SD = 1, possible range 1–6) and did not vary by adequacy of OAM taking or handling.
Conclusions
Understanding of OAM taking and handling in this group of vulnerable patients was low and did not align with patient-reported adherence. Future interventions should ensure that patients understand how to safely take and handle OAM, thereby optimizing their therapeutic potential.
Keywords
Introduction
Advancements in biopharmaceuticals have led to increasing availability and use of oral anticancer medications (OAM); the US Food and Drug Administration has approved nearly 90 indications for OAM between 2015 and 2019. 1 Many of these medications have improved efficacy and reduced toxicity compared to parenteral chemotherapy. However, the increased use of OAM creates challenges for patients, providers, and health care systems. Because these medications are administered at home rather than in a clinical setting, timely prescription filling, sufficient patient education, monitoring for side effects and toxicity, safe medication handling, adherence, and persistence are all of special concern.2,3 Adherence refers to correctly taking the medication (e.g., timing dosing, frequency) as prescribed, and could include under adherence (taking less than prescribed) or over adherence (taking more than prescribed), while persistence refers to taking the medication for the intended duration. 4
Prior studies of OAM adherence have found wide variability;5–7 one review reported adherence and persistence rates from 16% to 100%. 8 Low adherence and persistence can lead to worse health outcomes, such as decreased efficacy, higher recurrence and death rates, and greater healthcare costs.8–11 Factors influencing adherence have been categorized as relating to the personal characteristics of the patient, specifics of treatment, and provider/system factors. 9 Older patients with multiple comorbidities, recipients of the national health insurance program for Americans aged ≥65 years (Medicare), patients of lower socioeconomic status (SES), and patients from underserved racial and ethnic minorities are at increased risk of non-adherence.11–16 For example, older patients with multiple comorbidities may require many prescription drugs, while patients of lower SES may be unable to afford medications. Patients from underserved racial and ethnic minorities may face language and cultural obstacles, resulting in insufficient understanding of the role of the medication or its administration.
In addition, financial challenges due to cancer treatment may also be related to medical adherence. Out-of-pocket costs of OAM may be high for patients depending on their insurance coverage. Patients with the most financial distress are typically underinsured and may spend nearly one-third of their household income on care-related costs. 17 Furthermore, health insurance literacy problems are associated with both material and psychological hardship. 18 Even with insurance coverage, a third of insured patients pay more out-of-pocket costs than they expected. 17 This is associated with increased levels of financial stress and decreased medication adherence and willingness to pay for cancer care even when adjusted for financial burden. Chino and colleagues found that nearly half of cancer patients reported that they were not adhering to treatment because of costs. 17 In chronic myeloid leukemia (CML), patients with higher copayments (>$53 per month) were 70% more likely to discontinue imatinib within the first six months of starting the medication. 19
In 2014, the Tufts Medical Center (Tufts MC) Cancer Center, an academic medical center located in Boston’s Chinatown neighborhood, created a Patient Navigation (PN) Program to reduce barriers to care. Given the patient population at Tufts MC, the PN Program focused on non-English, Chinese-speaking patients, as well as patients of lower socio-economic status. In addition to linguistic barriers, some Chinese-speaking patients have cultural beliefs that result in greater misunderstanding of their cancer and treatment.20–23 Therefore, navigators were embedded within the clinical team and provided linguistically and culturally congruent support (acting as medical liaison between patient and providers, assisting with appointment coordination). By 2016, more than one third of the 996 PN visits across 158 patients involved assistance based on medication issues related to side effects, dosing, refills, and insurance, which was brought to the attention of the clinical team. Recognizing this growing need, the Tufts MC Cancer Center developed an OAM Safety Initiative, including hiring a specialty pharmacist, who worked closely with patients on all types of cancer medications. 24 This initiative was built on the 2013 American Society of Clinical Oncology/Oncology Nursing Society Chemotherapy Administration Safety Standards. 25 The specialty pharmacist had 1198 interactions across 457 patients in 2016 related to access, medication reconciliation, and patient education. 24 Although the initiative addressed many patient issues related to OAM, it was primarily provided on an ad hoc basis, so some patients continued to have unmet needs related to their OAM.
To formally assess OAM adherence in the most vulnerable patients, we conducted a cross-sectional institutional pilot study in 2018. We assessed patient-reported understanding of OAM validated against pharmacy records, patient-reported adherence, and patient-reported issues with access to OAM. Building on our findings, a longitudinal pilot intervention study to enhance understanding of and adherence to OAM was subsequently conducted. 26
Methods
Sample
Study participants were enrolled at the Tufts MC Cancer Center. The Cancer Center includes a specialty pharmacy that dispenses oncologic agents, such as OAMs, and other medications. As part of standard of care, patients starting on an OAM received information and/or teaching about their OAM on an ad hoc basis from the specialty pharmacist and/or the clinical care team. For this study, the specialty pharmacist generated a list of potentially eligible participants who were ≥18 years old, receiving their care on the outpatient adult hematology/oncology service at the Tufts MC Cancer Center, and receiving an OAM that was filled at Tufts MC. OAMs included cytotoxic therapy and all targeted agents, but excluded hormonal therapy. Patients filling their OAM at outside pharmacies were not included.
The list of potentially-eligible participants was narrowed to only include vulnerable patients, who were defined based on electronic medical record (EMR) documentation of Chinese as a spoken language, older age (≥65 years old), and/or enrollment in Medicaid insurance, which covers medical costs for Americans with limited income and resources. These patient groups represent vulnerable and underserved populations who may have difficulty accessing high-quality cancer care. 27 Patients could belong to more than one vulnerable subgroup (e.g., Chinese and ≥65 years old), but were classified based on the following hierarchy: Chinese language, older age, and then, Medicaid insurance. Research assistants conducted daily appointment screenings for patients who were identified as potentially eligible with an upcoming appointment from February 2018 to June 2018 and further assessed for eligibility based on (1) confirmation by the specialty pharmacist at the time of the appointment that the patient was still taking the OAM and (2) assessment by the clinical team that it was clinically appropriate to approach the patient. Potentially-eligible participants with no clinic visit during the study window were reclassified as ineligible.
A language-congruent research assistant (English, Cantonese, Mandarin) approached eligible participants prior to their clinic or infusion visit to introduce the study and obtain informed consent in the preferred language. A professional translation service was used to translate the consent form and all patient-reported measures into traditional and simplified written Chinese. Participants then completed questionnaires about (1) adherence to and understanding of OAM, (2) attitudes and practices around OAM, and (3) demographic characteristics. To prevent a change in responses as a result of the clinic visit, study questions not completed before the beginning of the clinic visit (with the exception of the demographic form) were not collected and were considered missing data. The study was approved by the Tufts Health Sciences Institutional Review Board (IRB).
Patient-reported measures
The adherence and understanding questionnaire contained 14 questions and was partially based on a validated instrument. 28 The study team, which included an oncologist, specialty pharmacist, patient navigator, and biostatistician—some of whom have experience in survey development—created additional questions about patient understanding of OAM instructions. These included questions about how to take the OAM(s) (i.e., daily, how many times per day, with food) and special handling instructions (i.e., wash hands, storage, disposal). A separate adherence and understanding questionnaire was completed for each OAM that the participant was taking. The attitudes and practices questionnaire was based on an existing measure about cost-related non-adherence and was completed once per participant in reference to their entire OAM regimen (i.e., not per medication). 29 The demographic questionnaire included five questions about education, employment, insurance coverage, and financial problems. All patient-reported measures were available in English as well as traditional and simplified Chinese.
EMR and pharmacy data
Additional demographic information on age, gender, and race/ethnicity were extracted from the EMR. Clinical variables extracted from the EMR included diagnosis (categorized as solid tumor or hematologic malignancy), year of diagnosis, treatment purpose (frontline or subsequent), and presence of any chronic conditions requiring medication management at the time of study enrollment. Subsequent therapy was defined as treatment given after frontline therapy due to disease or toxicity. EMR data was extracted by trained research assistants and reviewed by a medical oncologist. The specialty pharmacist abstracted the following information from the pharmacy data: time on the OAM, OAM class, OAM fill/refill dates, treatment regimens (medications, dosing, cycles), copay amounts for fill/refill closest to the date of study enrollment, and receipt of drug cost assistance. OAM classes included conventional (e.g., alkylating agents, antimetabolites, differentiating agents), immunomodulatory agents, proteasome inhibitors, tyrosine kinase inhibitors (TKIs), or multiple classes (i.e., patient taking more than one OAM from different classes). Treatment regimens were classified by complexity based on the number of drugs prescribed, scheduling considerations, route of administration, and presence of Risk Evaluation and Mitigation Strategies (REMS), which are required by the US FDA for certain medications with serious safety concerns. 30 Drug cost assistance could include being enrolled in: a drug cost assistance program facilitated by the specialty pharmacist (e.g., grant foundation support), Medicaid or subsidized insurance (low or no cost sharing for drugs), or Medicare with low/no copay (e.g., state-sponsored or subsidized Part D plans). Among participants in a drug cost assistance program facilitated by the specialty pharmacist, we were able to calculate both actual copay amount and hypothetical copay amount for two common OAMs (i.e., lenalidomide, ibrutinib) had the participant not been enrolled in the program.
One specialty pharmacist reviewed and validated patient-reported responses to the understanding questions about taking OAM(s) and special handling instructions for accuracy. Patient-reported responses on understanding of OAM taking (i.e., daily, how many times per day, with food) and OAM handling (i.e., wash hands, storage, disposal) were compared to the prescribing instructions for that OAM and classified as adequate or inadequate. Adequate responses were those describing behaviors that avoided compromising medication safety or efficacy. All of the patient responses and pharmacist classifications were reviewed by the study oncologist, who had not participated in the ordering of the OAM or in the ad hoc education.
Data analysis
Demographic and clinical characteristics of the sample were described with means, standard deviations (SD), medians, quartiles (Q1 = Quartile 1, Q3 = Quartile 3), frequencies, and percentages. For participants taking more than one OAM, the separate adherence and understanding questionnaires for each OAM were combined at the regimen level for analysis. Disease and treatment characteristics were described separately by whether the participant had adequate understanding of OAM taking and OAM handling. We described issues related to OAM access due to insurance and financial issues overall and separately by whether the participant had any drug cost assistance. Finally, we reported copay amounts for participants’ most recent refill of their OAM regimen.
Results
Sample
Sixty-seven patients met eligibility criteria, but 8 were not approached, primarily due to logistics (e.g., patient arrived too late, patient missed appointment). Of the 59 eligible participants approached about the study, 56 enrolled (94.9%) and 3 refused. One enrolled participant did not complete any patient-reported measures because their clinic visit started immediately, so the analytic sample was restricted to 55; 47 participants completed all measures. Mean age was 68.2 years (SD = 12.3) and 52.7% were female (Table 1). Patients belonged to the following vulnerable subgroups: 27.3% Chinese language, 63.6% older age, and 9.1% Medicaid insurance. More than half of participants had at least some college education (53.8%); among those with less than a high school education (n = 9), most were Chinese (n = 6).Two-thirds of participants had a hematological malignancy and the median years since diagnosis was 3.0 (Q1 = 1.5, Q3 = 4.5). The most common OAM was TKI (41.8%) and the median time taking OAM was 1.0 year (Q1 = 0.4, Q3 = 1.7). Treatment purpose was evenly split into frontline or subsequent therapy.
Patient, disease, and treatment characteristics, n = 55.
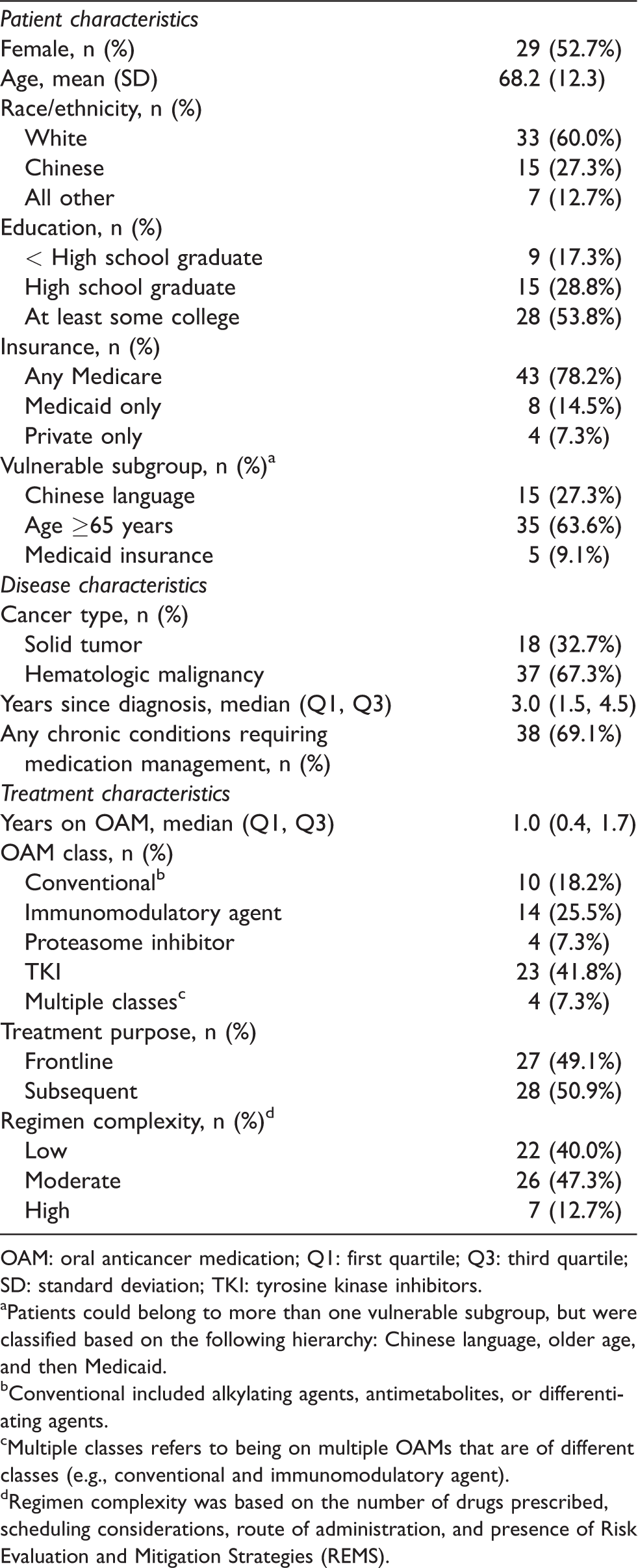
OAM: oral anticancer medication; Q1: first quartile; Q3: third quartile; SD: standard deviation; TKI: tyrosine kinase inhibitors.
aPatients could belong to more than one vulnerable subgroup, but were classified based on the following hierarchy: Chinese language, older age, and then Medicaid.
bConventional included alkylating agents, antimetabolites, or differentiating agents.
cMultiple classes refers to being on multiple OAMs that are of different classes (e.g., conventional and immunomodulatory agent).
dRegimen complexity was based on the number of drugs prescribed, scheduling considerations, route of administration, and presence of Risk Evaluation and Mitigation Strategies (REMS).
Understanding of OAM taking and handling
Of 54 participants completing questions about medication taking, 16 (29.6%) had adequate understanding of taking. With regards to medication handling, 8 out of 52 (15.4%) had adequate understanding of handling; only 8 of 52 (15.4%) had adequate understanding of both taking and handling.
When disease and treatment characteristics were described by adequacy of understanding of medication taking, no major differences were observed by vulnerable subgroup, patient-reported adherence, years since diagnosis, years on OAM, or treatment purpose (Table 2). Participants with adequate understanding of OAM taking were more likely to take multiple classes of OAM (18.8% vs 2.6%), have higher regimen complexity (18.8% vs 10.5%), and have a higher proportion with at least one chronic condition requiring medication management (87.5% vs 60.5%) compared to participants with inadequate understanding of OAM taking.
Disease and treatment characteristics by patient understanding of OAM taking and handling.
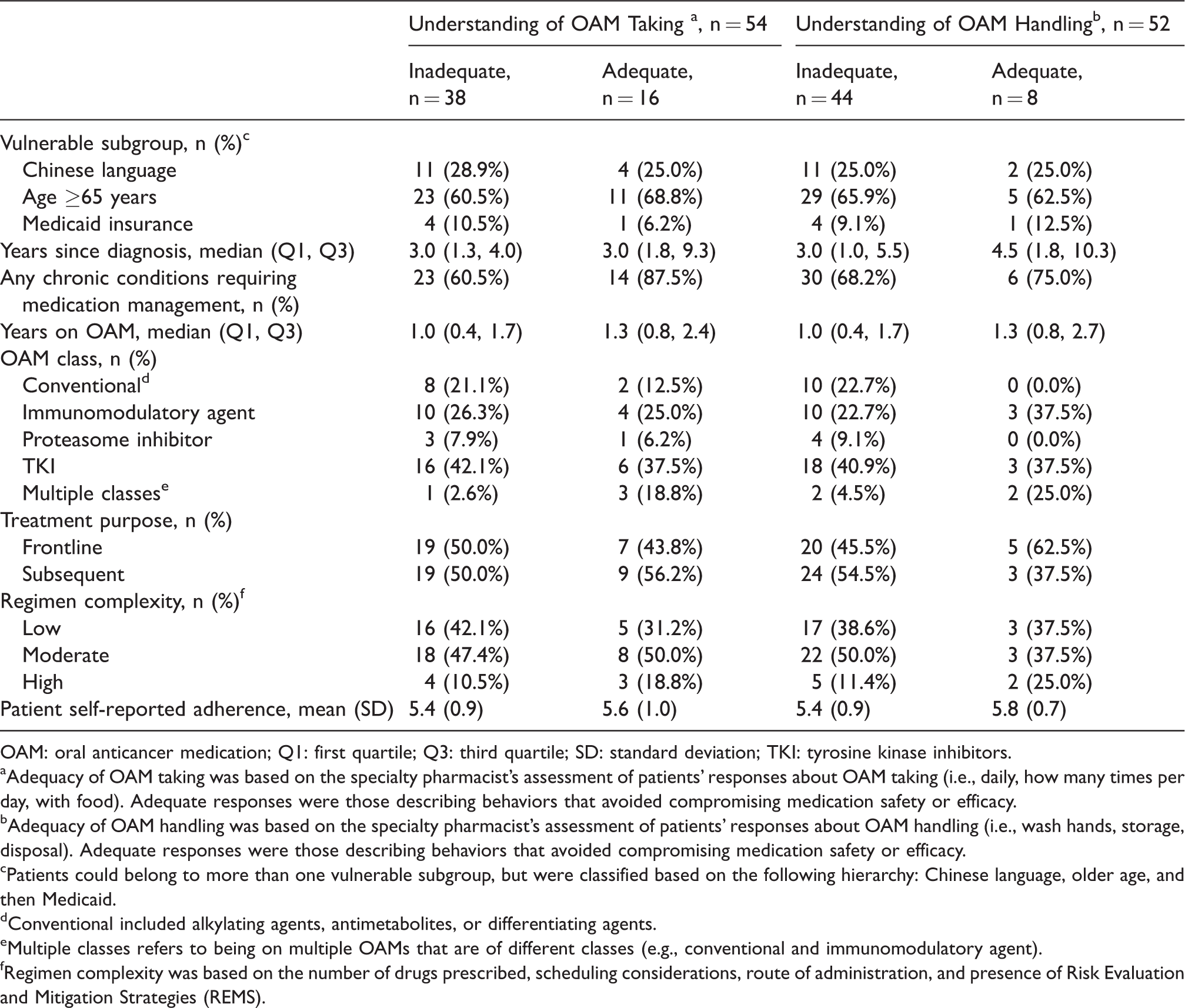
OAM: oral anticancer medication; Q1: first quartile; Q3: third quartile; SD: standard deviation; TKI: tyrosine kinase inhibitors.
aAdequacy of OAM taking was based on the specialty pharmacist's assessment of patients' responses about OAM taking (i.e., daily, how many times per day, with food). Adequate responses were those describing behaviors that avoided compromising medication safety or efficacy.
bAdequacy of OAM handling was based on the specialty pharmacist's assessment of patients' responses about OAM handling (i.e., wash hands, storage, disposal). Adequate responses were those describing behaviors that avoided compromising medication safety or efficacy.
cPatients could belong to more than one vulnerable subgroup, but were classified based on the following hierarchy: Chinese language, older age, and then Medicaid.
dConventional included alkylating agents, antimetabolites, or differentiating agents.
eMultiple classes refers to being on multiple OAMs that are of different classes (e.g., conventional and immunomodulatory agent).
fRegimen complexity was based on the number of drugs prescribed, scheduling considerations, route of administration, and presence of Risk Evaluation and Mitigation Strategies (REMS).
Similarly, no major differences were observed in adequacy of medication handling by vulnerable subgroup, patient-reported adherence, years on OAM, or having at least one chronic condition requiring medication management (Table 2). Participants with adequate understanding of OAM handling were more likely to have longer median years since diagnosis (4.5 vs 3.0), take multiple classes of OAM (25.0% vs 4.5%), take medication as frontline treatment (62.5% vs 45.5%), and have higher regimen complexity (25.0% vs 11.4%) compared to participants with inadequate understanding of OAM handling.
Access to OAM
Most participants received drug cost assistance (n = 41, 74.5%; Table 3). Among these participants, assistance came from a drug cost assistance program facilitated through the specialty pharmacist (n = 14), subsidized insurance (n = 20), or Medicare with low or no copay (n = 6). Prior authorization was required more often for participants with drug cost assistance (80.5%) than those without assistance (28.6%). Overall, only two participants reported problems with insurance when getting their OAM. Participants with drug cost assistance were more likely to report that their cancer team helped them figure out whether their OAM was covered by their insurance (28.6%) compared to those with no drug cost assistance (16.7%).
Access to OAM by Drug Cost Assistance.
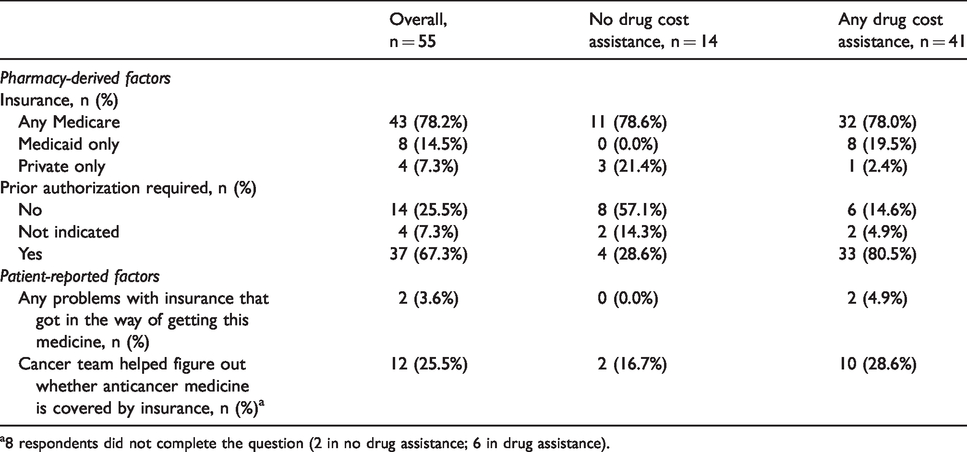
a8 respondents did not complete the question (2 in no drug assistance; 6 in drug assistance).
With regards to their most recent copay for their OAM, 38 participants (69.1%) had no copay, 14 participants (25.5%) had a copay between $1 and $25, with the remaining three having higher copays; the maximum was $3075. The three higher copays were all among participants without drug cost assistance. Among participants taking lenalidomide and enrolled in a drug cost assistance program facilitated by the specialty pharmacist (n = 6), their hypothetical median copay amount without the assistance would have been $1896, compared to the actual copay of $0. For ibruitinib (n = 3), the hypothetical copay amount would have been $404, compared to $0.
Discussion
Our institutional pilot study to assess understanding of and adherence to OAM included 55 patients from pre-specified vulnerable groups. Patients’ understanding of medication taking and handling was strikingly low, despite high levels of patient-reported adherence. Understanding tended to be higher among patients with more complex medication regimens. The majority of patients had drug cost assistance, which was reflected in low or no copays. However, a small subset of patients had high copays.
Less than one-third of patients had adequate understanding of how to take their OAM, and even fewer understood how to handle their OAM. Adequate understanding of taking and handling of their OAM is a key factor influencing adherence.7,31 Therefore, our findings of inadequate understanding are consistent with the low-end estimates of adherence and persistence (e.g., 16%, 42%) from prior reviews.5,8 The discrepancy between high levels of patient-reported adherence and inadequate understanding of taking and handling their medications was worrisome. If patients are unaware that they do not fully understand how their OAM should be taken, they may not be able to accurately report on their own adherence. 31 Furthermore, even if patients do understand how to take their medication, they may be susceptible to social desirability bias when reporting their own medication adherence. 32 Therefore, measures of adherence other than patient-report may be needed, such as pill boxes and pill counts, medication event monitoring (MEMS) caps, or medication fill information.9,33 Pill boxes, pill counts, and MEMS caps can prove challenging with OAM, which have special handling instructions, including storage or the use of gloves and not commingling with other oral medications. 34 In addition, they may require more frequent in-person visits. Medication fill information, including medication possession ratio, is another method of assessing adherence. 35 Although our study was restricted to medications filled at our specialty pharmacy, we could broaden our inclusion criteria if we were able to get information from outside pharmacies and/or insurers to allow calculation of medication possession ratio.
By targeting our study to include more vulnerable patients, defined by Chinese language, older age, and lower socioeconomic status, we may have included patients with lower levels of understanding than would be expected from the general population.11–16 These vulnerable patients may have also had more difficulty accurately assessing their own adherence. This may be especially true for Chinese patients, where lower levels of adherence may be partially explained by language and cultural barriers, as well as lower levels of educational attainment in our assembled sample.21–23,36 Programs to enhance OAM understanding and adherence should pay special attention to meeting the needs of vulnerable patients, which may vary by geographic region or practice setting. We hypothesized that understanding and adherence would be lower among patients with more complex regimens.9,37 For example, capecitabine is often taken twice daily for two weeks followed by a 1-week rest period, which could cause confusion for the patient. However, we found that patients with higher levels of understanding tended to be on more complex regimens and take multiple classes of OAM. Those with adequate understanding of taking were also more likely to have a chronic condition requiring medication management, while those with adequate understanding of handling tended to have a longer time since diagnosis, and be on OAM as frontline therapy. A variety of factors could explain these paradoxical findings. The clinical team or specialty pharmacist may spend more time with patients on complex regimens to make sure that patients understand how to take and handle the drug, perhaps assuming the lower complexity regimens do not require as much education. The clinical team may also only offer complex OAM regimens, or any OAM treatment at all, to patients who they think will be able to manage the medication at home. Incorporating more systematic education sessions for all patients initiating an OAM could help address these challenges. With regards to patients taking medications to treat their chronic condition, we collected whether patients were taking any medications besides the OAM, rather than an overall daily pill count. Some research shows increased pill count is related to lower adherence, but other research shows minimal relationship.38,39 Our results suggest that patients taking medications for a chronic condition have more experience managing their medications. Three-quarters of patients had drug cost assistance, which explains low copays overall and few patient-reported problems that prevented or delayed access to the OAM. Given that patients were from vulnerable subgroups, it is reassuring that most had few issues with access. However, a small subset of patients without drug cost assistance had high copays, with a maximum over $3,000. Patients who are treated at facilities without specialty pharmacists or PNs may not have access to drug cost assistance programs and may regularly face high copays. Patients included in this pilot were at different phases of their treatment, which could also influence copay amounts or perceived costs due to the lag between care delivery and payment. For example, patients on medications for longer may have reached their deductible, patients enrolled at the beginning of the year may be working towards paying down their deductible, or patients with Medicare Part D may be in the coverage gap (“donut hole”) of their benefits where there is more cost-sharing.40,41 In addition, some patients may only be on the OAM for a short time, particularly in the setting of subsequent therapy, while other patients may receive the OAM as chronic, frontline treatment (e.g., imatinib for chronic myelogenous leukemia). Interestingly, less than 30% of patients with drug cost assistance reported that the cancer team helped figure out whether an OAM was covered by insurance, despite some patients being in the program facilitated by the specialty pharmacist and many of the patients receiving medications requiring prior authorization. Many of these results demonstrate that not all patients were aware of the work done by the specialty pharmacist and pharmacy technician support staff behind the scenes, and some patients may be unclear of the role of the specialty pharmacist on their care team.
This pilot study has limitations. Not all patients completed all study measures; however, given that missing data were due to the start of the clinic visit, data should be missing completely at random and should not result in bias. Some, but not all of the study measures had been previously validated.28,29 However, the items included in the specialty pharmacist’s validation of patient understanding of taking and handling were based on a direct comparison between the prescription instructions and patients’ responses. In order to accurately capture copay amounts, only patients filling their OAMs at Tufts MC Cancer Center were included. In addition, patients who were on free drug programs directly with the pharmaceutical company were not captured. These two restrictions in the sample may influence to whom the results generalize and may reflect different experiences with access to OAM. Given the modest sample size, analyses are descriptive rather than hypothesis testing. Finally, generalizability of findings should be considered because only patients from a single medical center were included, which had a substantial proportion of Chinese patients.
In conclusion, this pilot study of 55 vulnerable patients on OAMs demonstrated many areas for improvement. Interestingly, our findings came after the development of the OAM Safety Initiative at Tufts MC Cancer Center, which had already incorporated ad hoc education sessions for some patients when initiating their OAM. Given the lifesaving potential and risk of side effects of OAMs, as well as the patients’ increased responsibility in managing their OAM, additional education and reinforcement is needed to ensure patients truly understand how they are supposed to take their medication.42–44 Practices that would like to improve patient understanding of and adherence to OAM should consider systematic teaching on administration and handling at medication initiation, periodic check-ins or reminders to confirm continued understanding, culturally- and language-congruent education, and objective methods for assessing adherence that do not rely only on patient self-assessment. As a result of this cross-sectional pilot study, we subsequently conducted a pilot longitudinal intervention study to investigate how to best deliver these education sessions in a systematic, rather than ad hoc basis. 26 Addressing these issues will maximize OAM safety and efficacy, allowing the full benefit on outcomes to be realized.
Footnotes
Acknowledgements
We would like to thank Daqin Mao, PhD, MS and Feng Qin Wang, BA for their assistance with recruitment; and Rachel Murphy-Banks, MA for her review of the manuscript. We would also like to thank John Erban, MD for his ongoing support of this work.
Data sharing statement
For original data, please contact
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Moore/Moreau Cancer Research Project Funding Opportunity (AMR); National Center for Advancing Translational Sciences, National Institutes of Health, Award Number 1KL2TR002545 (AMR); Yawkey Foundation (SKP).